

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Originating with the separation of the follicle from around the crown of an unerupted tooth, the dentigerous cyst develops from fluid accumulation between the reduced enamel epithelium and the enamel surface1. Cystic develop ment is usually related to unerupted third molar or maxillary canine, and it has the tendency of displacing the related tooth. A cyst formed around the maxillary third molar may invade the maxillary sinus, growing unnoticed to such extensive size as to occupy a considerable portion of the maxillary sinus. As the cyst grows, the bony walls overlying the cyst thin out, giving rise to an egg shell sensation upon palpation and possibly transmitting pressure to the walls of the sinus; thus causing ophthalmologic and nasal symptoms to develop2. Some untreated dentigerous cysts may-in rare cases-grow large and have the potential to develop into an odontogenic tumor such as ameloblastoma or to become malignant as in oral squamous cell carcinoma and mucoepidermoid carcinoma.
The standard treatment for a dentigerous cyst involves surgical enucleation and extraction of the cyst-associated impacted or unerupted tooth3,4, but long time for follow-up is required to rule out postoperative recurrence and postoperative cystic development5.
The present case of an extensive dentigerous cyst involving the whole maxillary sinus in a 22-year-old female is not common; the lesion was enucleated by the Caldwell-Luc approach supported by computed tomography (CT) and magnetic resonance imaging (MRI) scan. The case was followed for a period of 7 years, and there was no evidence of sinus infection or recurring cyst formation. Thus, we present the case with literature reviews.
II. Case report
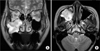
A 22-year-old female patient under orthodontic treatment at a local clinic was referred to our department for further evaluation. The patient suffered from swelling and dull pain around the right infraorbital area, with partial right-sided nasal obstruction and watering of the right eye. The intraoral examination revealed fluctuant mass palpating on the buccal vestibule from the first premolar to the second molar; though the mobility of the teeth could not be measured owing to fixed orthodontic appliances, teeth from the canine to the second molar showed negative response in the percussion test and turned out to be vital in electric pulp test. On Water's view, the right maxillary third molar was dislocated into the right maxillary sinus with the haziness of sinus. Thinned alveolar cortical bone around the lateral wall of the sinus was also observed.(Fig. 1. A) The CT scan showed an enlarged cystic lesion measuring 5.2 cm horizontally, 4.3 cm vertically, and 4 cm sagittally; a partially disrupted posterior sinus wall with some obliteration of the retro-maxillary flat plane caused by expansive mass was also noted.(Fig. 1. B) MRI revealed an expansile mass invading into the anterior masticatory space, but the dark rim of the posterior to the mass implicated the preservation of the posterior wall of the sinus. There was no evidence of orbital extension.(Fig. 2)
There were no abnormal findings in the patient's general examination, so enucleation of cyst of the right maxilla was performed using the Caldwell-Luc approach under general anesthesia. After periosteal reflection, the cystic sac was identified, and cystic mass containing yellowish fluid was detected from the thinned buccal cortical bone. The cyst was easily dissected together with the ectopic third molar from the sinus walls except the posterior wall-which was partially eroded-to the posterior wall of the sinus. The enucleated mass measured 5.3×4.2 cm and had an oval shape. The crown of the third molar was located within the lumen of the cyst, and its root remained outside.(Fig. 3. A) The excised mass was submitted for histopathological analysis, revealing a relatively uniform layer of non-keratinized, stratified, squamous epithelial lining cell.(Fig. 3. B) A diagnosis of the dentigerous cyst was made, and the postoperative status of the patient was uneventful. The patient remained symptom-free over a postoperative follow-up period of 7 years.
III. Discussion
As the most common type of developmental odontogenic cyst, dentigerous cyst is defined as an odontogenic cyst derived from reduced enamel epithelium surrounding the crown of an unerupted tooth1. It makes up about 20% of epithelium-lined cysts in the jaw, and it is commonly associated with unerupted mandibular or maxillary third molars or maxillary cuspids. It occurs at any age but has peak incidence in patients from the 10-30 year-old age group6,7. When the maxillary sinus is invaded, symptoms usually occur late in the process; the cyst usually remains asymptomatic but may produce painless bony expansion or facial asymmetry if it becomes large2,8. If inflamed, however, it becomes symptomatic, exhibiting classic signs of sinus disease including swelling, facial pain, headache, and nasolacrimal obstruction2,3,8,9. A large maxillary cyst involved the whole sinus in the present case. Since it can transmit pressure to the walls of the sinus, ophthalmologic and nasal symptoms may develop. Epiphora could occur owing to the pressure to the nasolacrimal canal from the cyst associated with an ectopic canine in the maxillary sinus2, and orbital proptosis could develop from a dentigerous cyst in the maxillary sinus associated with a displaced tooth7. As a differential dia gnosis, ameloblastoma is a benign epithelial odontogenic tumor consisting of cells similar to the enamel organ of dental follicle. It has similar clinical radiographic characteristics to the dentigerous cyst such as relatively rapid growth, painless facial swelling, and predilection at the mandibular molar area. Differential diagnosis between the two diseases is important in view of the clinical, radiological, prognostic, and therapeutic similarities. Note, however, that the age group in the incidence of ameloblastoma is younger compared to that of the cyst and odontogenic epithelium of dentigerous cyst, and dental follicle around an impacted tooth is usually replaced by squamous epithelium10; hence the low potential for transit to ameloblastoma. In addition, root resorption adjacent to the lesion is a critical factor in the radiographic differential diagnosis between the tumor and cysts in the jaw; that of ameloblastoma is higher than dentigerous cyst5,10.
Dentigerous cysts usually occur as well-circumscribed, unilocular radiolucencies surrounding the crown of a tooth and corticated border. In the present case, the entire borders of the lesion could not be clearly defined by plain radiograph such as Water's and panoramic views owing to image overlapping related to the hard palate and petrous bone of the skull10,11. The border of cysts may be rendered ambiguous by secondary infection or expansion to the posterior sinus wall; hence the need for 3-dimensional images. The CT scan showed cystic expansion to masticatory space, bony erosion of pterygoid wall, and thinned outer cortex. Since the unclear posterior border of cyst was detected, however, MR imaging was done to confirm the posterior border of the mass and to distinguish between malignant tumor and inflammation. In MR imaging, no changes in signal intensity at the masticatory space were detected; the dark rim of the hypointense signal located in the posterior mass reflected the preserved posterior wall of the maxillary sinus12,13.(Fig. 2. B)
Despite the disadvantages damaging to the vitality of engaged tooth and tissues, cyst enucleation is the most common procedure to prevent the development of benign or malignant tumors caused by cystic remnants. The Caldwell-Luc approach was reported to be the most common treatment when dentigerous cysts are associated with an impacted tooth within the maxillary sinus14,15. Marsupialization is another advisable treatment to preserve the cyst-associated tooth and promote its eruption16; note, however, that the major disadvantage of marsupialization is the recurrence or persistence of the lesion17. We performed total enucleation of the cyst and displaced tooth using the Caldwell-Luc operation followed by drainage to the nasoantral window rather than intraoral marsupialization because the posterolateral walls of the maxillary sinus were found to be eroded in part. No specific complications have been noted for 7 years after surgery (Fig. 4), but further follow-up is still needed to exclude the possibility of recurrence or postoperative maxillary cyst.



 XML Download
XML Download