

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Condylar dislocations commonly occur in association with a mandibular fracture as a result of facial trauma, and its displacement is commonly anterior rather than posterior, lateral, or superior. Condylar dislocations with combined direction of displacement have often been misdiagnosed or entirely neglected due to their extremely rare occurrence. Such is the case of superior-lateral dislocations. According to Yoshii et al.1, clinicians should bear in mind the possibility of an unusual condylar dislocation whenever the signs, symptoms, and clinical courses are not typical of common mandibular fracture. In this paper, we present an unusual case of lateral dislocation of the intact mandibular condyle with symphysis fracture and describe a method of reduction using bone-traction hook.
This study was approved by the local Ethics Committee of the Dental College Hospital of Yonsei University, Seoul, Korea, after obtaining written consent from the patient.
II. Case Report
A 54-year-old man visited Yonsei University Health System with four-day history of maxillofacial trauma. During the injury, he was under the influence of alcohol; he only recalled being hit with a falling luggage from a passing truck before landing on the ground. He did not experience loss of consciousness or vomiting. Before he was referred to the Department of Oral and Maxillofacial Surgery, the severity of his injuries was evaluated at the emergency room. The medical history revealed controlled diabetes mellitus and hypertension. During the physical examination, limitation of mandibular movement, unfavorable occlusion, tenderness to palpation of chin and bilateral temporomandibular joints (TMJ), and bony prominence in both preauricular regions were observed. The panoramic radiograph and three-dimensional computed tomography (3D CT) showed fracture of the symphyseal region and dislocation of both condyles. The 3D CT clearly revealed the evident lateral displacement of the left condyle; the right condyle was severely dislocated laterally from the glenoid fossa and engaged over the lateral surface of the zygomatic arch. The bilateral condyles and zygomatic arches were intact and were not fractured.(Fig. 1)
The patient was hospitalized and immediately transferred to the operating room. Under general anesthesia via nasal intubation, manual reduction of the bilateral condyle dislocation was attempted, to no avail. Bone traction hook was placed at the sigmoid notch through stab incision, and reduction was finally achieved after applying outward traction.(Fig. 2) Open reduction and internal fixation of the mandibular symphysis fracture were done with self-reinforced, biodegradable poly-70L/30DL-lactide plates and screws. The mandible was placed into the intermaxillary fixation (IMF) with IMF screws and elastics for seven days. Intensive jaw physiotherapy was instituted for one month. We instructed the patient to open his mouth to the maximum extent possible and move anteriorly/laterally.
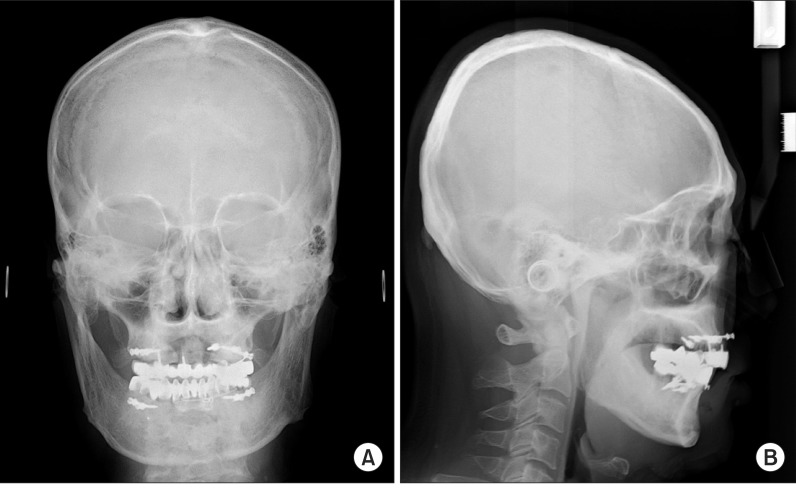
Lateral and posterior-anterior cephalographic images were obtained during the first post-operative day and month. All images verified the position of the bilateral dislocated condyles into the glenoid fossa and reduction of symphysis fracture. Even though the right condyle seemed to be displaced slightly laterally (Fig. 3), mouth opening was found to be within normal limits, and favorable occlusion was confirmed. No symptoms of TMJ disorder were observed. Unfortunately, the patient was not cooperative, and long-term follow-up could not be performed.
III. Discussion
Although PubMed database listed 23 cases published between 1969 and 20111-17, there were few reports of superior-lateral dislocation of intact mandibular condyle. Medial pulling of the pterygoid muscles during impact on the face may partly contribute to the rarity of condylar lateral displacement13. According to Amaral et al.17, maxillofacial trauma associated with superior or lateral dislocation of the intact mandibular condyle is more predominant among young male adults who have figured in a road traffic accident.
Allen and Young2 classified the lateral dislocation of the mandibular condyle into two types: type I (lateral subluxation), wherein the condyle is laterally displaced from the fossa; and type II (complete dislocation), wherein the condyle has been dislocated both laterally and superiorly as it enters the temporal fossa. Satoh et al.8 further subdivided type II dislocation into three subcategories: type IIA, wherein the condyle is not hooked above the zygomatic arch; type IIB, wherein the condyle is hooked above the zygomatic arch; and type IIC, wherein the condyle is lodged into the zygomatic arch. The present case fits the criteria of right-type IIB and left-type I mandibular condyle dislocations.
Amaral et al.17 pointed out that high energy of trauma could induce this type of dislocation and anterior mandibular fractures. According to Allen and Young2, in such cases, there was always a history of trauma to the chin usually associated with fracture in the symphyseal region. The related mandibular fracture obviously promoted the rotation and movement of the ramus, which would facilitate the superior or lateral dislocation of the condyle as observed in the current case and previously reported cases2,6-9,11,13,17. As described by other authors, however, intact mandibular condyle dislocations may also occur occasionally without traumatic fractures5,12,14,16.
Among the treatment options for intact condyle dislocations, manual reduction is the simplest, least traumatic, and safest1,12,18. Nonsurgical methods such as traction wire placed at the angle of the mandible6,9 or mouth props--functioning as fulcrum--placed in the molar region12 have been previously used. According to the literature review, however, open reduction was selected for treating 52.2% of the cases, whereas closed reduction was carried out in the remaining 43.5%1-17. Reduction was not completed in one case11. The higher rates of open reduction may be correlated to the waiting time for treatment17. Delay in treatment may cause fibrosis of the glenoid fossa, resulting in incomplete reduction. The formation of fibrous tissue can make manual reduction impossible12. In the present case, the patient visited the emergency room four days after the trauma, and manual reduction under general anesthesia was unsuccessful. To our knowledge, this is the first reported case of type IIB dislocation reduced with the aid of bone traction hook. By modifying the approach of close reduction, we were able to impose strong traction, disengage the condyle from above the zygomatic arch, and relocate both condyles to their normal positions. Despite the radiographic evidence of slight lateral displacement of the right condyle in the postoperative posterior-anterior cephalographic image (Fig. 3), the patient did not manifest any discomfort or mouth opening limitation.
In summary, superior or lateral dislocation of the intact condyle is often neglected yet requires thorough physical and radiographic examinations. Early diagnosis and management are strongly emphasized because prolonged dislocation can make reduction more difficult, leading to unsatisfactory results. Manual reduction is the first treatment option for superior-lateral condylar dislocations; in delayed cases, however, open reduction or application of strong traction force by means of an extraoral route--bone traction hook, for example--is highly recommended in this case report due to its favorable outcome.


 XML Download
XML Download