

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Antibodies specific to human neutrophil antigens (HNA), especially HNA-2 antibody, are implicated in alloimmune neonatal neutropenia (ANN), autoimmune neutropenia (AIN), transfusion-related acute lung injury (TRALI), drug-induced neutropenia, and graft failure after bone marrow transplantation [12]. The HNA-2 antigen is located on the CD177 glycoprotein and is expressed specifically on neutrophils [123]. In HNA-2-positive individuals, two neutrophil subpopulations can be identified based on CD177 expression [456]. HNA-2-negative or HNA-2-null individuals do not express CD177 on neutrophils [7]. The frequency of HNA-2-positive individuals exceeds 90%, while the HNA-2-null phenotype varies between 0.0% and 2.0% among different populations. Interestingly, among eastern Japanese, Korean, and French populations, the frequency of HNA-2 null is 11.5% to 14.0% [8910]. HNA-2 expression varies among individuals, ranging from 0% to 100%, and is slightly higher in women than in men. HNA-2 expression decreases in elderly women, but not men [1112], and is reportedly increased in newborns, pregnant women, healthy people receiving granulocyte-colony-stimulating factor, and patients with severe bacterial infections and chronic myeloproliferative disorders [1314151617].
Various techniques are used to detect HNA-2 antigen and antibodies. The combination of granulocyte agglutination test (GAT) and granulocyte immunofluorescence test (GIFT) is recommended for HNA antibody screening. Monoclonal antibody-specific immobilization of granulocyte antigens (MAIGA) assay is used to confirm antibody specificities [218]. However, the requirement for fresh granulocyte panels is a limitation of serological techniques. Regarding antigen detection, owing to the unavailability of specific antisera, various molecular techniques have been implemented to detect single nucleotide polymorphisms (SNPs) in HNA-1-, HNA-3-, HNA-4-, and HNA-5-encoding genes [56]. For the HNA-2 system, CD177 polymorphism is reportedly associated with different patterns of antigen expression; however, it remains inconclusive whether CD177 polymorphism determines HNA-2 deficiency [47192021]. Hence, molecular techniques are not able to distinguish HNA-2-positive and HNA-2-null individuals.
Flow cytometry is widely used for determining HNA-2 expression. This study aimed to investigate the HNA-2 phenotype frequencies among Thai blood donors by using a simple flow-cytometric analysis and to compare the relationships of sex and age with HNA-2 expression.
Go to : 
METHODS
1. Study population
This study involved 220 unrelated, healthy Thai blood donors who visited the blood bank of Thammasat University Hospital from November 2016 to April 2017, including 150 males and 70 females, with the median age of 38 years (range 20–57 years). Peripheral blood samples were collected in EDTA-anticoagulant tubes for HNA-2 expression analysis. Informed consent was obtained from each subject. This study was approved by the Committee on Human Rights Related to Research Involving Human Subjects, Thammasat University, Thailand (IRB No.132/2557).
2. Antibodies
Phycoerythrin (PE)-conjugated antibody specific for CD177 (clone MEM-166; BD Biosciences, Franklin Lakes, NJ, USA) and fluorescein isothiocyanate (FITC)-conjugated antibody specific for human CD45 (clone 2D1; BD Biosciences) were used for neutrophil staining. Isotype control antibodies including PE-mouse IgG1, κ (clone MOPC-21; BD Biosciences) and FITC-mouse IgG1, κ (clone MOPC-31C; BD Biosciences) were used to determine non-specific binding of antibodies. All antibodies were titrated before use to determine the concentration giving minimum saturation binding.
3. Isolation of polymorphonuclear cells (PMNs)
PMNs were isolated using Polymorphprep (AXIS-SHIELD; Alere Technologies AS, Oslo, Norway). Briefly, 3 mL of blood sample was overlaid on 3 mL of Polymorphprep in a 15-mL conical tube. Samples were centrifuged at 2,500 rpm, 25℃ for 35 minutes in a Universal 320/320R swing-out rotor centrifuge (Hettich Lab Technology, Tuttlingen, Germany). Following centrifugation, two layers, including a top layer of mononuclear cells and a lower layer of PMNs, separately appeared as white interfaces. The PMN layer was collected and the cells were washed twice with 2 mL of RPMI 1640 incomplete medium (Thermo Scientific, Waltham, MA, USA). To determine cell viability, the PMNs were stained with 0.4% trypan blue in phosphate-buffered saline (pH 7.2), and the number of viable cells was counted using a hemocytometer. At least 1×106 cells/mL of PMNs was used to investigate HNA-2 expression.
4. Antibody staining
For antibody staining, 100 µL of PMN suspension was incubated with 2.5 µL of human CD177-PE and CD45-FITC antibodies on ice for 20 minutes. After incubation, the cells were washed twice with RPMI 1640 medium and centrifuged at 1,500 rpm, 4℃ for 5 minutes. The supernatant was discarded, and the pellet was resuspended in 100 µL RPMI 1640 medium for flow-cytometric analysis.
5. Flow-cytometric analysis
The stained neutrophils were analyzed for fluorescence intensity using a BD FACSVERSE flow cytometer (Becton Dickinson, Franklin Lakes, NJ, USA). Single-color controls of human CD177-PE and CD45-FITC antibodies were used to set compensation. In addition, isotype control antibodies were used to determine nonspecific binding of antibodies and to set gates. HNA-2 expression was analyzed using FlowJo software (FlowJo, Ashland, OR, USA). Variations in HNA-2 expression were observed by flow cytometry using the CD177 (MEM-166) antibody.
Total PMNs were initially defined by gating of CD45 and side scatter (SSC). Populations of CD45high/SSC cells were further gated to determine the expression of CD177. According to previous reports, an individual was regarded HNA-2-negative when less than 5% of neutrophils were reactive to the CD177 antibody [1220].
6. Statistical analysis
A two-tailed t-test was used to compare the expression of antigens among different sex and age groups. The subjects were grouped in four categories based on antigen expression, according to a previous report [20]: group 1, ≥60% (strong expression); group 2, 40–59.9% (intermediate expression); group 3, 5–39.9% (weak expression); and group 4,<5% (negative reaction). HNA-2 phenotype frequencies were compared with those previously reported for other populations by using a chi-square test [8910111222232425]. Statistical analyses were conducted using SPSS (Version 16.0, SPSS Inc., Chicago, IL, USA). A P value ≤0.05 was considered statistically significant.
Go to :
RESULTS
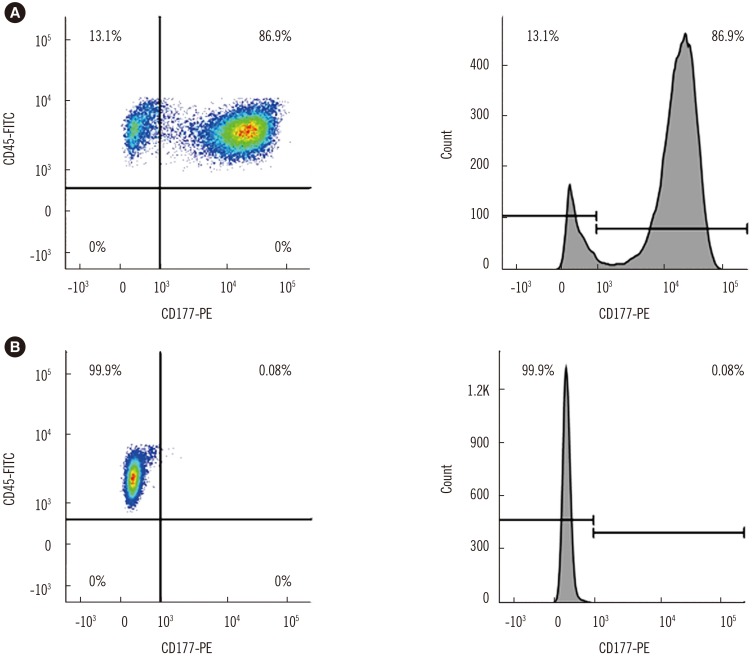
1. CD177 expression on neutrophils from healthy donors
CD177 expression was in the range of 0.08–97.90% (66.60±18.10%). Two populations of neutrophils in terms of CD177-MEM-166 reactivity, with variation in HNA-2 expression, could be distinguished (Fig. 1). Among the 220 Thai blood donors, 219 were HNA-2 positive (99.55%) and one male donor was HNA-2 negative (0.45%).
2. Effects of sex and age on HNA-2 expression
Mean antigen expression was significantly higher in women (71.01±15.46%) than in men (64.59±18.85%) (t-test=−2.669; 95% CI: −11.17 to −1.70; P <0.05). The distribution of HNA-2 expression showed no significant differences among age groups (Table 1).

Table 1
Distribution of HNA-2 expression among healthy Thai blood donors stratified according to sex and age
![]()
3. Comparison of HNA-2 phenotype frequencies among populations
HNA-2 phenotype frequencies in the Thai population were compared with those reported previously for Asian and other ethnic populations [8910111222232425] (Table 2). The HNA-2-positive phenotype had the highest incidence among populations, and its frequency in our study population was similar to that in Chinese, Taiwanese, Japanese, African, American, and Brazilian populations [111222232425], but significantly higher than that in eastern Japanese, Korean, and French populations (P <0.001) [8910].
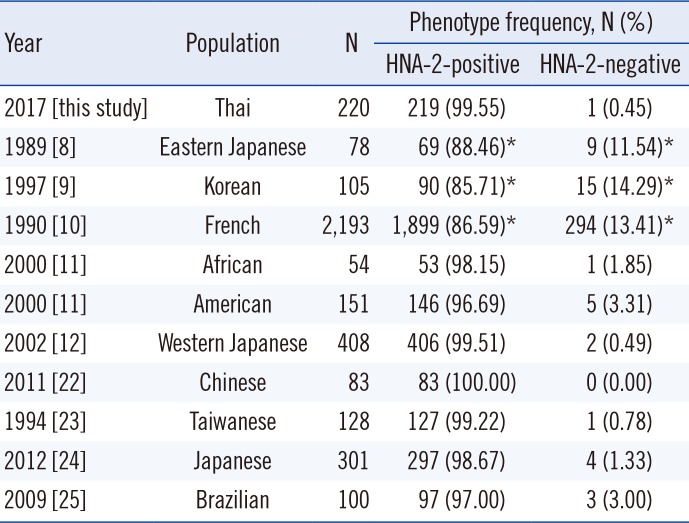
Table 2
HNA-2 phenotype frequencies among different populations
| Year | Population | N | Phenotype frequency, N (%) | |
|---|---|---|---|---|
| HNA-2-positive | HNA-2-negative | |||
| 2017 [this study] | Thai | 220 | 219 (99.55) | 1 (0.45) |
| 1989 [8] | Eastern Japanese | 78 | 69 (88.46)* | 9 (11.54)* |
| 1997 [9] | Korean | 105 | 90 (85.71)* | 15 (14.29)* |
| 1990 [10] | French | 2,193 | 1,899 (86.59)* | 294 (13.41)* |
| 2000 [11] | African | 54 | 53 (98.15) | 1 (1.85) |
| 2000 [11] | American | 151 | 146 (96.69) | 5 (3.31) |
| 2002 [12] | Western Japanese | 408 | 406 (99.51) | 2 (0.49) |
| 2011 [22] | Chinese | 83 | 83 (100.00) | 0 (0.00) |
| 1994 [23] | Taiwanese | 128 | 127 (99.22) | 1 (0.78) |
| 2012 [24] | Japanese | 301 | 297 (98.67) | 4 (1.33) |
| 2009 [25] | Brazilian | 100 | 97 (97.00) | 3 (3.00) |
![]()
Go to :
DISCUSSION
In this study, we developed a single-step method for HNA-2 phenotyping by flow cytometry using anti-human CD177 and CD45 monoclonal antibodies. Owing to the PMN preparation procedure used and CD45/SSC gating, monocyte contamination during neutrophil isolation was minimized. Additionally, two isotype control antibodies were used to determine non-specific antibody binding and to maximize the ability to discriminate between positive and negative neutrophil populations [26]. Hence, HNA-2-positive and HNA-2-negative individuals could be identified according to the percentage of antigen expression (≥5% and <5%). Various CD177 antibodies have been used for HNA-2 phenotyping, including 1B5, TAG4, MEM-166, and 7D8 [111227]. In this study using CD177 (MEM-166), we identified a single peak representing HNA-2-expressing neutrophils in flow-cytometric analysis. In contrast to previous reports, we identified no subpopulations with heterogeneous expression [112027]. HNA-2 phenotyping using flow-cytrometric analysis has a few limitations in that the instrument is expensive and the blood samples need to be processed within 24 hours.
Regarding the effects of sex and age on HNA-2 expression among the 220 Thai blood donors, HNA-2 expression was significantly higher in women than in men, in accordance with findings in Japanese and Brazilian populations [111220]. These results revealed that estrogen levels might affect HNA-2 expression. In a Japanese population, HNA-2 expression reportedly decreased with age in women, while it remained constant in men [11]. In contrast, no association with age was found in both sexes in the current study, similar to previous findings in a Brazilian population [20]. The frequency of the HNA-2-positive phenotype resembled that in Asian, African, American, and Brazilian populations [111222232425] and was significantly higher than that in eastern Japanese, Korean, and French populations [8910]. This finding confirms that alloimmunization and clinical disorders, especially, ANN and TRALI, caused by antibodies against HNA-2 may be less probable than those caused by other HNA antibodies in Thais [28]. Further studies in unrelated healthy donors from different regions of Thailand are required to confirm this finding.
In conclusion, this is the first report of HNA-2 phenotype frequencies in a Thai population determined by flow-cytometric analysis. The data would be helpful in predicting the risk of HNA-2 alloimmunization and in recruiting granulocyte panel donors.
Go to :
 XML Download
XML Download