

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
According to Luhr's classification1, atrophic edentulous mandibular fracture is fracture of an edentulous patient's remaining mandible with the width of less than 20 mm. The mandible is divided into the alveolar bone and basal bone. Because alveolar bone is maintained by the functional loading of teeth, atrophic mandible is common among old edentulous patients2. Yang et al.3 reported a 12.7% ratio of edentulous mandible among domestic patients aged 65 and over. Mugino et al.4 reported that only 11 out of 335 mandibular fracture patients (3%) treated during the period of 1980-2004 had edentulous mandibular fracture, and that only 8 (2.3%) had atrophic mandible. As such, the incidence of atrophic edentulous mandibular fracture is very rare, and it is difficult for surgeons to gain enough clinical experience.
Following the principle of general fracture treatment, maintaining the function and shape of the mandible by reducing and fixing the fracture segment, is also applied to edentulous mandibular fracture. However, open reduction has been criticized since it is hard to put old patients under general anesthesia, and blood flow may be diminished due to subperiosteal dissection caused by surgery5. Therefore, closed reduction using maxillomandibular fixation has been preferred traditionally. Nonetheless, because edentulous patients have no tooth, and given the small cross-sectional area of mandible, it is hard to perform maxillomandibular fixation by closed reduction, and long fixation periods may cause the deterioration of respiratory function and temporomandibular joint disorder6.
It is known that blood flow is critical factor in the healing of fracture, but stable reduction and fixation of bony segments are also important5. Therefore, we report our recent cases where in two atrophic edentulous mandibular fracture patients were treated successfully by open reduction and rigid fixation using a locking plate system based on the Association for Osteosynthesis principle7 together with a review of articles.
II. Cases Report
1. Case 1
On September 22, 2010, an 85-year-old female patient had a car accident at a crosswalk at dawn; she was rushed to our emergency room due to bilateral mandibular body fracture. She was referred to the department of oral and maxillofacial surgery and hospitalized to have an operation. In the clinical examination, displacement of bony segment was visible, and it was moved manually. The patient complained of hypoesthesia in the overall lower lip and chin area. There were overall ecchymosis and edema in the vestibule of the mouth, but the bone was not exposed. In the panoramic view and threedimensional computed tomography, a fracture line was observed in the bilateral mandibular body area; there was no other fracture.(Figs. 1, 2)
Operation was performed by intraoral approach. After making an incision on alveolar crest, fullthickness subperiosteal dissection was done to expose the fractured area while preserving the mental nerve.(Fig. 3. A) The bony segment was reduced temporarily by a boneholding forcep, and bicortical fixation was then performed on both sides using 2.4 mm 6-hole universal reconstruction plate (Stryker, Vienna, Austria) with 1012 mm screws. In this process, the mental nerve was kept intact.(Fig. 3. B) Primary suture was carried out as continuous suture using nonabsorbable sutures, and silastic drain was inserted. There was no special complication during the operation. A day after the operation, a wellreduced bony segment was observed in the panoramic view.(Fig. 4. A) Two days after the operation, the drain was removed; the patient was discharged four days after the operation. On the 9th day, the patient visited the department of oral and maxillofacial surgery to have the sutures removed, and threemonth panoramic view and monitoring were done. (Fig. 4. B) Although the patient did not recover completely from hypoesthesia in the lower lip and chin on both sides, some improvement was noted, and the surgical site was healed without complication. She did not have a denture since the first medical examination and did not want to have one after the operation. So it was impossible to gain a normal occlusion of the patient.
2. Case 2
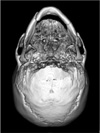
On February 3, 2011, a 61-year-old male patient slipped at dawn while going to the bathroom. He was rushed to our emergency room due to fracture of the mandible and referred to the department of oral and maxillofacial surgery. The patient was discharged from the emergency room due to personal affairs, but 2 days after injury, he visited again due to the pain in the mandible. In the clinical examination, there was no exposed bone, but displacement of bony segment in the right mandibular angle and hypoesthesia of the right lip were noted. In the computed tomography (CT), a fracture line was observed in the right mandibular angle and left body.(Fig. 5) There was no special medical history. The patient was hospitalized on February 7, 2011, and operation was performed 5 days after injury. Bilateral extraoral approach was used while monitoring the preservation of the marginal mandibular nerve with a nerve stimulator. During the operation, the facial artery and vein were ligated. After exposing the fractured area, the bony segment was reduced temporarily using boneholding forcep, and bicortical fixation was performed on both sides using 2.4 mm 6-hole universal reconstruction plate and 10-12 mm screws. A drain (Hemovac; Sewoon Medical, Seoul, Korea) was inserted, and primary suture was performed using absorbable sutures and stapler in each layer. There was no special complication during the operation. A day after the operation, a well-reduced bony segment was observed in the panoramic view. (Fig. 6. A) Four days after the operation, the drain was removed; on the 6th day, the sutures were removed. The patient was discharged the next day. His panoramic view (Fig. 6. B) had been taken, and he was monitored for 6 weeks after the operation. Although the hypoesthesia in the right area was not recovered, the fractured area was healed without special complication. Temporary relining was performed on the bottom of the denture used after removing sutures. Prosthesis and hospital visit were recommended for the complete recovery of normal occlusion, but the patient refused due to cost; further monitoring was not done because he wanted to be treated in another hospital.
III. Discussion
According to Luhr et al.1, atrophic edentulous mandible is when the width of the mandible is less than 20 mm. It is divided into class I (16-20 mm), class II (11-15 mm), and class III (less than 10 mm) based on the width of the remaining mandible. In these two cases, the thinnest part of the mandible in CT was 10.6 mm and 19 mm, respectively, and classified as class II and class I atrophic edentulous mandibular fracture, respectively, according to Luhr's classification. Ellis and Price5 stated that, to treat patients with edentulous atrophic mandibular fracture, the application of open surgery, approaching method in surgery, method of periosteal dissection, type of metal plate used in internal plate fixation, and application of bone graft should be considered. Therefore, the treatment of these two cases was planned before the operation considering the aforesaid matters.
The application of open reduction to old patients with atrophic edentulous mandibular fracture is still controversial due to the possibility of complication and deterioration of blood flow in the fractured area caused by operation5,8. Though old patients are likely to have complication due to operation or general anesthesia, such risk can be reduced by cooperating with the related department and reinforcing postoperative management9. In Case 1, although the patient was old and had systemic diseases, she was discharged without special complication and with good prognosis. According to the research of Bradley10, blood flow in the atrophic mandible was supplied by the surrounding soft tissues. It is known that blood flow is critical factor in the healing of fracture, but stable reduction and fixation of bony segment are also important11,12. It is proved by research that the application of open reduction yields good clinical results1,5.
Approaching methods of open surgery are divided into intraoral and extraoral approaches. Since there is no evidence for the superiority of one approach over the other, the surgeon can select between them5. In Case 1, as shown in Fig. 3. A, intraoral approach was used because the fractured area is in the front of the mandible. Thus, there was no problem in moving instruments and securing a clear view with enough exposure being provided. In Case 2, the extraoral approach was used because the right angle (Fig. 5) was in the rear; hence the difficulty to move the instrument to fix the screw vertically when using the intraoral approach. After experiencing two cases, we concluded that intraoral approach was favorable for fracture in the front of the very atrophic mandible, and that extraoral approach was favorable for fracture in the less atrophic mandible or in the angle area. According to Luhr et al.1 and Bradley10, when operating edentulous mandibular fracture patients, the application of supra-periosteal exposure as periosteal dissection may sustain blood flow. When carrying out supraperiosteal exposure, however, it is hard to reduce bone accurately and fix metal plates because the fractured area is not visible. In addition, a recent animal testing reported that supraperiosteal exposure did not increase blood flow13. Our two cases used subperiosteal exposure, but there was no problem in the healing of fracture.
In monocortical fixation using miniplate, buttressing between fracture segment is very important, with the wider section providing stronger support14,15. Therefore, if this method is applied to atrophic edentulous mandibular fracture with small crosssectional area, the miniplate is likely to have fatigue fracture due to the movement of the bony segment. When two miniplates are used, the longer distance between plates provides stronger support16. In atrophic edentulous mandible, however, it is difficult to secure enough distance between plates. For a small crosssectional area of fracture, the concept of load bearing should be applied, and such may be obtained by bicortical fixation using locking plate7. According to Sikes et al.17, in the atrophic mandible, the fixation of bony segment using reconstruction plate is better than monocortical fixation using miniplate. Kunz et al.18 reported that the reconstruction plate applied to 40 atrophic edentulous mandibular fracture patients recorded a success rate of 95%. Therefore, we performed bicortical fixation using a 2.4 mm universal locking plate. In the locking plate system, the plate can provide stable fixation without being attached on the surface of the bone; thus facilitating the adjustment of the plate19. In addition, the locking plate can be applied regardless of the area with tensile force, and denture can be used without additional plate removal surgery if applied to the base of the mandible. The patients in these two cases did not want to remove the metal plate. Therefore, we decided that bone graft was not necessary owing to the low possibility of pathologic fracture, and because it is better to adjust the existing denture.
Oral and maxillofacial surgeons rarely have patients with atrophic edentulous mandibular fracture, and they tend to avoid operation because of the patients' old age. After experiencing the two cases above and reviewing articles, however, we recommend performing bicortical fixation using a reconstruction plate after subperiosteal exposure if surgery is possible.





 XML Download
XML Download