

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Alveolar bone graft is essential in severe atrophic ridge for dental implant but is difficult in many cases due to soft tissue deficiency following alveolar bone atrophy, necessitating soft tissue graft prior to hard tissue bone surgery. Note, however, that this is a very challenging, technique-sensitive procedure.
In general, the advantages of tissue expanders are safeness of material, low complication rate, low risk of infection, small incision, minimal trauma, and short surgical time. In particular, the short surgical time can reduce post-operative pain and save on cost.
The use of self-inflating hydrogel tissue expander (Cylinder Dental, Osmed GmbH, Ilmenau, Germany) prior to the vertical augmentation of resorbed edentulous ridges may reduce the mean incidence of post-operative graft exposition from 25% to 4%, increasing the mean vertical bone gain from approximately 4.0 mm to 7.5 mm compared to augmentations without prior tissue expansion1.
The combination of soft tissue expansion and subsequent vertical augmentation provided high gain of well-structured bone for further successful implant therapy, accompanied by minimal complications1.
In the cases reported herein, we achieved soft tissue augmentation using self-inflating oral tissue expander and hard tissue augmentation with mixed bone graft result in a successful surgery.
II. Cases Report
1. Case 1
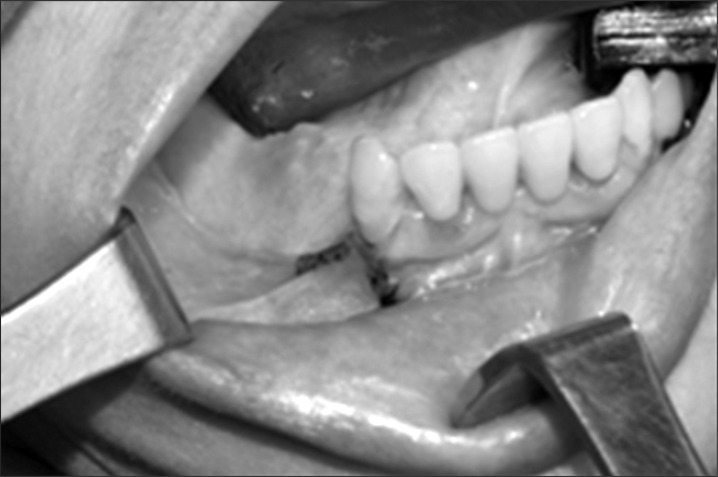
A 48-year-old female patient was diagnosed with severe bone resorption after peri-implantitis and removal of her previous 3 implants for tooth loss due to periodontitis. Three new implants were planned for rehabilitation. First, she needed vertical bone augmentation and soft-tissue expansion due to severely resorbed ridge.(Fig. 1)
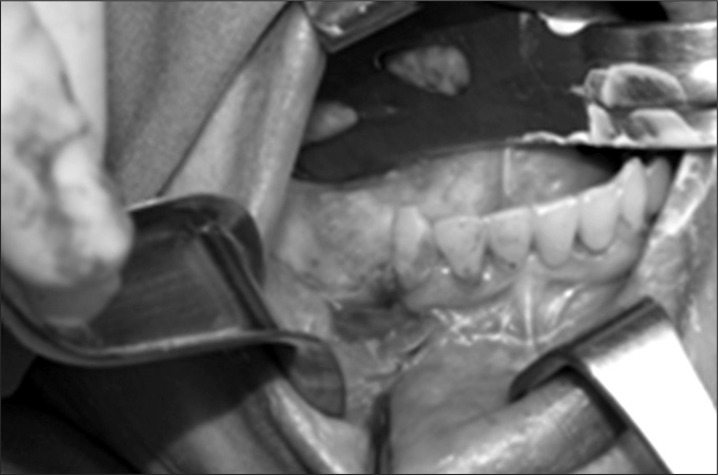
Osmed tissue expander (cylinder type, 0.15 mL) was inserted subperiosteally in the region of the lower right posterior area and fixed with 1 micro screw (Jeil self-tapping mini screw, 1.4×3 mm, Jeil Medical Corp., Seoul, Korea) under local anesthesia with lidocaine (2% Lidocaine HCL, Epinephrine Inj., Yuhan Corp., Seoul, Korea) and midazolam (Midazolam 5 mg/5 mL, Bukwang Pharmaceutical Co., Seoul, Korea) intravenous sedation.(Fig. 2)
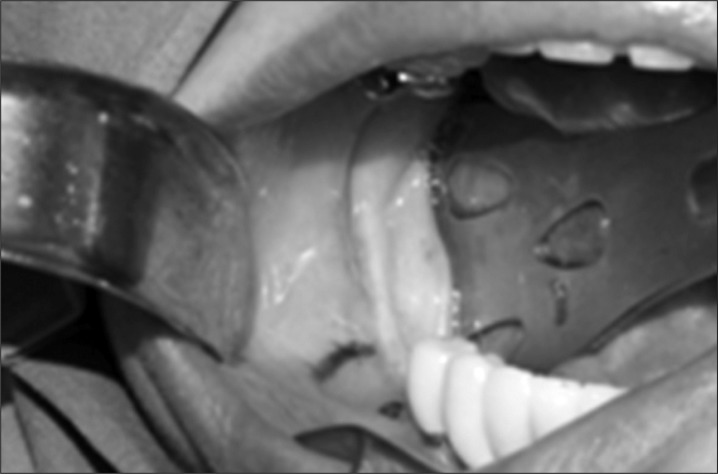
The tissue expander was left in place for 6 weeks and expanded from 0.15 mL to 0.7 mL. After bony augmentation with composite bone graft (autogenous bone [harvested from right ramal area]+xenograft [Bio-Oss; Geistlich, Wolhusen, Switzerland]), tension-free coverage of the augmented bone was achieved using the soft tissue that had been created. The tissue expander was used because of the firmness of soft tissue. Six months later, the grafted bone was very hard and intact. When implant surgery was done, insertion torque was 25 Ncm; currently, the operation site is healing following prosthetic treatment.(Fig. 3)
2. Case 2
A 54-year-old female patient was diagnosed with severe bone resorption on the right mandibular posterior area. The patient wanted to have 3 more implants for right-side molar rehabilitations. Bone graft and new implants were planned, but the vertical height of the remaining alveolar bone was low and close to the inferior alveolar nerve canal, posing a limitation in implant surgery.(Figs. 4, 5)
First, the insertion of tissue expander was performed for soft tissue augmentation. Buccolingual incision to secure a pouch was done, and Osmed tissue expander (cylinder type, 0.045 mL) was inserted and fixed using screw fixation.(Fig. 6)
The expander was left in place for 3 weeks and expanded from 0.045 mL to 0.24 mL.(Fig. 7)
Nerve repositioning surgery for inferior alveolar nerve repositioning was done during implant surgery. Simultaneous implant surgery was done after autogenous and xenogenic bone graft and tension-free soft tissue coverage using self-inflating tissue expander.
One and a half years after the operation, the inserted dental implant and expanded soft tissue healed well. In the neurologic examination, the sensory of the lower right lip was improved, and periodic follow-up was done with no complaints from the patient.(Fig. 8)
III. Discussion
This research reviewed 2 cases of soft tissue augmentation using Osmed self-inflating tissue expander in patients who initially visited the Department of Oral and Maxillofacial Surgery at Ewha Womans University Mokdong Hospital for bone graft and implant operation.
Primary wound closure is essential for the successful re-gene ration of bone. Soft tissue dehiscence and subsequent expo sure of bone grafts to the oral cavity are complications of ridge augmentation and are the main cause of the insufficient outcomes of reconstructive surgery. The main reasons for graft exposure are poor quality and quantity of soft tissue and difficulties in achieving primary closure of the flap. The wound should be closed primarily without tension so that vascularization is not compromised2.
Invented by Neuman in 1957, the tissue expander has been used for maxillofacial lesion wherein soft tissue is insu-fficient. It has been mainly used by the Department of Plastic Surgery since 19763. In 1982, interest in tissue expansion in reconstructive surgery was revived by a description of tissue expander in breast reconstruction4. In dentistry, tissue expander is used prior to bone graft in defective soft tissue areas and for the reconstruction of excision sites in cancer patients, albeit selectively.
Tissue expansion improves the quality and quantity of soft tissue and facilitates primary wound closure. Closure of the flap is more easily achieved in bone graft surgery. The osmotic soft tissue expander creates a surplus of periosteum and soft tissue, which can be used to cover bone grafts5.
Tissue expansion reduces the incidence of wound dehi-scence and exposure of bone grafts. In patients with substantial bone resorption, the technique allows tension-free wound closure over the augmented bone without periosteal incision6.
A novel self-inflating hydrogel tissue expander and its biomaterial were previously described, paving the way for the Osmed tissue expander7. The self-inflating device consists of osmotic active hydrogel, copolymer of methylmethacrylate, and vinylpyrrolidone5.
The volume of oral tissue expander used in this case report was 0.15 mL for Case 1 and 0.045 mL for Case 2. The expansion period was 6 weeks and 3 weeks, respectively, based on the manufacturer's guide. Soft tissue expansion was observed clinically after surgery, enabling graft of hard tissue and surgery of dental implant.
A limitation of the self-inflating tissue expander is the difficulty in the fixation of tissue expander in the initial position. In movable soft tissue such as non-attached gingiva in particular, it is difficult to maintain fixation and to expand soft tissue; hence the possibility of bursting. In addition, it is difficult to control the volume or degree of expansion and predict soft tissue expansion.
Later, a selection guideline for predictable material accor-ding to the expansion of the self-inflating tissue expander is essential.
In conclusion, the self-inflating tissue expander can used for atrophic alveolar bone and contractured soft tissue due to repeated surgery; thus enabling closing the primary wound after hard tissue graft using soft tissue expansion.





 XML Download
XML Download