

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor,
The G antigen (Rh12) is a member of the Rh system of blood group antigens expressed on red blood cells (RBCs) possessing C or D antigens. Anti-G mimics the anti-C+D pattern but cannot be serologically differentiated, since it is adsorbed by both C−D+ and C+D− RBCs [1]. We report the first case of anti-G identified in a Korean man and provide a brief review of the literature on its clinical significance. Informed consent was not required for this report, and IRB approval was exempted.
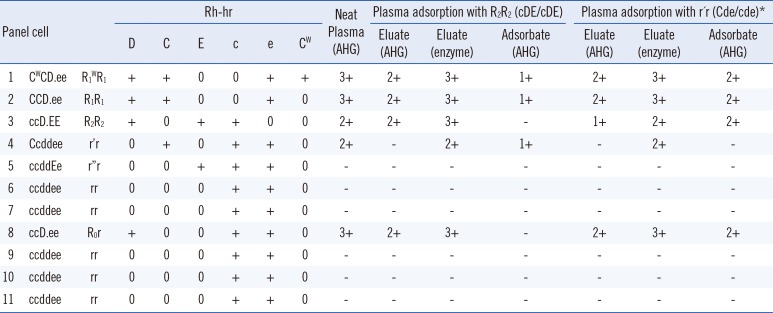
A 78-year-old Korean male patient visited the outpatient department of a tertiary hospital in Seoul for preoperative risk evaluation in June 2016. He had a medical history of RBC transfusion performed in 1958 following a car accident. Antibody screening test was performed with ID-DiaCell I-II (Bio-Rad, Cressier, Switzerland) and ID-Card LISS/Coombs (Bio-Rad), revealing positive results in both panels of cells (CDe/CDe, 3+; cDE/cDE, 2+). The patient's ABO blood group was O, and the Rh phenotype was determined to be D−C−E−c+e+. The antibody identification test using ID-DiaPanel (Bio-Rad) and ID-Card LISS/Coombs revealed an anti-C+D pattern (Table 1). Additional adsorption-elution tests were conducted using the patient's plasma to discriminate among the combinations of anti-C, anti-D, and anti-G.
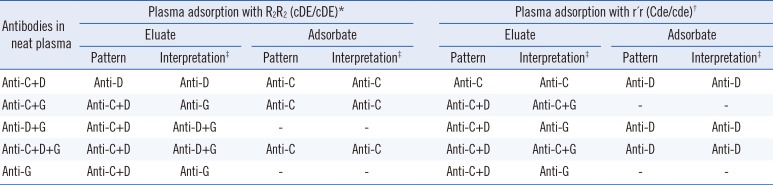
For these tests, instead of the conventional method described by Issitt [23], we adopted a different strategy and conducted parallel adsorption-elution tests using R2R2 (cDE/cDE) and r´r (Cde/cde) cells (Table 2) [4]. In the plasma adsorbed by R2R2 and r´r cells, the presence of anti-C and anti-D, respectively, was confirmed by antibody identification using the ID-DiaPanel (Table 1). The eluates prepared from the R2R2 and r´r cells both initially showed the anti-D pattern. However, when tested again using papain-treated cells (ID-DiaPanel-P, BioRad), the anti-C+D pattern was detected in both cases (Table 1). We concluded that the patient's antibody profile is anti-C+D+G. The patient underwent robot-assisted laparoscopic radical prostatectomy in July 2016. He did not require any RBC transfusion and was successfully discharged four days after the surgery.
The G antigen was first reported in 1958 [5]. The G-negative phenotype has been associated with a Ser to Pro substitution at residue 103 of Rh polypeptides encoded by a common region in exon 2 of the RHD and RHCe/RHCE genes [6]. This antigen is generally not expressed on RBCs that lack C and D antigens. However, rare cases of RBCs expressing only the G antigen, such as the rGr (cGe/ce) phenotype, have been reported [7]. Thus, anti-G is generally detected in individuals who lack the C and D antigens and have been exposed to these antigens through transfusion, pregnancy, or transplantation.
Anti-G consists of the IgG isotype and may cross the placenta. Although it does not typically bind to complements, cases of severe delayed hemolytic transfusion reaction and hemolytic disease of the fetus and newborn (HDFN) have been reported [278]. Nevertheless, the clinical significance of anti-G is controversial, because it is frequently accompanied by anti-C and/or anti-D, and the severity of associated HDFN varies [9]. Rare cases of isolated mild to moderate HDFN due to anti-G have been reported [910]. Thus, until a better understanding of its clinical relevance is achieved, fetal anemia monitoring should be considered for pregnant women who are confirmed to be anti-G-positive.
Distinguishing anti-G from anti-D and anti-C is important for female children or women of childbearing age, particularly for female patients expressing anti-G and not anti-D. This is because such individuals would require RhIg prophylaxis during pregnancy or the transfusion of platelets from RhD-positive donors to prevent anti-D allo-immunization. The adsorption and elution testing protocols described above do not need to be fully performed if the aim is to simply detect anti-D in these patients. Testing the plasma for anti-D after adsorption by r´r cells is sufficient to decide whether the patient will benefit from RhIg prophylaxis. This simple approach should be convenient and effective for smaller transfusion services. Laboratories with sufficient resources can perform the full antibody differentiation screening process, using either the stepwise protocol based on Issitt's method [23] or the parallel adsorption-elution method shown in Table 2.
This report presents the first case of anti-G alloantibody identification in Korea. Although our patient was a 78-year-old man, transfusion services should be aware that differentiation between anti-D and anti-G is crucial in female children and women of childbearing age for determining the eligibility of RhIg prophylaxis. All pregnant women showing serological anti-C+D reactivity should be further evaluated for anti-G through adsorption-elution testing.
 XML Download
XML Download