

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pre-eclampsia (PE) is a heterogeneous disease defined by the onset of hypertension and proteinuria after 20 weeks' gestation, affecting 2–5% of pregnancies worldwide [123]. The clinical presentation and outcome of PE is variable, and early-onset severe and rapidly progressive PE with pre-term delivery to late-onset PE have been described [4]. PE remains an important cause of maternal and fetal/neonatal morbidity and mortality. Indeed, severe and life-threatening complications such as intrauterine growth restriction (IUGR), eclampsia, and HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count) can occur [4]. Clinical management can be challenging because of the lack of effective treatment options other than delivery.
The pathogenesis of PE is multifactorial and not fully understood. However, abnormal remodeling of maternal spiral arteries is observed in women with subsequent PE, leading to placental hypoperfusion and systemic endothelial dysfunction [5]. Placental dysfunction leads to altered circulating levels of pro-angiogenic or anti-angiogenic mediators, notably placental growth factor (PlGF), soluble endoglin and the soluble fms-like tyrosine kinase receptor-1 (sFlt-1), and a truncated and soluble form of vascular endothelial growth factor (VEGF) receptor, which neutralizes VEGF and PlGF. Hence, PE and its complications may occur because of an imbalance in circulating angiogenic factors [6].
Levine et al [7] showed that five weeks before development of clinical symptoms of PE, serum concentrations of s-Flt-1 are increased, whereas PlGF concentrations are decreased, resulting in an increased s-Flt-1/PlGF ratio. Increased sFlt-1 levels and reduced PlGF levels can be used to predict the subsequent development of PE.
While increasing data are becoming available and promising results have been observed for sFlt-1 and PlGF, soluble endoglin and VEGF have not been shown to be clinically effective for managing PE. Despite its pathophysiological implications, no specific increase in soluble endoglin in the context of PE or HELLP syndrome has been demonstrated [8]. The use of VEGF as a tool for managing PE appears to also be compromised. There are analytical difficulties in the measurement of VEGF because of the different assays available for total or free, biologically active VEGF measurement [9].
The potential relevance of determining s-Flt-1, PlGF, and the s-Flt-1/PlGF ratio for the diagnosis and prognosis of the disease has been investigated to help physicians identify patients at high risk of PE who require close monitoring. Interestingly, the sFlt-1/PlGF ratio appears to show better performance than single markers in predicting the risk of PE [1011]. Several strategies have been investigated for first trimester screening of women at high risk of PE to introduce, if applicable, low-dose acetylsalicylic acid and during the second trimester or later, to predict or rule out the diagnosis of PE [12].
Additionally, a major prospective clinical trial validated cut-offs for the sFlt-1/PlGF ratio for the management of PE in the PROGNOSIS study (Prediction of Short-Term Outcome in Pregnant Women with Suspected Preeclampsia Study), which clearly demonstrated that an sFlt-1/PlGF ratio of 38 or lower can be used to rule out the onset of PE within one week, independently of gestational age [13]. The negative predictive value was 99.3% [13]. Furthermore, a sFlt-1/PlGF ratio greater than 85 (for early-onset PE, <34 weeks of gestation) or 110 (for late-onset PE, ≥34 weeks) is indicative of a high risk of PE diagnosis or placenta-related disorders requiring close clinical and biological monitoring. For women with a sFlt-1/PlGF ratio between 38 and 85 or between 38 and 110, current PE can be ruled out; however, these women carry a high risk of developing PE within four weeks [14].
Despite the simplicity of defining PE, which has recently been debated [15], several clinical situations are also relatively complex to assess in ruling out PE diagnosis: women with pre-existing nephropathy and presenting with chronic proteinuria, women with chronic pre-pregnancy hypertension and IUGR, development of hypertension without proteinuria or the opposite, and hypertension with thrombocytopenia or hepatic cytolysis without proteinuria. Because of current difficulties in diagnosing PE and conducting early identification of women at high risk of PE, other biological markers are necessary; sFlt-1 and PlGF appear to be excellent candidates in this context.
The objective of this study was to evaluate the routine use of sFlt-1, PlGF, and the sFlt-1/PlGF ratio in a specific population of high-risk patients, including multiple pregnancies, in clinical practice to improve care and prognosis for these patients.
METHODS
This mono-centric, prospective, non-interventional study was conducted from January to May 2014 in the specialized perinatal care center of the Department of Gynecology and Obstetrics in Nantes University Hospital, France. Patients did not object to taking part in the study. Written informed consent was obtained from each patient. The local ethics committee of the University Hospital of Nantes approved the study (No. RC13_0283).
1. Inclusion and exclusion criteria
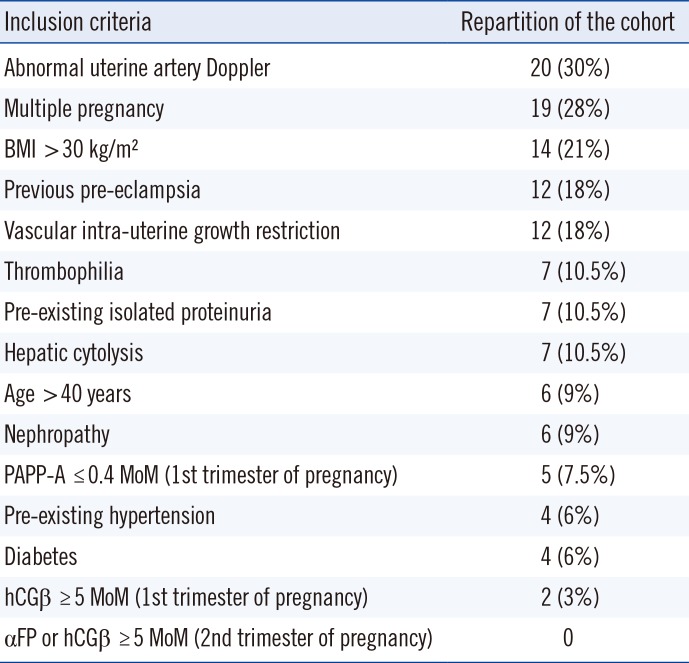
All adult patients with ongoing pregnancy between 20 and 37 gestation weeks and with at least one risk factor were eligible (Table 1). Women with a confirmed diagnosis of PE at the specified gestation period were excluded from the study. During the enrollment period, 75 patients were included, and eight were excluded: seven did not meet the inclusion criteria (two for completing over 37 weeks of gestation, and five for already being diagnosed with PE) and one was excluded for medical termination of pregnancy. A total of 67 women were included in the study over 5 months.
2. Serum markers of PE
Once consent was obtained, an additional blood sample was collected during routine check-up to determine serum sFlt-1 and PlGF concentrations and calculate the sFlt-1/PlGF ratio. Blood was collected in a standard serum tube: samples were centrifuged and stored at −20℃ until analysis. Serum samples were analyzed within six months of storage. sFlt-1 and PlGF concentrations were measured in the Clinical Biochemistry Laboratory of Nantes University Hospital, using an electrochemiluminescence Elecsys immunoassay on a Roche Diagnostics Cobas e411 system (Roche Diagnostics, Mannheim, Germany). Each run was validated by measuring two levels of quality control material prior to starting the experiment. The reference range (5th–95th percentile) was defined by Roche Diagnostics in a cohort of 877 women ongoing normal single pregnancy from nine European centers (Germany, Spain, Austria, Czech Republic, and Switzerland) leading to 1,685 samples analyzed. PlGF and sFlt-1 assays previously demonstrated strong characteristics in terms of inter- and intra-assay precision with total imprecision CV below 5% [16].
3. Judgment criteria
The main endpoint was the occurrence of PE with hypertension (≥140/90 mmHg) and proteinuria (≥0.30 g/24 hours) and/or related complications such as HELLP syndrome or eclampsia. The secondary objective of this study was to evaluate the sensitivity, specificity, and negative and positive predictive values of sFlt-1/PlGF ratio of 38, as determined in the PROGNOSIS study, in the specific population of high-risk pregnancies.
In this high-risk population, a prevalence of 15% of PE was expected. Considering a specificity of 95% for the sFlt-1/PlGF ratio with an accuracy of 5%, 86 inclusions were necessary. Taking into account that 2% of the biomarker results would not be analyzable, our goal was to include 88 patients to ensure the desired accuracy.
4. Statistical analysis
Data from patients' clinical histories and serum markers of PE were collected in a database using Microsoft Excel 2010 software (Microsoft Corporation, Redmond, WA, United States). All the data in this study are presented as mean±SD. Sensitivity, specificity, and positive and negative predictive values were determined, and a contingency table was prepared. Statistical analysis according to PE status was performed using MedCalc software for Windows, version 15.0 (MedCalc Software, Ostend, Belgium). Kruskal-Wallis test was conducted to analyze continuous variables and Fisher's exact test for categorical variables. A P value below 0.05 was considered statistically significant.
RESULTS
1. Description of the population
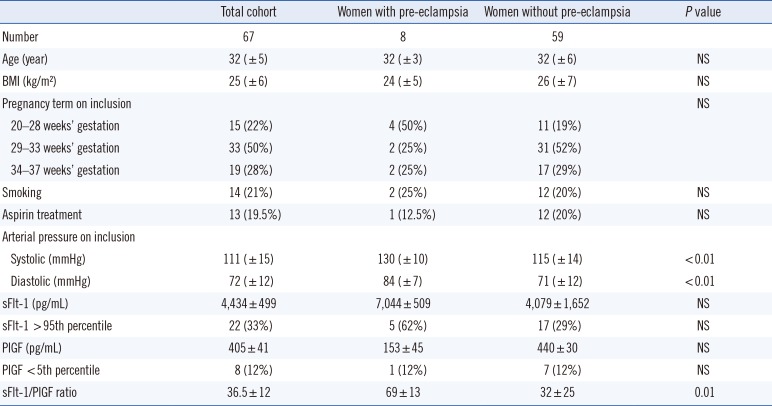
A total of 67 women were included in the study over five months. All women had at least one risk factor. An abnormal uterine artery Doppler (notch or/and high pulsatility index) was the most common risk factor (N=20; 30%). Seven patients (10.5%) with pre-existing isolated proteinuria and four patients (6%) with pre-existing chronic hypertension were included. The mean age was 32 years (±5 years). Inclusion criteria and cohort distribution according to these criteria are shown in Table 1. Among the cohort of 67 patients, eight developed clinical PE: five before 34 gestation weeks, one between 34 and 37 weeks, and two after 37 weeks. The demographic and clinical characteristics of the cohort, shown in Table 2, did not significantly differ between the two groups, except for arterial blood pressure.
2. Serum markers of PE
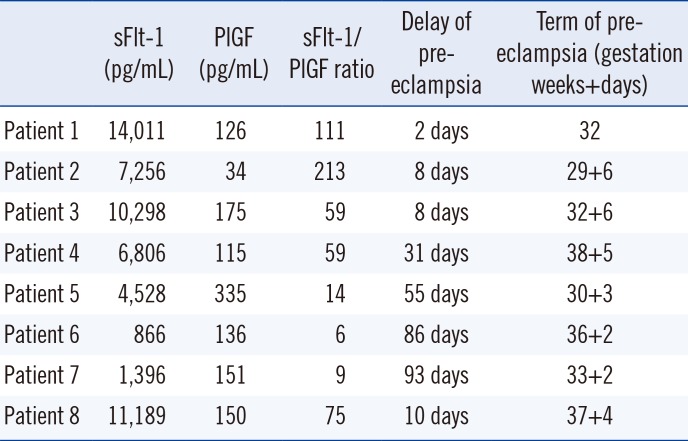
sFlt-1 and PlGF concentrations and sFlt-1/PlGF ratio assessments are shown in Table 2. Twenty-two patients (33%) had a sFlt-1 concentration higher than the 95th percentile, with five (62%) in the pre-eclamptic group. For PlGF, eight patients (12%) had a concentration lower than the 5th percentile, with one in the PE group (12%). The mean sFlt-1/PlGF ratio was 36.5±12 for the entire cohort, which was significantly higher (69±13) for women who developed PE than for women without PE (32±25) (P=0.01). Individual results for women with PE are shown in Table 3.
3. Predictive performances
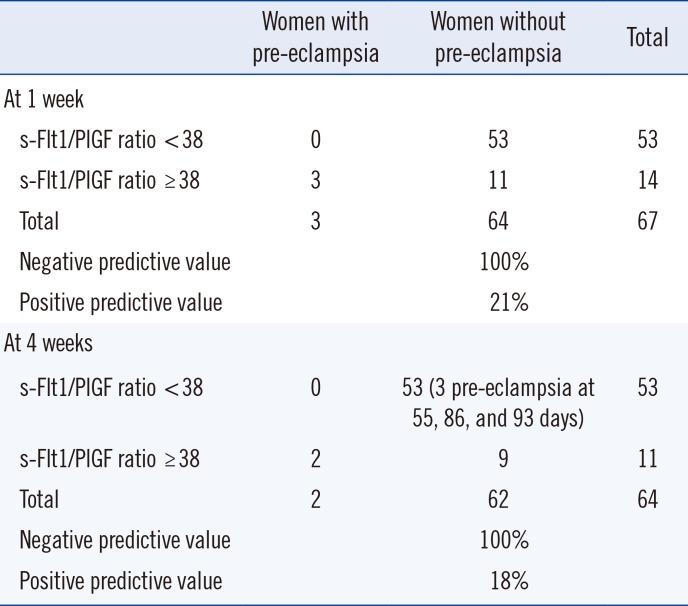
For a sFlt-1/PlGF ratio threshold of 38, 14 women exhibited a high sFlt-1/PlGF ratio (Table 4). Among them, three developed PE within less than one week (two days for one patient, eight days for two patients). The negative predictive value of the sFlt-1/PlGF ratio at one week with a threshold at 38 was 100%; the positive predictive value was 21%. Sensitivity and specificity were 100% and 83%, respectively (Table 4).
Concerning the risk of PE occurring within four weeks at the same threshold and after excluding the three patients who presented with PE before one week, two of the remaining patients developed PE (one patient at 10 days and the other at 31 days). The negative predictive value of the ratio for the risk of PE occurring at four weeks was 100%; positive predictive value was 18%. Sensitivity was 100%, and specificity was 85% (Table 4).
4. Discrepancies
Among the patients who did not develop PE despite a sFlt-1/PlGF ratio greater than 38, three presented with PE but in atypical form: one patient exhibited symptoms of PE with HELLP syndrome but without hypertension, while two patients had PE without proteinuria.
Three patients with a ratio below 38 developed PE at more than four weeks (55, 86, and 93 days).
DISCUSSION
Our prospective study, conducted in a specialized perinatal care center, demonstrated that the sFlt-1/PlGF ratio can be used to rule out PE in a specific population of high-risk patients with excellent negative predictive value. Our negative predictive value for ruling out PE within one week was 100%, in accordance with that from the PROGNOSIS study (99.3%) [13]. The aim of using the sFlt-1 and PlGF biomarkers is to rule out PE onset, avoiding unnecessary hospitalization and identifying high-risk pregnant women who require intensive monitoring. Use of the two serum biomarkers and their ratio appears to be essential for pregnant women at high-risk of PE or when diagnosis of PE is difficult because of the absence of symptoms or pre-existing diseases.
In fact, hypertensive disorders other than PE such as gestational hypertension or chronic hypertension can occur during pregnancy. The onset of hypertension during pregnancy or worsening of pre-existing chronic hypertension without proteinuria represents a complex situation, in which it is essential to rule out PE. Verlohren et al [17] showed that the sFlt-1/PlGF ratio in patients with PE is significantly higher compared with that in patients with chronic and gestational hypertension. These data, recently confirmed in a Spanish cohort [17], demonstrated the role of the sFlt-1/PlGF ratio in differentiating PE and other pregnancy-related hypertensive disorders [18].
Thus, because both PE and chronic kidney disease (CKD) are characterized by proteinuria, hypertension, and progressive renal impairment, differential diagnosis may be difficult during pregnancy. Rolfo et al [19] evaluated the potential value of using sFlt-1 and PlGF to differentiate between CKD and PE. They demonstrated that women with CKD exhibited normal levels of sFlt-1, PlGF, and sFlt-1/PlGF ratio. The sFlt-1/PlGF ratio was generally significantly higher in subjects with PE than in those with CKD, suggesting that serum biomarkers can be used to distinguish these two diagnoses [19]. Ghosh et al [20] also demonstrated that serum PlGF measured in the early second trimester of pregnancy may be an effective predictor of early-onset PE in another group of high-risk pregnant women who are overweight or obese rather than in normal or underweight women.
Serum sFlt-1 and PlGF PE markers and their ratio show highly predictive performance for clinical care. In addition to the many advantages described above, they are easier to use than uterine artery Doppler and represent an additional method of management in clinical practice. In fact, establishing velocimetric parameters is relatively straightforward. However, uterine artery Doppler has several weaknesses: reproducibility is limited, the resulting indices vary with the anatomical site of insonation, and uterine artery blood flow can be difficult to measure accurately by Doppler sonography [21]. Recent studies have demonstrated the poor sensitivity of using only second-trimester Doppler ultrasound measurements for general prediction of PE in a well-characterized, low-risk, nulliparous population [22]. However, some studies suggested that combining the uterine artery pulsatility index with PlGF and sFlt-1 may be useful for predicting PE [2324].
The actual impact and clinical usefulness of the sFlt-1 and PlGF biomarkers in pregnant women with suspected PE was evaluated in the pre-eclampsia open study (PreOS). sFlt-1/PlGF ratio results led to a change in the decision to hospitalize women for 16.9% of the cohort (20/118). These results demonstrated the usefulness of the sFlt-1/PlGF ratio for clinical decision-making of hospitalization in a considerable proportion of women with suspected PE. In addition to improving clinical care, assessment of the sFlt-1/PlGF ratio helps avoid unnecessary stress and anxiety for the patient. Reducing unnecessary hospitalizations is a major consideration in the current context of a heavy financial burden in many healthcare institutions [25]. The economic impact of introducing sFlt-1 and PlGF for managing PE appears to be positive. In the PROGNOSIS study by Vatish et al [26], hospitalizations were reduced by more than a half, generating cost-savings of £344 per patient. The expected annual cost savings for the UK National Health Service would be approximately £24 million per annum, based on a cohort of 68,900 women presenting annually with hypertensive disorders including suspected PE [26].
Based on this data, the National Institute for Health and Care Excellence (NICE) guidance recommends sFlt-1/PlGF ratio testing to rule out PE in women presenting with suspected PE between 20 and 34+6 gestation weeks. However, there is currently insufficient evidence and some contradictive recent data preventing their routine use in diagnosing PE [2728]. An intermediate and rational method of introducing the sFlt-1/PlGF ratio into clinical practice as a first step, and with respect to the currently relatively high cost, would be to reserve these markers for high-risk populations with suspected PE or for differential diagnosis.
Our study has some limitations, such as the size of the cohort, heterogeneity of the patients included, the mean age of the patients, and influence of multiple pregnancies. Nevertheless, it represents a practical population. The mean age of the patients was 32±5 years with 34 patients out of 67 (50%) aged 30–35 years. Indeed, hypertensive disorders and HELLP syndromes are known to be associated with increasing maternal age during gestation. Concerning multiple pregnancies, 19 patients (28%) in our population had at least a twin pregnancy. Dröge et al [29] reported that women with twin pregnancy who did not develop PE had a higher median serum sFlt-1 concentration and sFlt-1/PlGF ratio than women with singleton pregnancies; however, the median serum PlGF concentration was unchanged. For patients with twin pregnancy and PE, the median sFlt-1/PlGF ratio was not significantly different compared with singleton pregnancies with PE. Current cut-offs for the diagnosis of PE were established using data from singleton pregnancies alone, which, based on our results, appears to be inappropriate: Dröge et al [29] suggested a threshold of 53 as an optimal cut-off for this patient category.
Broader use of the sFlt-1/PlGF ratio in maternity care may support targeted clinical care by helping to identify women who are at high risk of developing PE and require close monitoring and management from women who are at a low risk of developing PE and can simply be reassured, thus avoiding unnecessary hospitalization [25].
This study demonstrated that a cut-off of 38 for the sFlt-1/PlGF ratio is appropriate for ruling out PE in a representative cohort of high-risk patients. Use of the sFlt-1/PlGF ratio in clinical practice will improve management of the disease and reduce health expenditures, while ensuring safety.
 XML Download
XML Download