

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
METHODS
1. Patients
2. Conventional cytogenetics
3. Probes for interphase FISH
4. Statistical analyses and survival analyses
RESULTS
1. Patient characteristics
Table 1
Clinical and biological characteristics of patients with multiple myeloma
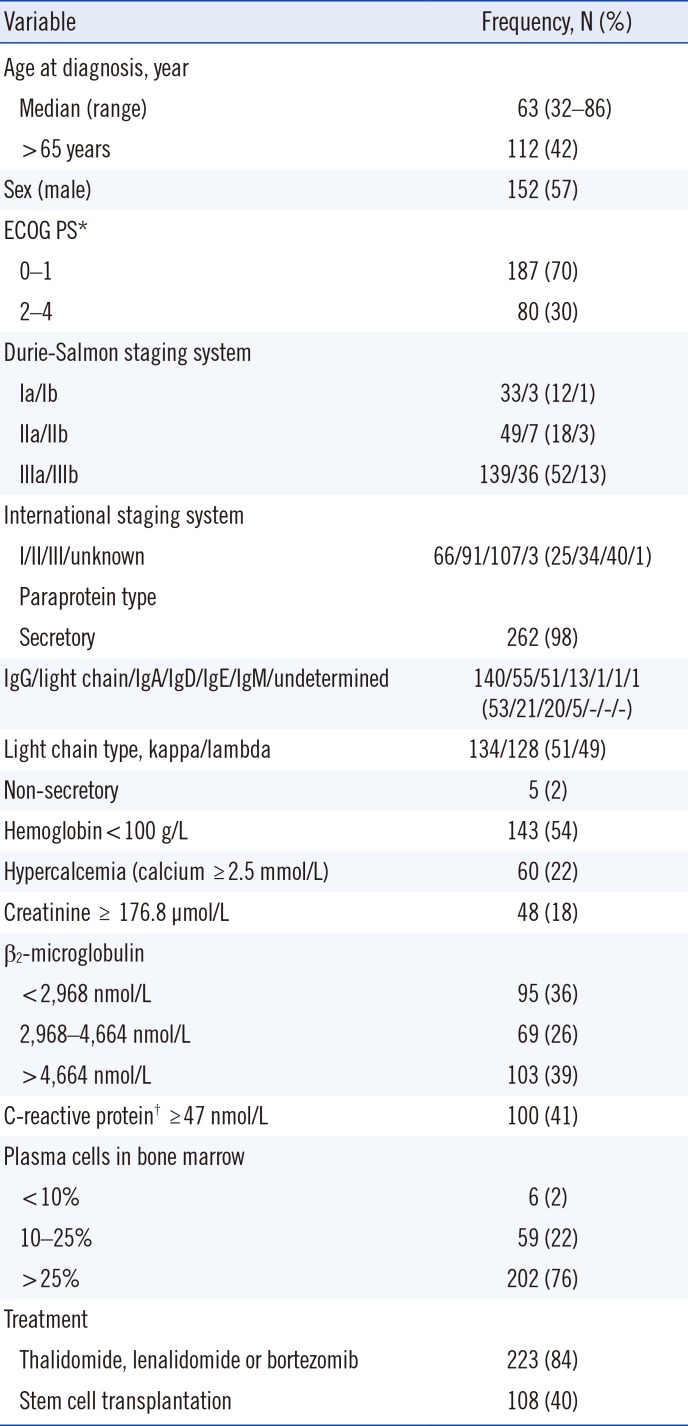
*ECOG PS score is as follows: 0=without symptoms; 1=mild symptoms not requiring treatment; 2=symptoms requiring some treatment; 3=disabling symptoms but allowing ambulation for > 50% of the day; 4=ambulation <50% of the day; †Data available from 244 patients.
Abbreviation: ECOG PS, Eastern Cooperative Oncology Group performance status.
![]()
2. Genetic abnormalities of the patients
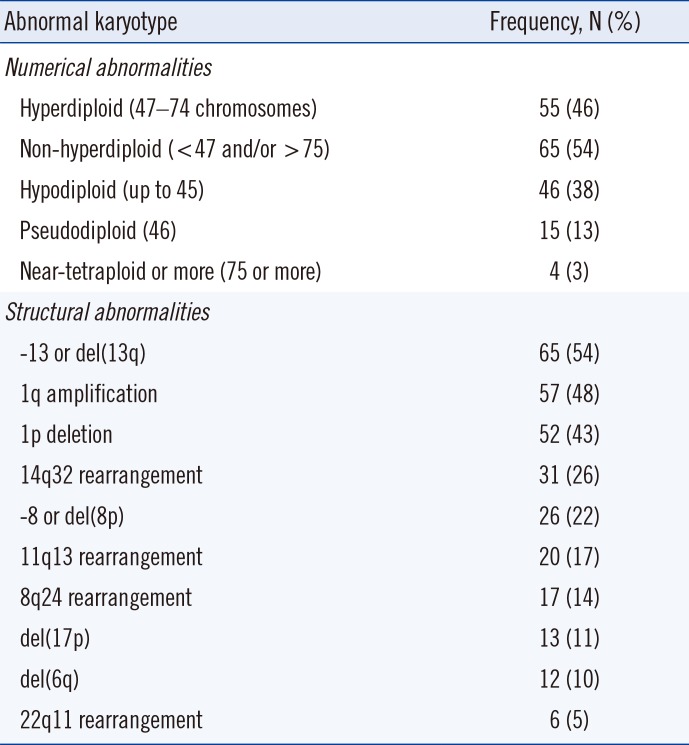
Table 2
Frequencies and distribution of cytogenetic abnormalities in 120 patients with abnormal karyotype
![]()
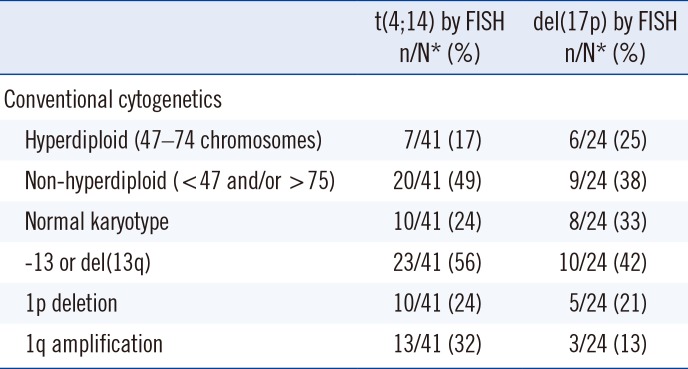
3. Comparison of detection frequencies and distribution of genetic abnormalities observed using cytogenetics, FISH, and comprehensive cytogenetics/FISH approaches
Table 3
Differences in detection frequencies and distribution of the identified genetic abnormalities according to the diagnostic approach of cytogenetics alone, FISH alone, and a comprehensive cytogenetics/FISH approach
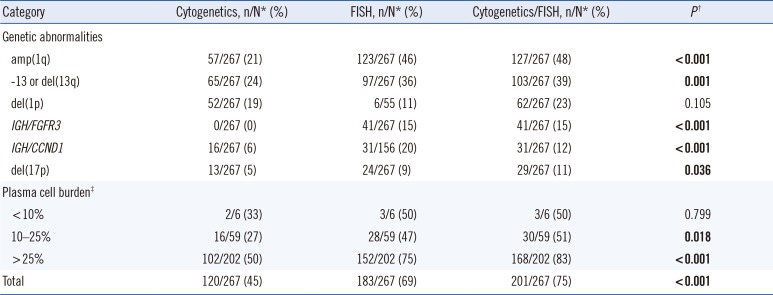
P values for comparison among cytogenetics, FISH, and cytogenetics/FISH groups were calculated using the Chi-square test. When the expected cell value was<5, Fisher's exact test was used. Significant P values are shown in bold.
*n/N indicates the positive number/total number of patients; †Cytogenetics versus FISH versus Cytogenetics/FISH group; ‡Proportion of plasma cells on bone marrow aspirate.
Abbreviations: amp, amplification; del, deletion.
![]()
4. Prognostic significance of the identified genetic abnormalities
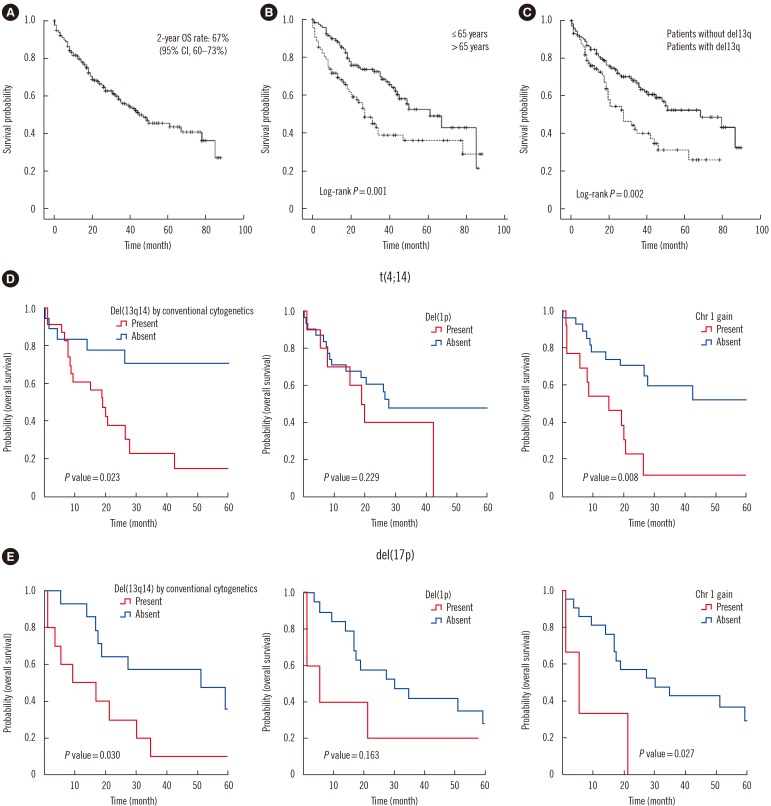
Fig. 1
Kaplan-Meier plots for the overall survival (OS) estimation and prognostic value of t(4;14) and del(17p) in multiple myeloma. (A) The OS rate at two years in 217 patients was estimated at 67%, and the median survival was 45 months (95% confidence interval [CI] 29–61 months). (B) OS according to age: ≤65 years group vs >65 years group (log-rank P =0.001). (C) OS according to the presence of del(13q) (log-rank P =0.002). (D-E) Prognostic value of t(4;14) and del(17p) in multiple myeloma.
![]()
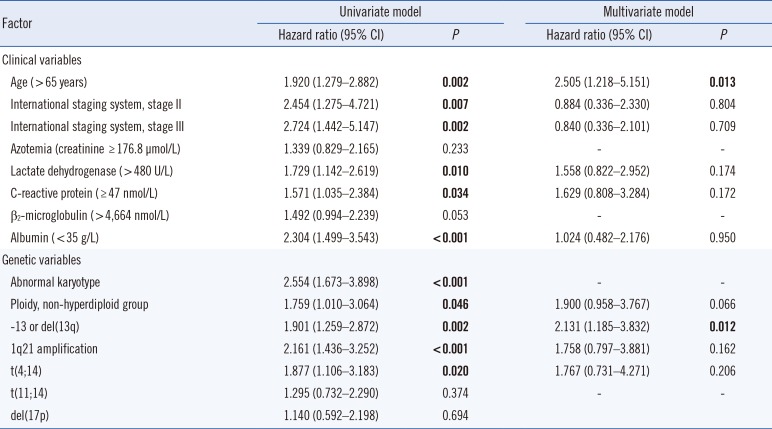
Table 4
Univariate and multivariate Cox regression analyses of the potential factors for overall survival (OS)
![]()
5. Role of additional chromosomal changes in the prognostic value of t(4;14) and del(17p) in MM
Table 5
Role of additional chromosomal changes in the prognostic value of t(4;14) and del(17p) in multiple myeloma
![]()
 XML Download
XML Download