

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
The hypermobility disorder of the temporomandibular joint (TMJ) may be classified into hypertranslation, subluxation, and dislocation1. Among them, hypertranslation is an excessive forward movement of the condylar head at the mouth opening, but it has no clinical meaning. If the patient cannot control the dislocated maxillary bone without an outer force, it is called true luxation. The temporary or incomplete dislocation that the patient can overcome himself/herself within a few hours is called subluxation2.
Most patients suffering from dislocation visit the emergency room or the hospital as an outpatient due to habitual dislocation, which may be cured through manual reduction therapy without anesthesia but may be more difficult to treat due to the fibrous adhesions between the joint disc and condylus in case of higher frequency of dislocation.
The treatment of TMJ dislocation is largely divided into nonsurgical and surgical methods. Nonsurgical methods include arthroplasty of TMJ, physical therapy, occlusal adjustment, therapy using occlusion stabilization devices, drug therapy, intermaxillary fixation or sclerotherapy, etc. In case these nonsurgical therapies fail, or they become recurrent or chronic, the surgical method must be considered3. Frequently used surgical methods include condylectomy4-6, fixation, lateral pterygoid muscle myotomy technique7 and zygomatic arch downfracture technique8, augmentation procedure using various kinds of planting fixtures9-11, etc.
In this case, wherein the chronic TMJ dislocation of a 74-year-old patient was treated with condylectomy and a good clinical result was obtained with no condylar movement disorder in the TMJ six months after the bilateral condylectomy.
II. Case Report
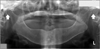
A 74-year-old female patient visited our department. Having medical history of radiation treatment due to thyroid cancer, the patient was treated with manual reduction for dislocated jaw in a clinic for the first time two years ago. She had evaded reduction for fear of the pain that she experienced during the previous manual reduction, even though the dislocation recurred 6 months before her visit to our department. Her lower jaw was protruding forward at the time of her visit, and she could not masticate anything due to the continuous pain on the left jaw joint and dislocation of mandibular joint, drooling at the mouth opening. The panoramic and computed tomography images showed symptoms of osteoarthritis with bone deformation, confirming the dislocation of jaw.(Fig. 1) Traditional manual reduction was performed but failed due to pain; thus, reduction was performed under monitored anesthesia care, with the affected area fixed with elastic bandages. Note, however, that the dislocation did not improve. Thus, surgery was decided after discussion with the patient and her guardian.
All the physical findings including the blood test and urinalysis conducted before the surgery showed normal results, and bilateral condylectomy was planned. Anatomical landmarks for zygomatic arch and condyle head were drawed on the surface of the patient's skin. Infiltration anesthesia was administered with 2% lidocaine (1 : 100,000 epinephrine) on the area of incision; to expose the zygomatic arch and condylar head, the skin was cut open through the preauricular incision approach. The articular capsule was incised horizontally, and the upper part of the mandibular fossa and condyle were exposed. The upper part of the condyle head was incised using cutting instruments under irrigation of water, with the incised mandibular condyle head trimmed to remove the sharp parts, washed with saline solution containing antibiotics, and subsequently sutured in a layered manner. The drainage tube was not used.(Figs. 2, 3)
After surgery, the patient was instructed to perform gradual mandibular opening movement by taking liquid food during the hospitalization period, but other intermaxillary fixation or occlusal adjustment or occlusion stability devices were not utilized. After being discharged from the hospital on the 7th day of surgery, the patient was instructed to take oral antibiotics, and analgesics for 7 days. One month after the surgery, the opening distance between edentulous ridges in the anterior teeth reached as far as 40 mm, and the panoramic image showed incised mandibular condyle on both sides. Two months after the surgery, dentures were made while the patient underwent physical therapy.(Fig. 4)
III. Discussion
The hypertranslation of TMJ in hypermobility disorders is known as an excessive forward movement of the condylar head at the mouth opening; the extent of exact forward movement is not defined, but the condylar head is located on the forward part of the condylus at the widest opening of the mouth. Dislocation of the TMJ may occur in several directions such as forward, rear, upper, and outward directions, although forward dislocation occurs most frequently. It is a condition wherein the condylar head is moved to the forward part of the condylus and its open lock since the patient cannot control it himself/herself. It occurs because the contraction of the masseter muscle and temporalis causes the lower jaw to get out of the glenoid cavity, and the spasm of the following masseter muscle, temporal muscle, and pterygoid muscle hampers the mandibular condyle from going back to its original position. It is divided into acute dislocation and recurrent dislocation depending on frequency of occurrence; in case it continues to exhibit the same symptoms for over 3 weeks after its occurrence, and the open lock, it is called chronic dislocation.
The cause of acute dislocation is known to be excessive movement when opening the mouth due to injury, dystonic reaction, yawning, etc. It may occur while airway intubation for general anesthesia, tooth extraction, or endoscopic operation for digestive tract is performed3.
Chronic recurrent forward dislocation is observed in a patient with habitual dislocation and whose mandibular condyle turns toward the rear down, unable to return to its original position in case the inclination of the joint condylus is anatomically sharp. In most cases, acute recurrent dislocation may be treated through manual reduction, botulinum toxin injections12, autologous blood injection13, etc.
The recurrent forward dislocation of the TMJ has various causes, including local ones such as change of laxity due to injury of articulate capsule and ligament or internal derangement of the TMJ, prolonged degenerative arthropamandib, functional disorder of the TMJ, morphological alterations of the temporomandibular condylus, or occurrence caused by drugs such as phenothiamine14. Systemic causes include systemic diseases such as Ehlers-Danlos syndrome15, liver cirrhosis, Parkinson's disease, or neurological diseases such as hysteria.
The clinical symptoms of the TMJ include the change of occlusion and face, reduction of mastication function, etc. Once the dislocation of the TMJ occurs bilaterally or laterally, the mouth cannot be closed without pain, tension of mastication muscle increases dramatically, and pronunciation is impossible. The patient also drools. The lateral dislocation of the joint may be controlled relatively simply through manual reduction; if it develops into a chronic one, however, treatment is difficult because the spasm of the masticatory muscle worsens and increase in thickness of the joint disc rear tissue and fibrous adhesion occur as a result of inflammatory response. The dislocation of the TMJ may be treated with intermaxillary fixation, manual reduction, physical therapy, insertion of hardener in the upper articular capsule, occlusion adjustment, pharmacotherapy using nonsteroidal inflammatory drugs or muscle relaxants, or nonsurgical therapy that induces the myostatic contraction of maxillary bone levator muscles using oral appliances that limit condylar movement. Note, however, that surgery may be considered in case the dislocation occurs recurrently and habitually or when the nonsurgical treatment fails.
For the surgical treatment of TMJ dislocation, various methods through which the clinician facilitates the condylar mobility of the TMJ or artificially places an obstacle to limit condylar mobility have been introduced. The eminectomy of surgical treatments was described by Myrhaug4 for the first time in 1951 and was later asserted by Irby3. It is one of the most universal treatments wherein the lower inclined path is made by cutting out the condylus positioned in the condylar mobility path; its prognosis are quite good, but radiological reexamination prior to surgery and careful attention during surgery are required since perforation on the cerebral ventricles may occur in case of pneumatization in the eminectomy process.
For the treatment that limits the mobility of the mandibular condyle, several methods have been introduced. Georgiade5 and Merrill6 announced a treatment method to prevent the dislocation of the TMJ by connecting the condyle and the articular capsule to the zygomatic arch with a dacron strip after Murphy publicized the method of folding the ligament of the TMJ for the first time in 1912. In 1929, Konjetzny16 reported the fixation method using meniscoplasty, and Pogrel17 attempted to prevent the dislocation of the TMJ using the temporal fascial flap.
The lateral pterygoid muscle myotomy by surgical methods for the dislocation of the TMJ was publicized by Boman for the first time in 1949. It was a method of removing the obstacle and limiting forward condylar gliding mobility by carrying out muscle myotomy and removal of joint disc simultaneously. According to him, the recurrent symptoms of dislocation disappeared from all patients in a long-term follow-up survey after applying the method to 21 patients.
Practiced and announced by LeClere and Girard18 in 1943, the zygomatic arch downfracture technique was a method of increasing the vertical dimension of zygomatic arch by displacing it to the downward side of the condylus after downfracturing the zygomatic arch. Thereafter, Dautery, Lawler, etc., utilized the method significantly, but it had some problems such as facial changes or summative fixation.
In the treatment of TMJ dislocation, the method by increasing the vertical dimension around the condylus using the insertions, the rib bone, costochondral graft19 or vitallium mesh, bone plate, hydroxyapatite, etc., are mainly used. The method is so simple that complicated surgery can be avoided. It has a merit of minimizing the limit of functional movement for the mandibular condyle or occurrences of complications but it also has the demerit of transformation or fractures of materials due to the mechanical properties of the inserted materials15.
In this case, the dislocation was treated so that the TMJ can perform its normal functions by partially cutting out both sides of the mandibular condyle of the patient with dislocation of the TMJ and whose mandibular condyle went over the condylus, unable to return to its original position, although the dislocation was not recurrent. One month after the surgery, a good result of 40 mm mouth opening distance between ridges in the anterior teeth could be obtained.
For the treatment of TMJ dislocation, surgery may be an effective method in case the nonsurgical treatment fails or dislocation occurs recurrently and habitually. Various surgical treatments such as eminectomy, anchoring procedure, lateral pterygoid muscle myotomy, zygomatic arch downfracture technique, and technique to increase the condylus using artificial insertions were introduced as methods to prevent recurrent and habitual dislocation of the TMJ.
An effective treatment for a patient with dislocation of the TMJ is to secure sufficient volume of mouth opening and to make it function normally. To achieve such target, it is important to prevent re-dislocation after surgery and to maintain the mouth opening volumes through constant physical therapy.
The authors are reporting this sample case of bilateral condylectomy performed on a 74-year-old female patient diagnosed with dislocation of the TMJ, and a satisfactory result was obtained without recurrent findings or functional mobility disorder of the mandibular condyle particularly complications six months after the surgery.



 XML Download
XML Download