

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
The primary goal in the treatment of temporomandibular joint disorder (TMD) is to ease pain or mandibular dysfunction1. TMD treatment can be divided into two categories: conservative method and surgical method. Conser vative treatments include medication, habit modifi cation, counseling, physical therapy, splint therapy, and manipulation2. Surgical treatments include arthrocentesis, arthroscope, arthroplasty, discectomy, and temporomandibular joint (TMJ) reconstruction3. A conservative, reversible method is widely accepted to be the first choice for TMJ treatment4. As one of the conservative treatments, occlusal splint has been frequently used for internal derangement and myofascial pain treatment. As for the mechanisms of occlusal splint therapy, wearing an occlusal splint is considered to cause alterations in mechanical sensitive input arising from periodontal tissue and spindle afferents in the jaw closing muscle5 and decrease in intra-articular pressure in TMJ6.
Occlusal splint is often successful, but the length of time required to reach a pain-free normal range of motion is suboptimum7.
Among the surgical interventions, arthrocentesis is generally suggested for patients who are not responsive to conservative therapy8. Arthrocentesis is an easy, minimally invasive, highly efficient procedure designed to decrease joint pain and increase the range of mouth opening in patients with closed lock of TMJ9. In fact, it has recently been proposed as a first-line treatment in disc displacement without reduction10.
To date, studies on occlusal splint only, arthrocentesis only, and combined treatment of occlusal splint and arthrocentesis have been conducted. Studies comparing those treatments are rare, however.
This study sought to test the hypothesis that the simultaneous use of occlusal splint and arthrocentesis is an effective method for anterior disc displacement without reduction. A retrospective comparative study was conducted to investigate the therapeutic effect of the simultaneous application of arthrocentesis and occlusal splint, arthrocentesis after occlusal splint use, and use of occlusal splint only.
Go to : 
II. Materials and Methods
1. Patient collection and definitions
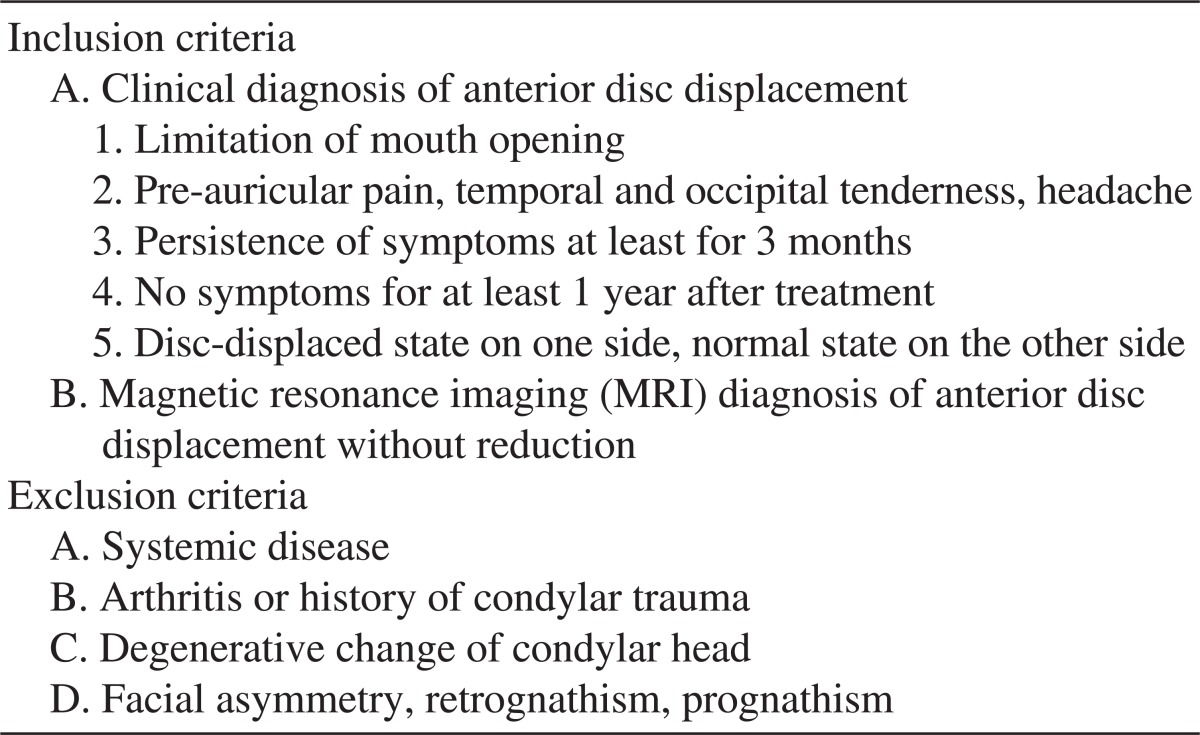
A retrospective study targeting 43 patients (3 males, 40 females) whose records were completely preserved and whose symptoms had improved was conducted at the Department of Oral and Maxillofacial Surgery, Dong-A University Hospital between 2008 and 2010. All patients were diagnosed with anterior disc displacement without reduction based on MRI. The inclusion and exclusion criteria are shown in Table 1.
The study was conducted after obtaining approval from the Institutional Review Board of Dong-A University Hospital (12-060).
2. Treatment groups
A total of 43 patients were divided into 3 groups: 17 in group A, 13 in group B, and 13 in group C.
Group A: Patients who underwent the simultaneous application of arthrocentesis and occlusal splint.
Group B: Patients whose symptoms did not improve with the use of occlusal splint, so they underwent arthrocentesis after occlusal splint use for 8 weeks.
Group C: Patients who only used occlusal splint.
3. Outcome measures
Visual analog scale (VAS) (0-10) was used for pain and noise assessment. VAS is considered to be a reliable, effective method for evaluating TMJ pain11. Zero indicates no pain, whereas ten means severe pain. Maximum comfortable opening (MCO) was measured between the edges of the upper and lower central incisors by a millimeter ruler. The success criteria for surgery for TMJ internal derangement have been proposed by American Association of Oral and Maxillofacial Surgeons (AAOMS)12: absence of or mild pain, range of motion of more than 35 mm for vertical.
We evaluated the period of achieving normal states among the groups. Normal state is said to have been achieved if the following requirements are satisfied: (1) VAS score for pain was less than 3 (pain<3); (2) MCO was more than 38 mm or MCO increase was more than 10 mm (MCO≥38 [or 10]); (3) Pain<3 and MCO≥38 (or 10). For Group A, follow-up check was performed at 1 week, 1 month, 3 months, and 6 months after arthrocentesis. In groups B and C, however, follow-up check was performed at 1 week, 1 month, 3 months, and 6 months after occlusal splint installation.
4. Arthrocentesis and splint therapy
Impression taking for occlusal splint was performed on the day of diagnosis in group A. One week later, group A wore full-coverage, hard acrylic stabilizing splint on the maxilla, and arthrocentesis was performed on symptomatic TMJ. On the other hand, impression taking for occlusal splint was performed on the day of diagnosis in group B. One week later, group B wore full-coverage, hard acrylic stabilizing splint on the maxilla. The occlusal splint was used for a mean of 8 weeks prior to arthrocentesis. Finally, impression taking for occlusal splint was performed on the day of diagnosis in group C. For all the groups, appropriate doses of diazepam and non-steroidal anti-inflammatory drugs (NSAIDs) were administered for pain control for one week. If patients complained of pain during treatment, they were prescribed an additional medication for one week. Patients were instructed to wear their splint the whole day except mealtimes.
Arthrocentesis was performed on all patients in groups A and B using the technique described by Nitzan et al.13 Two points were marked over the skin of the affected joint indicating the articular eminence and articular fossa. This was followed by the injection of a local anesthetic to block the auriculotemporal nerve14,15. A 23-gauge needle was inserted into the superior compartment at the articular fossa (posterior mark), followed by the injection of 2-3 mL of lactated Ringer's solution to distend the joint space. An 18-gauge needle was then inserted into the distended compartment in the area of articular eminence to enable free flow of the solution through the superior compartment. The lactated Ringer's solution was connected to one of the needles. Sufficient pressure was secured by placing the infusion bag at an elevation of 1 meter above the level of the joint. During the procedure, the patient repeated maximum mouth opening, protrusion, and lateral movement. Upon the termination of the procedure, 2 mL (20 mg) hyaluronic acid (Hyruan plus; LG Life Sciences, Seoul, Korea) was injected into the joint space followed by the removal of the needles. Postoperative medication consisted of antibiotics thrice daily for 3 days and NSAIDs thrice daily for 7 days.
5. Statistical analysis
Data were analyzed using the PASW ver. 18.0 for Win (IBM Co., Armonk, NY, USA). Descriptive analyses were used to illustrate the characteristics of the participants. We assessed the assumption of sampling distribution such as normality before statistical analysis, but the hypothesis for normality was not met. Therefore, we conducted variables log transformation. In evaluating the statistical significance of pain, MCO, and noise changes within group, repeated measure of ANOVA and ANOVA test with Bonferroni's post hoc test were conducted. A P-value of α<0.05 was considered to be statistically significant.
Go to :
III. Results
1. Demographic data
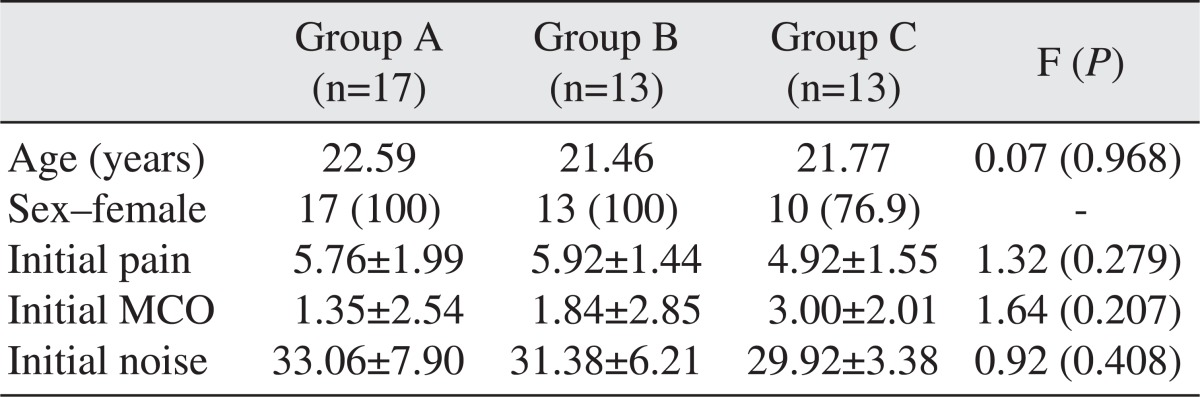
Patients numbered 43 (males: 3; females: 40). The mean age in each was 22.59 (group A), 21.46 (group B), and 21.77 (group C) (F=0.07, P=0.968). There were no statistical differences among the three groups in terms of baseline pain (F=1.32, P=0.279), MCO (F=1.64, P=0.207), and noise (F=0.92, P=0.408).(Table 2)
2. Descriptive data on pain, MCO, and noise
The descriptive data for pain, MCO, and noise in each group are presented in Table 3. The baseline mean VAS scores for pain for group A, group B, and group C were 5.76, 5.92, and 4.92, respectively. After treatment, there was a reduction in the mean VAS for pain in all groups, with group A, group B, and group C recording 1.38, 1.73, and 2.00, respectively, at the follow-up check after 6 months.
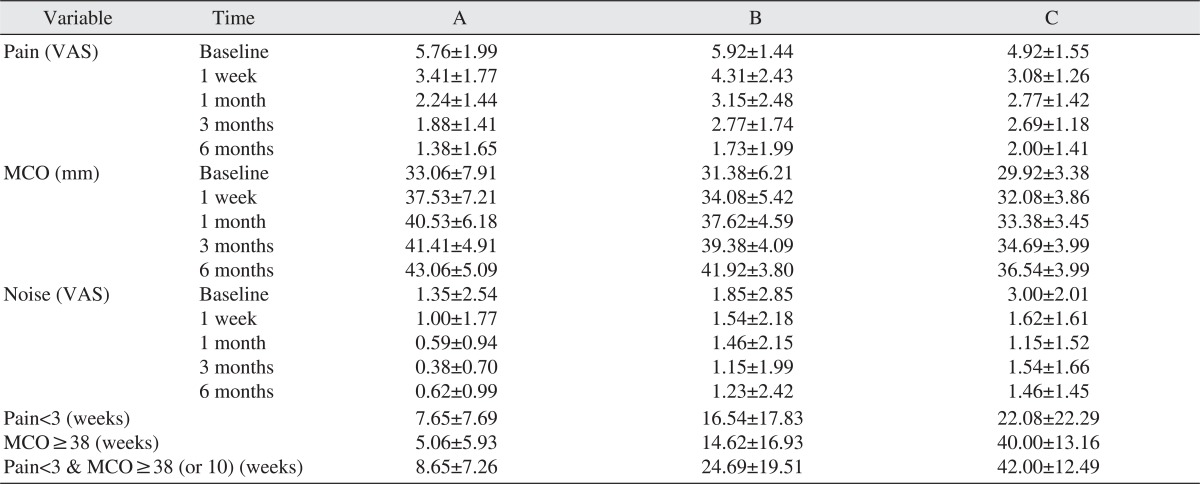
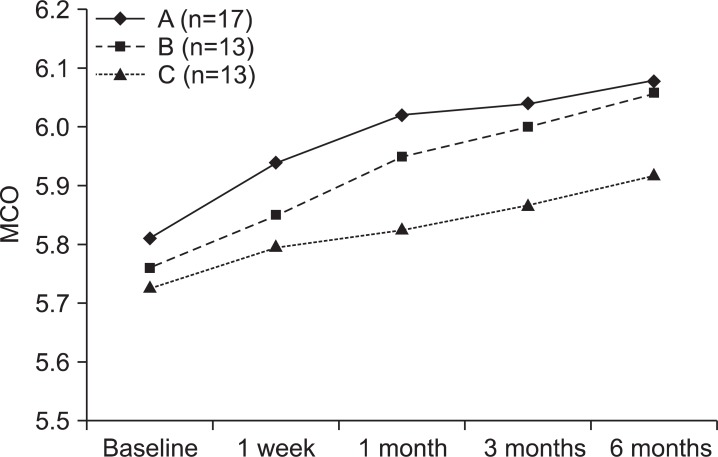
The baseline mean MCO of group A, group B, and group C was 33.06, 31.38, and 29.92, respectively. After treatment, there was an increase in mean MCO in all groups, with group A, group B, and group C recording 43.06, 41.92, and 36.54, respectively. At the follow-up check after 6 months, increases of MCO for group A, group B, and group C were 10.00, 10.54, and 6.62, respectively.
The baseline mean VAS scores for noise of group A, group B, and group C were 1.35, 1.85, and 3.00, respectively. After treatment, there was a reduction in the mean VAS for noise in all groups, with group A, group B, and group C recording 0.62, 1.23, and 1.46, respectively.
For group A, the period of pain<3 was 7.65 weeks, MCO ≥38 (or 10) was 5.06 weeks, and both pain<3 and MCO≥38 (or 10) were 8.65 weeks. For group B, the period of pain<3 was 16.54 weeks, MCO≥38 (or 10) was 14.62 weeks, and both were 24.69 weeks. Finally, group C recorded 22.08 weeks for the period of pain<3, 40.00 weeks for MCO≥38 (or 10), and 42.00 weeks for both.
3. Comparison of VAS values and MCO between groups
The change patterns for pain, MCO, and noise in each group are shown in Table 4 and Figs. 1-3. We checked the variables at five points: baseline and 1 week, 1 month, 3 months, and 6 months later. For pain, there was no interaction between group and time (F=1.48, P=0.199). Time had a significant main effect (F=58.31, P<0.001), but the same cannot be said for group (F=0.702, P=0.502). Based on Bonferroni's post hoc test, the levels of pain were found to decrease continuously; the difference was significant in group A (F=27.12, P<0.001) and group B (F=20.11, P<0.001). In contrast, pain in group C showed a decreasing tendency but increased 3 months later (F=15.34, P<0.001).
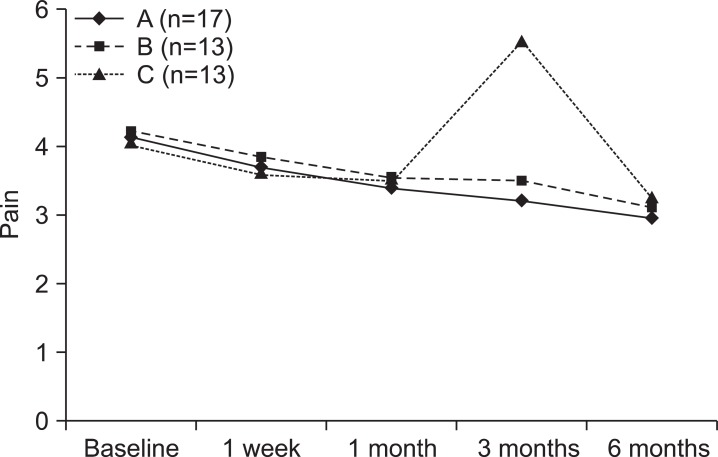 | Fig. 1Comparison of visual analog scale (VAS) pain values between groups. F=repeated measure of ANOVA.
|
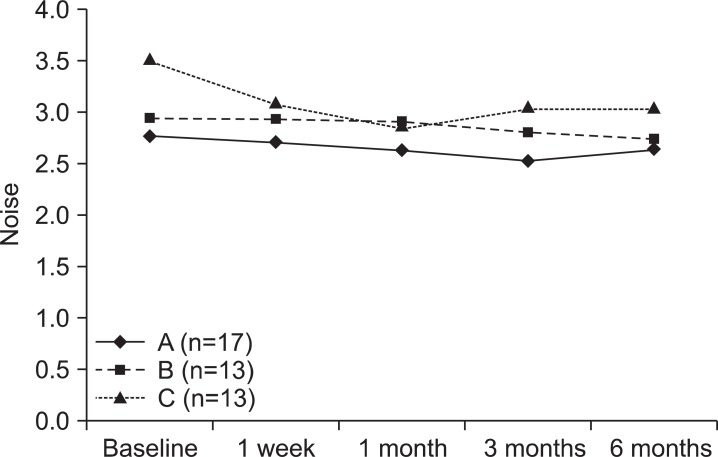
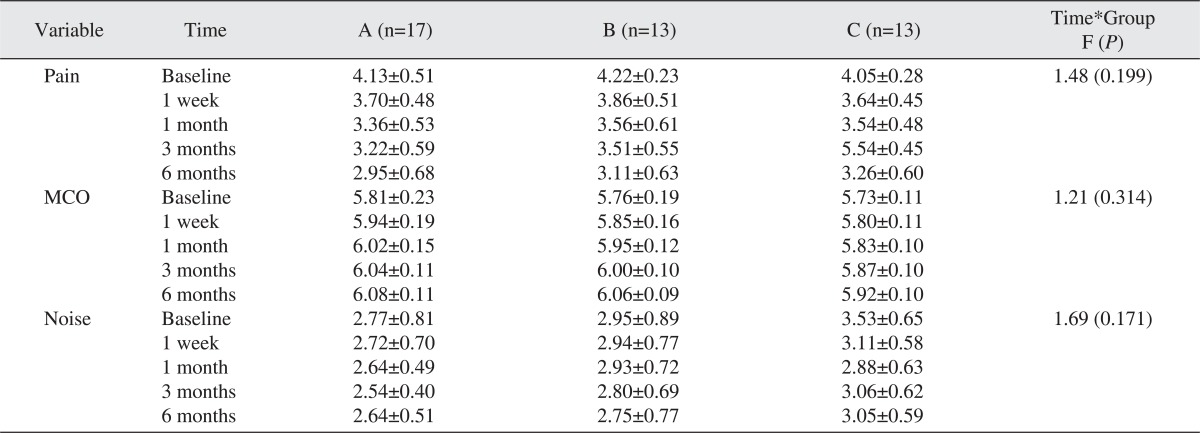
For MCO, there was no interaction between group and time (F=1.21, P=0.314). Group had a significant main effect (F=6.25, P=0.004); the main effect of time was not significant, however (F=49.67, P<0.001). For noise, there was no interaction between group and time (F=1.69, P=0.171). Time had a significant main effect (F=4.87, P=0.014), whereas the main effect of group was not significant (F=2.34, P=0.109). Bonferroni's post hoc test showed that noise in group C changed significantly compared to group A or group B. Noise in group C decreased from baseline (3.53±0.65) to 1 month later (2.88±0.63) and increased 3 months (3.06±0.62) and 6 months (3.05±0.59) later.
4. Comparison of the period to achieve normal state between groups
ANOVA were conducted to determine if there was any relationship between group and study variables, i.e., period of pain<3, MCO≥38 (or 10) and both pain<3 and MCO≥38 (or 10). Table 5 and Fig. 4 shows that the mean log value of pain<3 was 4.06 in group A, 4.55 in group B, and 4.79 in group C. There was no association between group and period of pain<3 (F=1.53, P=0.228). For MCO≥38 (or 10), the mean log level was 3.80 in group A, 4.55 in group B, and 5.96 in group C. There was significant difference according to treatment (F=28.71, P<0.001). Group B took longer time to achieve normal state than group A, with group C taking longer time than group B.
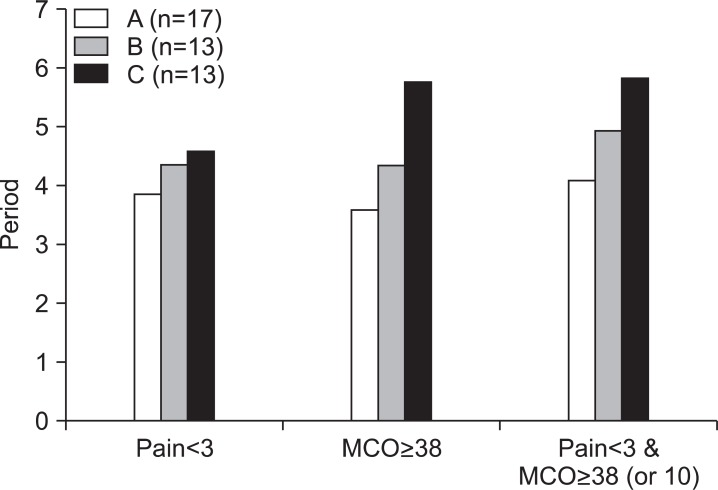

For both pain<3 and MCO≥38 (or 10), the mean log score of group A was 4.28, that of group B was 5.12, and that of group C was 6.02. The difference was statistically significant (F=16.62, P<0.001). Therefore, "simultaneous application of arthrocentesis and occlusal splint" was proven to be an effective method for TMD.
Go to :
IV. Discussion
This study compared the treatment outcomes of the simultaneous application of arthrocentesis and occlusal splint (group A), arthrocentesis after occlusal splint use (group B), and occlusal splint use only (group C).
As a result, all groups in this study showed improvement in pain, MCO, and noise. There was no interaction between group and time, however. On the other hand, an association was observed between group and period of normal state. For MCO≥38 (or 10), there was a significant difference by treatment. Group B took longer time to achieve normal state than group A, with group C taking longer time than group B. For both pain<3 and MCO≥38 (or 10), a statistically significant difference was noted. Group A took less time to achieve normal state than group B and group C. A more effective result was observed in group A than in the two other groups at the initial stage.
Occlusal splint is one of the most widely used treatments for TMD. Carraro and Caffesse16 claimed that the adoption of occlusal splint reduced TMJ pain by approximately 70% and muscle pain related to increased muscle activity by around 85.2%. According to de Leeuw et al.17, a nonsurgical approach achieved long-term effects for patients with internal derange ment in a 30-year follow-up study. The initiation of splint use within a short period after symptom onset was found to increase treatment efficiency18. Thus, occlusal splint inser tion and physical treatment are the most commonly used conservative alternatives19 through which approximately 90% of all TMD cases can be successfully treated20.
Nonetheless, Major and Nebbe21 reported that the use of occlusal splint resulted in the effective reduction of headache and muscle pain, but that it had a limitation in the reduction of TMJ pain. According to Lundh et al.22, occlusal splint had no advantage in treating disc dislocation without reduction.
Therefore, in the treatment of TMD, conservative therapies such as occlusal splint do not achieve a satisfactory outcome in some cases. A surgical method should be considered in such cases. Surgical methods include arthocentesis, arthroscope, discectomy, and insertion of implant.
In 1986, Sanders23 reported that arthrocentesis using saline solution or Ringer's solution was effective in the treat ment of synovitis in a case study. Arthrocentesis is developed and established by many researchers - including Murakami et al.24 in 1987 and Nitzan et al.25 in 1990 - as a treatment option that shows satisfactory prognosis.
Arthrocentesis is a minimally invasive procedure that may be performed under local anesthesia with or without sedation; its main purpose is to clear the joint of tissue debris, blood, and pain mediators, believed to be byproducts of intra-articular inflammation26.
Kropmans et al.27 investigated the results of 62 previous studies and reported that the combined treatment of arthrocentesis and occlusal splint was effective.
According to Park et al.28, the combination of arthrocentesis and stabilization splint for TMD patients enabled an increase in the amount of maximum mouth opening and decrease in the average value of pain.
In light of the results of this study, arthrocentesis and occlusal splint are good for TMD patients. Note, however, that the simultaneous application of arthrocentesis and occlusal splint is more effective, reducing the patient's discomfort in a shorter time and improving the patient's quality of life.
Go to :
V. Conclusion
The improvement of symptoms was noted in group A, group B, and group C, but group A exhibited quicker improvement than the other groups in terms of pain reduction and MCO increases. In other words, a more effective result was observed in group A than in the two other groups at the initial stage.
Go to :
 XML Download
XML Download