

 PDF
PDF ePub
ePub Citation
Citation Print
Print


I. Introduction
Tooth ankylosis is defined as the condition wherein normal passive tooth eruption is ceased without physical impediment such as supernumerary tooth or impacted wisdom tooth1. The pathogenesis of ankylosis is not understood completely, and it is also called infraocclusion, secondary dental retention, and submerged tooth. Clinical findings for dental ankylosis include reduced occlusal surface area, inclination of adjacent teeth, underdevelopment of alveolar ridge of concrescence, absence of dental mobility, and abnormal percussion sound upon tapping (e.g., metallic percussion). Patients visit a clinic to address such clinical symptoms with no knowledge of ankylosis and normally seek orthodontic therapy2. Since the treatment of ankylosed tooth is not an easy job even for seasoned orthodontic dentists, surgical orthodontic treatment is primarily considered to avoid extracting the ankylosed tooth and to conserve it instead3. Another possibility is prosthetic restoration by implant after dental extraction. This approach, however, may require the broad cutting of alveolar bone in the event of removing the ankylosed dental root because cementum or dentin is anatomically fused with the alveolar bone. This can become an issue at the time of subsequent prosthetic restoration2. For the case wherein a maxillary molar is ankylosed, oro-antral fistula may occur, and such may pose the risk of displacement of root fragment into the maxillary sinus; thus possibly increasing the need for sinus implantation4-6. If the ankylosed tooth is fixed with root canal, there is bigger possibility of root fracture in the event of dental extraction, leading to increased complexity.
Another possibility is sinus bone grafting through lateral access- which is an invasive treatment- versus the crestal approach. Lately, however, the use of piezoelectric device7-13-which minimizes damage to soft tissue- is increasingly practiced. Since the method such as vascular tortuosity becomes assessable through pre-operative computed tomography (CT) scan14,15, such approach is preferentially considered for 3-4 mm or less sinus bone grafting6-18. The piezoelectric device- an ultrasonic surgical tool that uses the piezoelectric effect- causes no significant damage to soft tissue upon contact; thus enabling the elevation of sinus membrane without perforation during sinus bone grafting, further minimizing bleeding when cutting bone around the posterior superior alveolar artery.
This case report presents the case wherein an ankylosed tooth in the maxillary posterior region with root canal and gold crown was extracted and immediate sinus grafting was subsequently done for future implant placement.
II. Case Report
A 16-year-old female patient visited the Department of Advanced General Dentistry, College of Dentistry, Yonsei University to have her right maxillary first molar extracted. This patient made a prior visit to the Orthodontics Department of the hospital to address her different vertical teeth height. The Orthodontic Department sent us a referral for surgical dental extraction of the ankylosed tooth, after estimating that orthodontic treatment would be difficult because the molar was restored through gold crown after root canal.(Fig. 1)
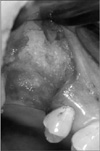
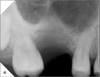
Root canal and prosthetic treatment were done at a private dental clinic 8 years ago, and approximately 3 mm of the crown was exposed upward from the gum. No dental mobility was observed, but sensitivity to percussion was noted. No gingival swelling or rubor was detected around the tooth, with a paradental cyst 3-4 mm deep.(Fig. 2) Symptoms associated with maxillary sinusitis, e.g., headache, runny nose, nasal congestion, and post-nasal drip, were not observed. The panoramic radiography revealed that two-thirds of the root of the right maxillary molar had subsided into the sinus. Severe sinus pneumatization was detected, but sinusitis-related complexity was not observed. The CT scan showed that one-third of the root of the upper first molar was fused with alveolar bone, and fusion with sinus septa was observed in particular. The inside of the sinus was clean, and no lesion such as mucous retention cyst was found.(Fig. 3) The patient and her guardian were advised with regard to the surgical procedure, and then surgical tooth extraction and bone grafting via the lateral approach to the sinus were performed.
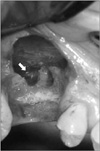
Under 2% lidocaine local anesthesia, two vertical cuts around the upper right first molar and crestal incision were made. Flap elevation was performed; the thin sinus bone wall around the buccal root of the ankylosed molar was noted. Using a bone rongeur, the full wall of the sinus was removed, and the sinus membrane linked with the root was carefully elevated.(Fig. 4) In the course of separating the sinus membrane from the root, a small perforation 0.3×0.3 mm occurred, but it was automatically restored with the sufficient elevation of the sinus membrane. Using a piezoelectric device (Surgybone; Silfradent, Santa Sofia, Italy), the fused sinus septa-root complex was incised, and the tooth piece and septa bone were successfully removed.(Fig. 5) Foreign matter such as Gutta-percha was completely removed as well.(Fig. 6) The sinus membrane was reinforced with absorbent collagen membrane (Biogide; Geistlich Biomaterial, Wolhusen, Switzerland), and 2 cc of allograft material (Orthoblast II; Isotis, Irvine, CA, USA) was placed in the elevated sinus space and the socket.(Fig. 7) Tension-free primary closure was achieved with a buccal advancement flap formed with a releasing incision.(Fig. 8) Antibiotic, non-steroidal, anti-inflammatory agent and nasal decongestant were prescribed for one week. Since the patient was still in the physical development stage, future treatment includes implant placement after the completion of her bone development at a private dental clinic in the vicinity.(Figs. 9, 10)
III. Discussion
The treatment of an ankylosed tooth is not an easy task since the surgery itself is difficult and patient age and ankylosis location must be considered. Chaushu et al.19 suggested some treatment methods for maxillary molars with infraocclusion: periodic observation, surgical removal, prosthetic restoration, and orthodontic treatment. Raghoebar et al.20 suggested that prosthetic restoration is advantageous for adult patients, but that it means limited vertical growth of the alveolar bone around the ankylosed tooth for young patients, possibly leading to a worse ankylosed condition; in such case, they recommend surgical removal instead. To assure proper vision and accessibility for tools, the extrac-tion of an ankylosed tooth should be done through surgical extraction. During treatment, a wide range of alveolar bone of the affected tooth needs to be cut for the successful removal of the ankylosed root. Such extensive surgery causes significant impairment to the bone around the affected tooth. Furthermore, in the maxillary posterior region, it poses consequential risk, i.e., oro-antral fistula in the event of surgical extraction of the ankylosed tooth or displacement of root fragments into the sinus. Regardless of the clean extraction of the ankylosed tooth, future site development, e.g., sinus bone graft for implantation, should be considered.
In this case, via the lateral approach to the sinus, direct access to the ankylosed root was attempted for tooth extraction; at the same time, bone grafting was performed for future implant placement. This enables assured direct sight and access and facilitates future site development for subsequent implant placement, ultimately foregoing the need for additional pre-implant surgery. The most important condition for wise sinus bone grafting is to conserve the sinus membrane. For this, the author used a piezoelectric device, enabling conserving safely the sinus membrane during the removal of the sinus septa. In this case, during surgery, a small perforation occurred in the sinus membrane, but such small sinus membrane perforation gets naturally fixed upon sinus elevation in most cases. Here, what matters is not to cause a large perforation. Without tool manipulation in the perforated area, forming a slightly bigger bone window ensures the safe elevation of membrane; eventually, the reduced perforation naturally closes. Even with the natural closing of the perforated membrane, however, sinus membrane makeup is recommended using absorptive membrane. If a large perforation occurs, it is good to delay bone grafting.
In this case, the timing for implant placement can become a crucial point. Implantation is not recommended for patients in the developing stage except those with congenital diseases, e.g., (partial) edentia. Since implant placed at a young, tender age acts like an ankylosed tooth, delayed implantation until the full completion of physical development is recommended in general. Similar to this surgical treatment, sinus elevation in case of tooth extraction and accompanied bone grafting can help in future implant work. Depending on the growth, however, bone volume fluctuation is actually difficult to predict. Consequentially, this issue is to be considered even though such surgical method may decrease the volume for future bone graft, and additional bone graft may be necessary for implant placement following developmental completion.
In conclusion, the direct approach to the lateral sinus can be a desirable treatment for simultaneous sinus floor augmentation for the extraction of an ankylosed maxillary molar and future implant placement. The appropriate use of a piezoelectric device can be expected to ensure the effective removal of tooth-bone complex while conserving the sinus membrane.







 XML Download
XML Download