

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor,
Chronic myeloid leukemia (CML) is a clonal hematopoietic stem cell disorder characterized by a reciprocal translocation between the long arms of chromosomes 9 and 22, resulting in the formation of a Philadelphia (Ph) chromosome. Most chimeric BCR-ABL1 fusion transcripts are e13a2(b2a2) or e14a2(b3a2), encoding a 210-kDa protein, p210, but some are a e1a2 transcript or e19a2 transcript encoding a 190-kDa protein or a 230-kDa protein, respectively [1]. Furthermore, some patients harbor rarer atypical transcript types such as e1a3, e6a2, e8a2, and e13a3. In addition, BCR-ABL1 transcripts have been reported to correlate significantly with the prognosis of CML patients. We retrospectively studied a CML patient with a variant BCR-ABL1 fusion transcript with no insertion between BCRexon8 and ABLexon2, to elucidate clinical characteristics of the rare e8a2 transcript CML.
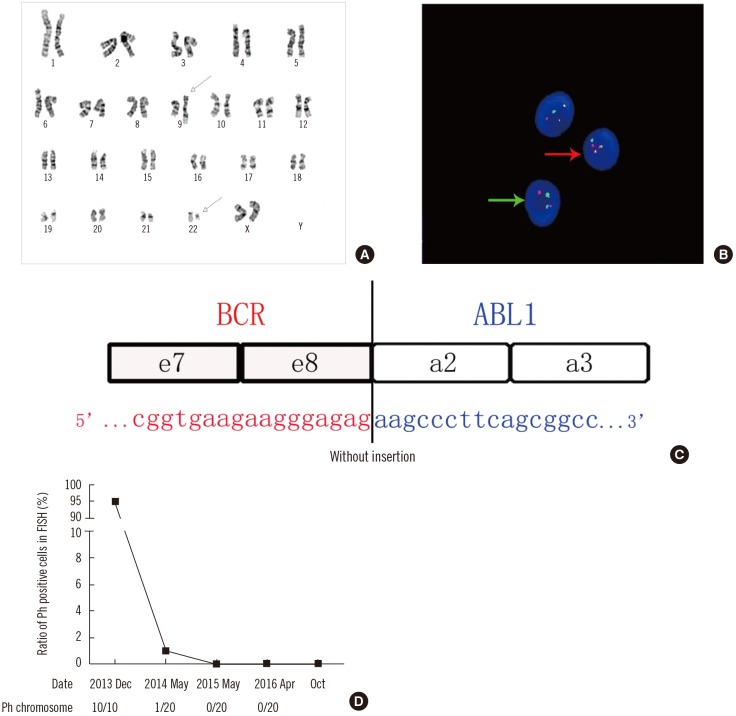
The study was approved by the Human Research Ethics Committee of Wuhan Tongji hospital, Wuhan, China. Written informed consent was obtained from the patient. A 47-year-old woman-was referred to Tongji Hospital in December 2013. Peripheral blood analysis revealed a white blood cell count of 124×109/L (82.7% neutrophils, 7.2% lymphocytes, 5.9% monocytes, 3.0% eosinophils, and 1.2% basophils); platelet count of 613×109/L; and hemoglobin level of 10.8 g/dL. The patient showed typical characteristics indicative of splenomegaly. The bone marrow smear indicated an abnormal cell composition including 4% myeloblasts. G-banding karyotype analysis showed 46, XX, t (9;22)(q34;q11) in all 10 analyzed metaphase cells (Fig. 1A).FISH analysis revealed Ph-positive cells with one green BCR signal, one red ABL signal, and two yellow BCR-ABL fusion signals, which were present in 95% of 200 interphase cells counted (Fig. 1B). Nevertheless, we failed to detect typical BCR-ABL1 transcripts such as e13a2 or e14a2 by qualitative RT-PCR. Subsequently, Sanger sequencing of complementary DNA revealed the e8a2-type fusion transcript (Fig. 1C). Accordingly, the patient was diagnosed as having CML in the chronic phase.Therefore, imported imatinib (400 mg, po, qd) was administered. After two weeks, the imported imatinib was replaced by domestic imatinib (400 mg, po, qd) because of the high cost of the former. At the request of the patient, the cytogenetic response was measured irregularly using FISH rather than by performing molecular monitoring using real-time quantitative PCR (RTqPCR). Positive cells were undetectable after 17 months of treatment (Fig. 1D).
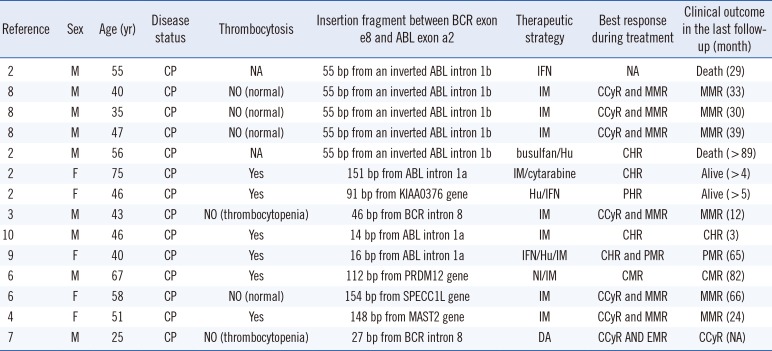
It is widely acknowledged that the direct junction between BCR exon e8 and ABL exon e2 fails to encode the chimeric oncogenic protein owing to the presence of a premature stop codon (UAG) at position 7 after the fusion locus [23]. Nevertheless, insertion of certain sequences could lead to the generation of an in-frame e8a2BCR-ABL1 transcript. In the 14 cases reported previously, insertion sequences from ABL intron 1b were identified in five cases; those from ABL intron 1a in three cases; those from BCR intron 8 in two cases; and those from another definite gene such as PRDM12, SPECC1L, or MAST2, in four cases [456]. Interestingly, in our case, sequencing analysis revealed that the BCR-ABL1 transcript was derived from a direct combination of BCR exon e8 to ABL exon e2, without any insertion between them. Moreover, this junction subtype of could indeed encode the oncogenic protein resulting in occurrence of CML. Furthermore, the number of bases in this insertion sequence contained three multiples of triplet bases [7]. Perhaps in simply considering the advent of the stop codon after the fusion contributing to the halt of normal translation of the BCR-ABL1 transcript, the previous reports misinterpreted the accurate coding sequence in the open reading frame of the fusion transcript.
According to the analysis of all cases, thrombocytosis could not predict the prognosis of patients. The insertion segment derived from particular functional genes including PRDM12, SPECC1L, or MAST2 demonstrated no association with poor molecular response. Additionally, tyrosine kinase inhibitors (TKIs) could effectively treat CML patients with the e8a2 transcript (Table 1). Just as in our case, the patient achieved complete cytogenetic response. Moreover, in an unique reported case where imatinib treatment was withdrawn after four years of constant complete molecular remission, the e8a2 transcript became detectable after three months and reverted to an undetectable status again four months after resumption of imatinib treatment.
It is recommended that RT-qPCR be utilized to monitor the molecular level precisely. TKIs have been demonstrated to be effective in the treatment of e8a2-positive patients. However, a larger number of CML patients with the e8a2 transcript are needed to study the clinical features and prognosis.
 XML Download
XML Download