

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Clefts of lip and palate are the most common deformities in oral and maxillofacial area. Although different research institutes in Korea reported various incidence rates regarding clefts of lip and palate, they are generally known to show an incidence of 0.95-2.25 per 1,000 newborn babies1. Bilateral cleft lip, in particular, may be symmetrical or asymmetrical due to its complex aspects. It appears in various forms from the case of cleft lip only to the case of cleft lip accompanied with alveolar cleft or cleft plate. Moreover, the sizes, shapes of its growth segments and the ratios between the segments change along with the growth of the patient. Therefore, successful surgical repair of bilateral cleft lip requires understanding of these various aspects and such changes occurring along with the growth of the patient2.
Treatment of bilateral cleft lip has been classically considered to be much more difficult than treatment of unilateral cleft lip3, and the surgical technique has gradually developed from the staged closure applying unilateral cleft lip surgery to simultaneous closure2,4. In the past, attention was focused on the lip itself, and correction of nasal deformity was postponed because early manipulation of nasal cartilage was thought to prevent its growth. Such thought, however, has been found to be groundless by research5, and synchronous repair of bilateral cleft lip and nose deformity was introduced, in which treatment of bilateral cleft lip was accompanied with correction of nasal deformity.
Mulliken is a pioneer of synchronous bilateral cleft lip and nasal deformity repair. He established the following five surgical principles in 1985: 1) maintenance of symmetry; 2) establishment of basic muscle continuity; 3) proper size and shape of the philtrum; 4) formation of the median tubercle from the lateral lip elements; and 5) primary position of the alar cartilage for construction of the nasal tip and columella. Mulliken said it is important to understand and apply these surgical principles rather than the surgical technique itself, and through research on growth measurements of bilateral cleft lip patients, he also emphasized the importance of taking growth into consideration2,6. Authors are to report a case of applying the Mulliken's principles and techniques for treatment of bilateral cleft lip patients.
II. Case Report
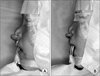
We visited Hanoi National Hospital of Odonto-Stomatology in 2009 and 2011, and the same operator performed surgery on two bilateral cleft lip and nose patients on the basis of Mulliken's principles and techniques. The first patient was an 18-month-old male, who was observed to have protrusive premaxilla because early surgical repair had not been performed.(Fig. 1. A) The second patient was an 8-month-old male, who did not have severe protruding premaxilla.(Fig. 1. B) In the case of the first patient, it was difficult to restore alveolar ridge continuity due to protrusive premaxilla, excessive soft tissue tension would have been expected due to immoderate dissection and closure if surgery had been performed without dealing with the problem first. Therefore, after premaxilla osteotomy, premaxilla was repositioned backward to a favorable position for surgery.(Figs. 2, 3) Afterwards, surgery was performed in the order of marking, dissection, closure and nasal correction. Since the surgeries were performed as part of our volunteer service activities overseas, it was unable to carry out a long-term observation of the patients' clinical course postoperatively.
1. Flap marking
The philtral flap was designed to be a little biconcave and its end to be dart-shaped because of the tendency of cicatrix to bulge outward later on the edges of its both sides. A long narrow strip was designed on both sides of the philtral flap for deepithelization, which was then performed in order to form a philtral ridge by placing it below the lateral labial flap. The peaks of the Cupid's bow to be formed were placed on the lateral labial elements. An alar base flap was designed on the upper junction of the lateral labial elements. The medial edges of the lateral labial elements were designed along right above the vermilion-cutaneous line.(Fig. 4) The second patient had a left nostril sill, but since the sill was unnecessary for advancement of the alar base flap, an incision line was also established on it.(Fig. 4. B)
2. Dissection
The philtral flap was incised up to the dermis, then the pieces of skin on its side were deepithelized, and then the remaining prolabial lip skin was excised. The philtral flap, including the subdermal soft tissue, was elevated from the premaxilla to the caudal septum. An alar base flap was formed by incising the lateral white line-vermilion-mucosal flap, and a bundle of orbicularis oris muscles was dissected from the lateral labial elements.(Fig. 5)
3. Closure
The alveolar ridge on both sides of the cleft was incised vertically and then closed by raising the gingivomucoperiosteal flap. The anterior wall of the gingivolabial sulcus was shortened by excising and refining the vermilion-mucosa remaining in premaxilla. The remaining mucous membrane of the premaxilla was made to be a flap, which was then sutured to the periosteum of the anterior nasal spine, thus achieving formation of the posterior wall of the anterior gingivolabial sulcus. By advancing the lateral labial element fully inward, medial mucosal flaps were made to form the anterior wall of the central gingivolabial sulcus and the posterior aspect of the upper lip. The orbicularis oris muscles were sutured from the bottom to the top. The pars peripheralis, the top closure, was sutured to the periosteum of the anterior nasal spine.(Fig. 5) The median tubercle was formed using the remaining portion of the lateral lip. The last skin closure was performed after nasal correction.
4. Nasal correction
The bilateral alar cartilage was exposed by incising the bilateral nostril rim. Interdormal mattress suture was perfor-med on the genuas of the bilateral alar cartilage as well as on its middle cruses, and then the sutured genuas and the sutured middle cruses were sutured to the upper lateral cartilage at the lateral side of genua and at the lateral crus respectively. The alar width was narrowed to 25 mm or below by positioning the cinch suture on each alar base.(Fig. 6) A nostril sill was constructed by cutting and refining the end of an alar base flap and then rotating it inward, thus suturing it to the end of the skin on both sides of the columellar base. The dermis of each alar base flap was sutured to the periosteum of the premaxilla and the orbicularis oris muscle, thus forming a normal cymal shape of the lateral sill and lowering the position of the alar base. This could minimize the nostrils being lifted during the patient's smile by stimulating the depressor alae nasi muscle.(Fig. 7)
If alar cartilage is properly positioned, there will clearly be extra skin in the soft triangle. The extra skin was excised together with the remaining skin on the lateral side of the columella. Crescentic excision was extended to the top and middle of the columella, passing the incision line on the nostril edge. Moreover, a lateral vestibular web appears inside the nose. This web was incised by lens type incision along the intercartilaginous line, after which it was sutured.(Fig. 7)
After completion of nasal correction, the last skin closure was performed. The end of the philtral flap was placed inside and sutured to the muscular layer in order to form a philtral ridge by having the philtral flap settle down.(Fig. 8) The height of the lateral lip was modified by cutting and refining the top edge of the lateral labial flap in the form of a cymal curve at the alar-labial junction.(Fig. 8. A)
III. Discussion
The suitable time for performing primary cheiloplasty on bilateral complete cleft lip patients may be variable according to literatures, but it is generally performed between 3 to 6 months after birth7. In cases of protrusive premaxilla, it is necessary to treat it surgically or nonsurgically before primary cheiloplasty. So the timing of primary cheiloplasty may be adjusted according to the prior surgical or nonsurgical treatment of the protrusive premaxilla. Protrusion of the premaxilla is a phenomenon appearing due to the abnormal growth of the bone under the influence of the strength of sticking out the tongue located in the bilateral cleft lip together with the abnormal muscular strength of the orbicularis oris muscles which are not continuous due to the cleft lip8. In the first case, surgical repositioning of the premaxilla was performed on the first 18-month-old patient (Fig. 1. A) because it was impossible to achieve a primary repair without treating the premaxilla first. Surgical repositioning of the premaxilla is recommended for 6 to 8-year-old patients rather than younger patients because surgical repositioning may hamper the growth of the midface9. In the first case, however, premaxillary osteotomy was performed on the patient during the course of primary correction of cleft lip and nasal deformity despite his age of 18 months because neither periodical observation of his clinical course nor use of an orthopedic appliance was possible due to economic circumstances.(Fig. 2) As premaxillary osteotomy was performed in the posterior part of the epiphyseal line and the surgical repositioning of the premaxilla took place without any particular fixation, we think the growth of the baby patient's midface would be inhibited only slightly.
It is necessary to understand the nasal and labial shape of a normal baby for correction of bilateral cleft lip, but only three-dimensional understanding is not sufficient. The surgeon must be aware of the changes that would appear during the normal growth and even be able to predict distortions occurring in the patient who had underwent surgery. Accordingly, it is necessary to perform fourth-dimensional treatment by taking changes in growth into consideration. Mulliken et al.10 confirmed that there is a correlation between the three-dimensional size immediately after the surgery and the growth speed by growth observation of bilateral cleft lip patients who had underwent surgery. In other words, the fast-growing parts would grow to be longer or wider whereas the slow-growing parts would deform to be shorter. The surgery must make the fast-growing parts smaller and the slow-growing parts slightly bigger than normal. Farkas et al.11 mentioned in their growth research in normal white people that nasal tip protrusion and columellar length grow slowly while reporting that all the labial parts grow fast, thus reaching 90% of an adult's labial parts size by the age of 5 years. Also in the two cases, surgery was performed based on these grounds, thus narrowing the nasal width to be 25 mm or below and increasing the columellar length. Since lips grow fast except the median tubercle, the patient's lips were formed to be shorter and narrower on an overall basis.(Fig. 8)
It is known that there are various methods of primary cheiloplasty for bilateral cleft lip, but none of them is perfect. Traditional methods, in particular, involve pulling the medial crura of the nose backward and downward, thus causing the columella to be shorter12. Because of these limitations of surgical methods, most surgeons perform primary correction while keeping in mind secondary surgery for columellar lengthening. Millard13 and Cronin14 stored some forked flaps in the inferior part of the nasal sill during the primary surgery and then used them in the secondary surgery. In 1990, however, McComb15 reported unaesthetic results such as nasal tip lengthening, unnatural nostrils, and excessive lengthening of the columella in their retrospective study of the two-stage surgery for 15 years. Mulliken also used the two-stage surgery for nasal correction initially. After understanding, however, that the nose of a bilateral cleft lip and nose patient just looks short but is not really short, he started to perform nasal correction without any additional tissue transplant. In addition, he established the present surgical procedures after stopping nasal tip vertical incision in order to minimize cicatrixes. He reported that as a result of retrospective comparison of his surgical procedures, the two-stage surgery and the one-stage surgery generally showed similar results. Also in the two cases, nasal correction was performed after an approach through the nostril marginal incision without using the nasal tip vertical incision approach.(Fig. 7)
In primary correction of cleft lip and nasal deformity using the Mulliken method, the three-dimensional position was determined based on the growth of white people. Mulliken proposed that the length of the philtral flap be 6-8 mm, that the distance between the peak of Cupid's bow be 3-4 mm, and that it should be 2 mm at the columellar-labial junction. Kim et al.16, however, announced the bilateral cleft lip surgery performed on some Koreans using the Mulliken method, also mentioning the necessity of some modification in the three-dimensional position due to the tendency of Koreans having fewer tissues than white people. They proposed that the length of the philtral flap be as long as possible, that the distance between the peak of Cupid's bow be 5 mm, and that it should be 3 mm at the columellar-labial junction. Since the patients were also oriental people in this case, we applied the modified three-dimensional position to the surgical operation.
The principles of the primary correction of bilateral cleft lip and nasal deformity had been established, and the surgical technique is gradually developing. The Mulliken method is a four-dimensional treatment taking growth into consideration, and good results are being reported both in Korea and abroad through this surgical method6,16. We hope this case report be helpful for oral and maxillofacial surgeons in applying the Mulliken's treatment method in their surgical operations.







 XML Download
XML Download