

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Orthodontic treatment alone is not sufficient to resolve severe skeletal malocclusion. Orthopedic treatment in children and orthognathic surgery in adults are needed to overcome the skeletal discrepancy and improve facial esthetics. Orthognathic surgery for Class III malocclusion with mandibular prognathism is not recommended for growing children for posttreatment stability. However, relapse occurs occasionally even if surgery is performed in adulthood. Relapse after orthognathic surgery can be multifactorial1,2,3 including factors such as preoperative age of the patient4, amount of mandibular setback5,6, direction of bony fragment movement7, skill of the surgeon8,9, soft tissue and muscular tension10,11,12, quality of orthodontic treatment5,6, and postoperative orthodontic retention4.
Early relapse or short-term relapse, which occurs at 6-8 postoperative weeks, is mostly caused by movements at the osteotomy site or sagging of the temporomandibular joint (TMJ)2. It has been reported that proximal segment rotation during surgery was associated with instability after mandibular setback6,13. Kawamata et al.14 who evaluated the postsurgical condylar displacement at 3 to 6 months after mandibular osteotomy in Class III patients reported that changes in the inclination of the condylar axis were distinctly seen, although changes in the position of the condyles within the joints were minimal. Lee and Park15 investigated 30 Class III malocclusion patients who received sagittal split ramus osteotomy (SSRO) and reported that the condyle tends to move inferiorly and rotate inward on the axial view and backward on the sagittal view at 1 month after surgery. Ueki et al.16 also reported condylar rotation seen on horizontal axial images after surgery for mandibular prognathism.
Positional and angular change of the condyle could occur immediately after orthognathic surgery. The goals of postsurgical orthodontic treatment are to settle the occlusion on the new skeletal position and to cope with immediate skeletal relapse. However, if the condyle position is not stable at the time of bracket debonding, late relapse can be expected to occur. Jakobsone et al.17 reported that most of the relapse after the mandibular setback occurred during the first 6 months, but some relapse was also observed between 1 and 3 years postoperatively. According to a recent study by Ueki et al.18, the postoperative anterior joint space (AJS) was significantly larger than the preoperative value after assessment at 1 year after surgery in the 87 mandibular prognathism patients.
However, there is little evidence to determine whether the condyle position is stable or displaced at the time of debonding, and if there is a relation to late skeletal relapse. Most previous studies that investigated the change of condyle position focused on the surgical method and/or fixation type14,16,19,20, asymmetry18,21, one-jaw or two-jaw surgery6,20,22, and improvement of TMJ disorder16,22. However, these studies lacked a cephalometric analysis, and therefore could not provide information regarding skeletal relapse after removal of orthodontic appliances. Recently, in a study using a cone-beam computed tomography, Kim et al.23,24 reported that the condyle moved from the anterior to the concentric position after surgery and tended to return slightly toward the original position at 17 months after surgery. They also concluded that these changes did not negatively affect the skeletal stability. However, in their studies, the relationship between the condylar position at debonding time and skeletal relapse during the postretention period could not be clearly explained. This is due to the fact that the statistical mean applied in their studies is highly misleading as an expectation of treatment response. The best way to represent the data is in terms of percentage of the patients who showed a stable result or relapse25. The purpose of this study was to investigate the positional change of the condyle after orthodontic-orthognathic surgery treatment and the relationship with skeletal relapse.
II. Materials and Methods
Samples were selected from patient records who received orthodontic-orthognathic surgery treatment at Gangneung-Wonju National University Dental Hospital from 2004 to 2009. Samples used in this retrospective study were TMJ tomograms taken before treatment (T1) and immediately after the removal of the orthodontic appliances (T2), and lateral cephalograms at T1, T2, and at the retention period (T3). Inclusion criteria were as follows: (1) patients who had mandibular prognathism and received mandibular set-back surgery with SSRO, (2) patients with no TMJ disorders before treatment, (3) patients successfully treated with normal overjet and occlusion, and (4) patients with good quality of TMJ tomograms at T1 and T2, and cephalograms at T1, T2, and T3.
Finally, tomograms and cephalograms of 19 patients were selected for the present study. Seven patients received only mandibular set-back surgery and 12 patients received bimaxillary orthognathic surgery. The protocols of this study were approved by the Ethics Committee of the Gangneung-Wonju National University Dental Hospital (IRB 2010-1-3).
1. Cephalogram analysis
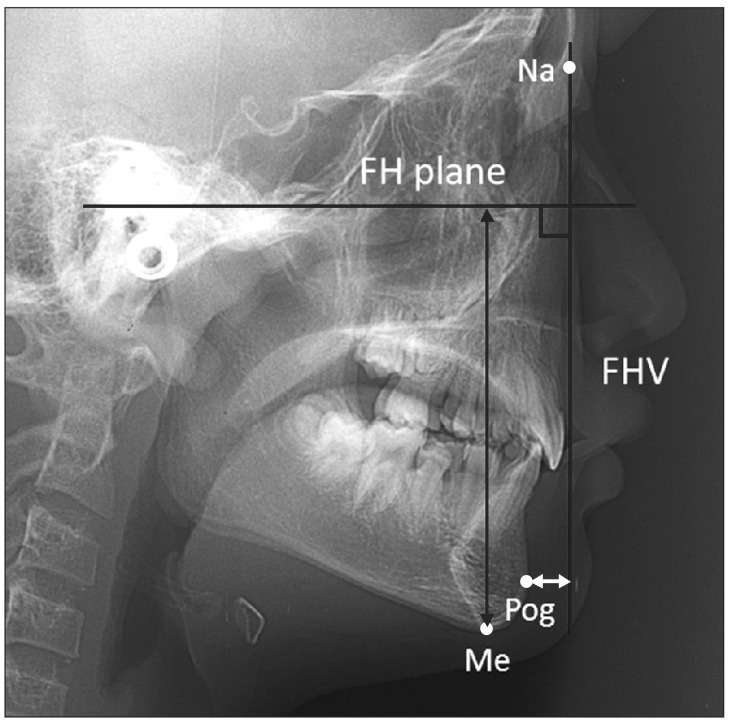
Lateral cephalograms taken in the habitual occlusion with the CX-90SP (Asahi Roentgen Industries Co., Kyoto, Japan) were traced on acetate paper to obtain measurements. Cephalograms at T2 and T3 were superimposed on sella-nasion line at sella. The distance from the menton (Me) to Frankfort horizontal (FH) plane, and the distance from pogonion (Pog) to the vertical reference line passing nasion and perpendicular to FH plane (FHV) were measured.(Table 1, Fig. 1) All measurements were read to a 0.01 mm scale and the radiographic magnifications (110%) were corrected to 100%.
Patients were divided into stable and relapse groups. The patients who showed skeletal changes more than 1 mm in the distance of Me to FH and/or Pog to FHV between T2 and T3 were classified in the relapse group. The relapse group consisted of 7 patients (3 females and 4 males; mean age, 21.9 years). The stable group consisted of 12 patients (5 females and 7 males; mean age, 21.7 years). Sample description and mean duration of the record is summarized in Table 2.
2. TMJ tomogram analysis
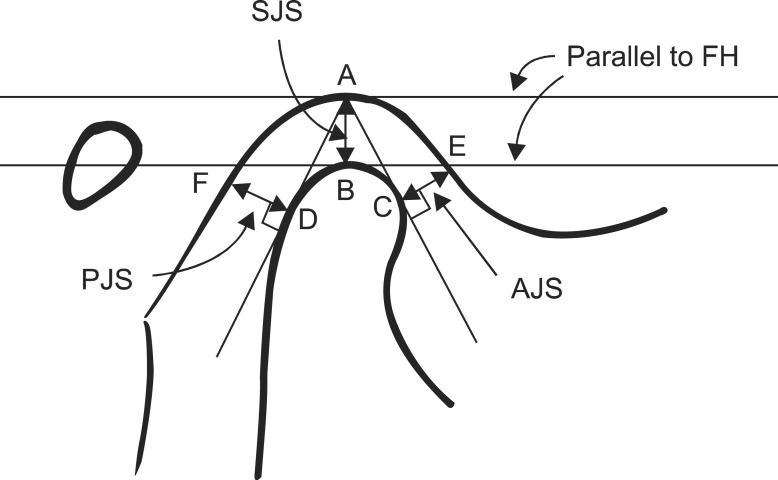
Individualized corrected TMJ tomogram was taken using CommCAT IS-2000 (Imaging Sciences International, Hatfield, PA, USA) while maintaining the FH plane of the patient parallel to the horizontal plane. To determine the long axis of the mandibular condyle, submentovertex radiography was used. The selected sections of the tomogram were traced using acetate paper and pencil. The distance of the condyle to the temporal fossa was measured in the AJS, posterior joint space (PJS), and superior joint space (SJS) as described in Fig. 2.
Measurements were read at the 0.01 mm scale and the radiographic magnification (126%) was corrected. Anteroposterior index (API) was calculated to define the position of the condyle to the temporal fossa as reported by Pullinger and Hollender26.
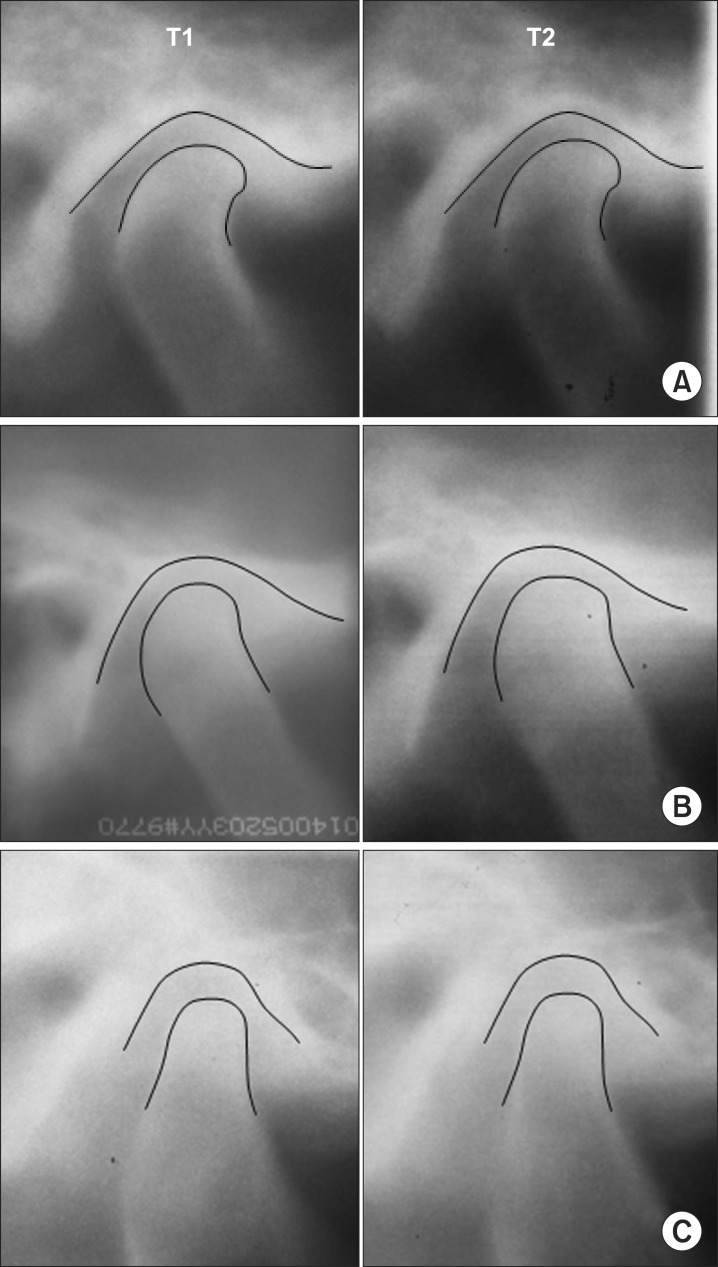
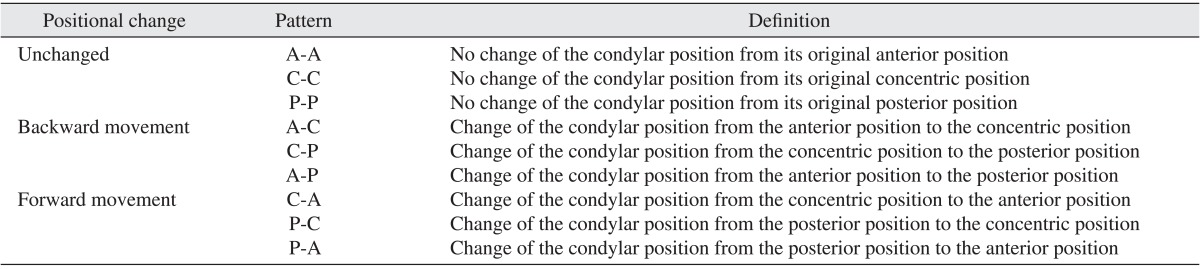
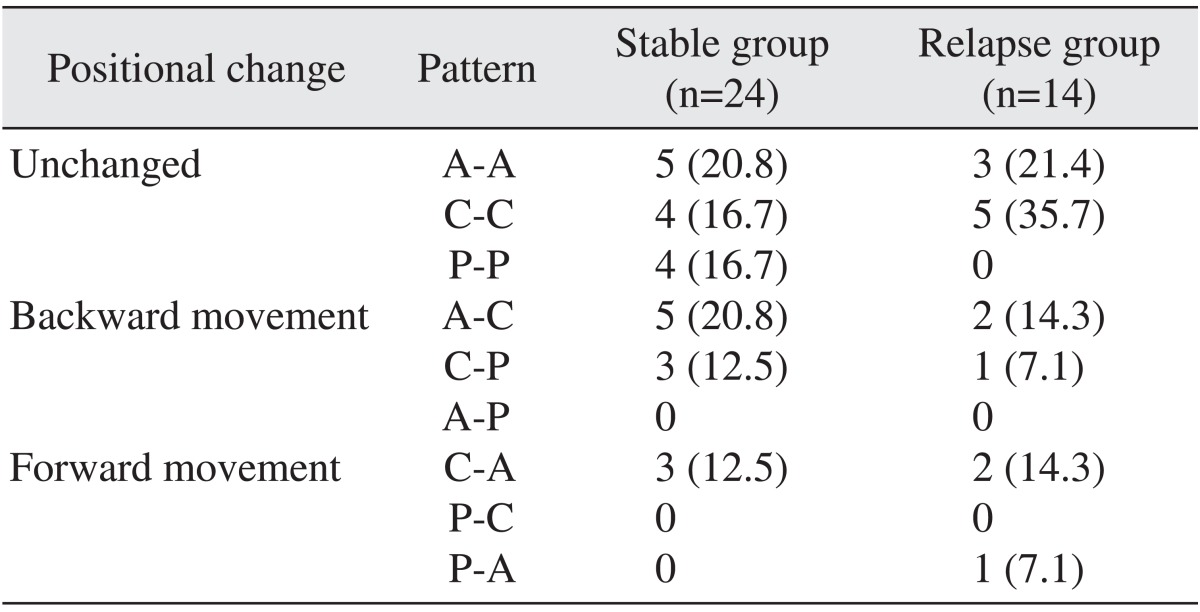
API between -12 and +12 was defined as concentric position, more than +12 as anterior position, and less than -12 as posterior position. Positional change of the condyle between T1 and T2 was classified as unchanged, backward displacement, and forward displacement as described in Table 3. Three different patterns of condyle change are shown in Fig. 3.
3. Statistical analysis
Normal distribution of the measurements was confirmed by the Shapiro-Wilk test. Because the measurements did not show normal distribution, nonparametric tests were used. The Mann-Whitney U test was used to verify the difference between the two groups. Spearman correlation analysis was used to determine the relationship between skeletal relapse and condylar changes. Additionally, the chi-square test was used to determine differences in the frequency of the pattern of condylar positional change between the groups. The statistical significance was determined at the 5% level of confidence. All statistical analyses were performed with IBM SPSS Statistics 20.0 (IBM Co., Armonk, NY, USA).
III. Results
Table 4 shows the group differences in the skeletal changes during the retention period (T3-T2). The Pog to FHV and Me to FH was not significantly different at posttreatment (T2) between the groups. However, the mean absolute value of the difference of Pog to FHV (T3-T2) was 0.6 mm in the stable group and 1.2 mm in the relapse group. The Me to FH (T3-T2) was 0.5 mm in the stable group and 1.2 mm in the relapse group.
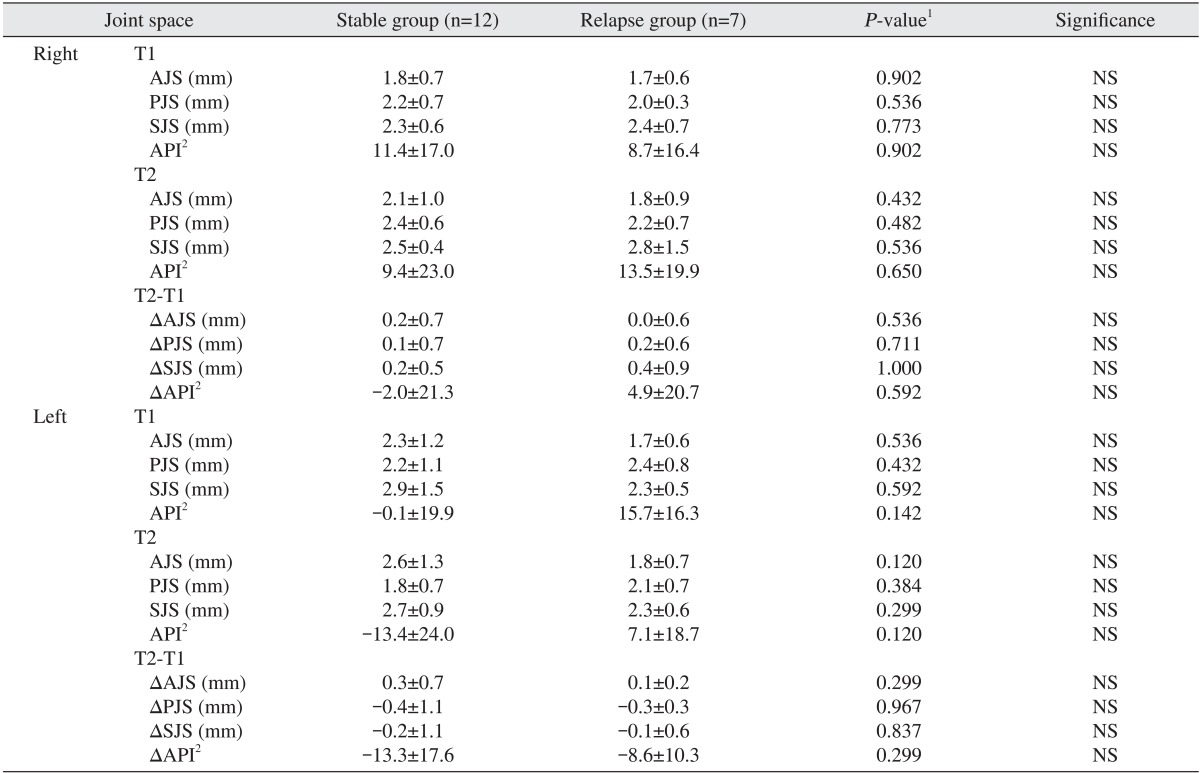
Table 5 shows the distance of the joint space (AJS, PJS, SJS) and API of the stable group and the relapse group at T1 and T2. The position of the condyle was generally concentric to the glenoid fossa. Although the API of the left condyle indicated a slight anterior position at T1 in the relapse group (API=15.7) and slight posterior position at T2 in the stable group (API=-13.4), the difference was not statistically significant between the groups (P>0.05).
Table 5 also shows a change of the joint space from T1 to T2. Negative values of API mean backward displacement of the condyle to the glenoid fossa. The condyles of the left side showed slight backward movement from T1 to T2 in both groups. However, the change of the condyle position was not significantly different between the groups (P>0.05).
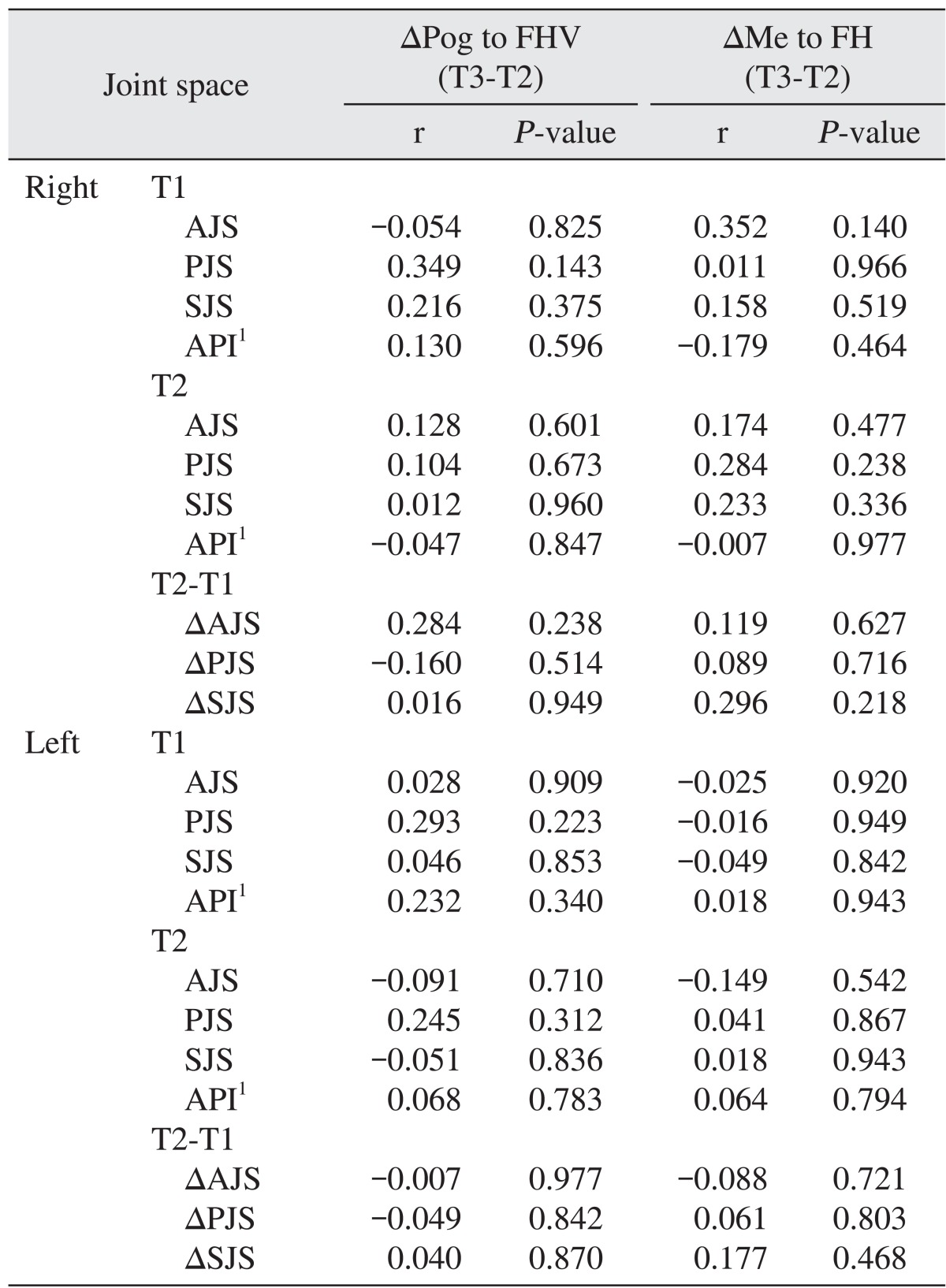
In the Spearman correlation analysis, no correlation was found between the change of chin position during the retention period and the position of the condyle at T1 and T2 (P>0.05).(Table 6)
The frequencies of the positional change of the condyle from T1 to T2 are shown in Table 7. The positions of 13 out of 24 condyles (54.2%) in the stable group and 8 out of 14 condyles (57.1%) in the relapse group were not changed from their original position after treatment. Backward movement occurred in 8 condyles (33.3%) in the stable group and 3 condyles (21.4%) in the relapse group, and patterns were A-C and C-P. There was no A-P pattern with backward changes. Forward movement occurred on 3 condyles (12.5%) in the stable group and 3 condyles (21.4%) in the relapse group. One P-A pattern of condyle movement was observed in the relapse group. No P-C patterns of condyle movement were found. The chi-square test, however, showed that frequencies of the pattern of positional change of the condyle were not statistically different between the groups (P=0.438).
IV. Discussion
Among the many factors affecting relapses after orthognathic surgery, we focused on the condyle position after bilateral SSRO for the mandibular set-back and evaluated the relation between condyle position and skeletal relapse. The preoperative age of the patients, A point-nasion-B point (ANB) angle, chin position at T1, and amount of mandibular set-back did not significantly differ between the stable group and the relapse group (Tables 2, 3), which means sample homogeneity between both groups. However, a different duration of the records (T1-T2 and T2-T3) between both groups and large standard deviation can be considered a weak point of this study, although the statistical evaluation showed no significance. It is interesting that the relapse group showed longer post-surgical orthodontic treatment than the stable group.
Some statistic measurements can be misleading, as true relapse can occur only in some cases and significant results can be distributed among groups. Proffit et al.7 reported that in both the postsurgical and posttreatment periods, almost all changes occur in a minority of patients, so it is better to consider the percentage of patients with clinically significant changes than to compare the mean value of the differences. Using ANOVA to analyze means, it can be concluded that not grouping according the treatment response is a potential weak point of previous studies23,24 on the long-term evaluation of the condyle change and skeletal stability. In the present study, we divided the samples based on treatment response, such as stable group and relapse group, and therefore a change of the condyle could be evaluated in both groups respectively. However, the mean positional change of the condyle was not different between the groups. In the chi-square test, the frequencies of the changing pattern did not differ between the groups.
In the present study, we could not find any relationship between the positional change of the condyle after orthodontic-orthognathic surgery treatment (T2-T1) and skeletal relapse during the retention period (T3-T2). One reason for a failure to identify a relationship may be the small sample size in the relapse group and severe criteria to define an episode of relapse. Only 1 out of 7 patients showed more than 2 mm at the distance of the Me to FH plane, while the other 6 patients included in the relapse group showed a small change of the chin area (range: 1 to 2 mm). Other classifications based on larger skeletal relapse may indicate significant differences between the stable and relapse groups. In the present study, however, it was difficult to collect relapse samples showing skeletal relapse more than 2 or 3 mm during the retention period that satisfied the inclusion criteria. Therefore, our results should be interpreted cautiously only in patients showing small skeletal relapse during retention periods.
In the relapse group, the number of patients with forward, backward, downward, and upward movement of the chin between T2 and T3 was 5, 1, 2, and 2 patients, respectively. In the present study, we could not investigate the results according to the subdivision based on the direction of skeletal relapse due to the small sample size. In future research, detailed classification based on the direction of skeletal change and a less strict definition of skeletal relapse may be needed to clarify the association between the positional change of the condyle and skeletal relapse.
It is interesting that approximately half of the condyles still showed forward or backward displacement at the posttreatment timepoint in both groups (45.8% for stable group and 42.8% for relapse group), even though 7 to 10 months on average of postsurgical orthodontic treatment was applied.(Table 7) Moreover, diverse patterns of positional change were observed. Many researchers also reported that condyle position changes on occasion after orthognathic surgery27,28,29 and maintaining the condylar position in its own position after orthognathic surgery is very important to reduce relapse and the risk of TMJ disorders30,31,32,33. To prevent positional changes of the condyle after surgery, several condylar positioning devices have been proposed, but use of condylar positioning devices did not provide better functional and long-term outcomes8,34. By this reasoning, most surgeons still rely on empirical methods to reposition the mandibular proximal segment during SSRO to obtain the most favorable condylar position8,9,35.
Ueki et al.9 concluded that the most favorable postoperative condylar position may not match the preoperative one, but would not be dramatically different except for cases of temporomandibular disorder (TMD) or asymmetry. In the ideal postoperative position of the condyle, remodeling of the TMJ induced by postoperative biomechanical stress would be small9,36,37. Kim et al.23 concluded that physiologic adaptation can accommodate small changes in the condylar position and this would be followed either by later skeletal relapse or condylar remodeling. Regarding specific manifestations of TMD signs and symptoms, this depends on the individual physiologic adaptation capacity of the patient. All patients in the present study did not show any TMD signs or symptoms after orthognathic surgery and during follow-up periods.
In the present study, we could not evaluate the condyle position immediately following orthognathic surgery and postretention period because TMJ tomograms were not taken at that time due to exposure to radiation and high cost. Therefore, it is unclear whether the condylar position changed during the postretention period in the relapse group. Additionally, mixed samples, including 2-jaw and 1-jaw surgery and possible residual mandibular growth after orthognathic surgery, might affect the results of this study. The possibility of rotation of the proximal segment, which can occur after orthognathic surgery, and its relation to late skeletal relapse after removal of orthodontic appliances remains to be investigated.
V. Conclusion
The present study investigated the condyle position of the patients who received orthodontic-orthognathic surgery for mandibular prognathism and compared it between stable and relapse groups.
More than 40% of the condyles showed positional change at posttreatment (T2) in both stable and relapse groups.
However, the changes of the condyle position (T2-T1) were small and did not statistically differ between stable group and relapse group.
Our results suggest that small positional changes of the condyle, which may occur after orthodontic-orthognathic surgery, are not related to skeletal relapse after removal of orthodontic appliances.



 XML Download
XML Download