

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Listeriosis caused by Listeria monocytogenes is a bacterial infection with a high case-fatality rate (CFR) of approximately 20% to 30%; listeriosis occurs mainly in the elderly, neonates, immunocompromised patients, and pregnant women via central nervous system (CNS) infection and bloodstream infection (BSI) [1234]. This gram-positive intracellular bacterium is widespread in the natural environment [5], and infections mostly arise following the consumption of contaminated food, such as unheated ready-to-eat meals and dairy products [678], because of the ability of L. monocytogenes to survive under salty or acidic conditions and grow at refrigeration temperatures [9].
An increase in the annual incidence of listeriosis has been reported in many countries recently [17101112]. Although a number of listeriosis outbreaks have been reported [13], most cases are sporadic. In addition, there is an increasing concern regarding the emergence of healthcare-associated listeriosis [11]. However, L. monocytogenes infection is difficult to diagnose and treat with appropriate initial empiric treatments because it does not produce any specific symptoms [14].
Large-scale multilocus sequence typing (MLST) has been performed in a number of European countries to investigate the genotype-related characteristics of strains [14615]. However, only a few groups have performed MLST studies of L. monocytogenes in Asian countries [16], and the available data is too limited for comparisons with other regions.
We investigated the annual incidence, clinical characteristics, and outcomes of listeriosis at three different hospitals in Korea and evaluated the effects of appropriate empiric antimicrobial treatments on patient outcomes. In addition, we analyzed MLST profiles of a subset of L. monocytogenes isolates to determine which strains caused outbreaks and compared our data with the results of previous studies. We aimed to determine whether listeriosis incidence increased in Korea and to analyze the risk factors associated with treatment outcome.
METHODS
We retrospectively collected the data pertaining to all culture-positive cases of human listeriosis from three hospitals of different sizes (38 cases from hospital “A” [>2,000 beds; tertiary university hospital, Seoul], 10 cases from hospital “B” [>800 beds; tertiary university hospital, Seoul], and 10 cases from hospital “C” [>700 beds; secondary national hospital, Goyang]) in Korea during 2006–2016 and calculated the annual number of cases and incidence per 100,000 admissions at the three hospitals. We excluded duplicate cases.
The following clinical data were collected from electronic medical records: age at diagnosis, sex, underlying diseases, date of patient death or most recent visit, sampling sites, date of sample collection and report of culture results, and any antimicrobial agents administered during hospitalization. Available laboratory findings at the time of sample collection, including C-reactive protein (CRP) level, erythrocyte sedimentation rate (ESR), white blood cell (WBC) count, neutrophil percent, and antimicrobial susceptibility test results, were also obtained.
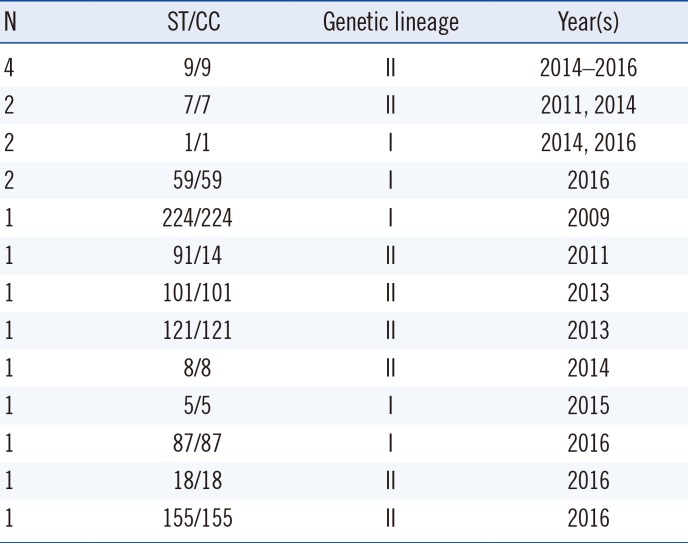
We performed MLST analysis for 19 isolates collected from hospital “A”, as described by Ragon et al [6]. The sequences of seven housekeeping genes (abcZ, bglA, cat, dapE, dat, ldh, and lhkA) were analyzed, and the sequence type (ST) and clonal complex (CC) of the obtained data were assigned using the Listeria MLST database hosted by the Institut Pasteur (http://bigsdb.pasteur.fr/listeria).
This retrospective study was approved by the Institutional Review Board at Shinchon and Gangnam Severance Hospital (Seoul, Korea) and the National Health Insurance Service of Ilsan Hospital (Goyang, Korea).
1. Definitions
Cases were categorized as CNS infections, BSIs, pregnancy-associated infections, or other infections based on the site of isolation of L. monocytogenes and clinical diagnosis. Pregnancy-associated infections were defined as listeriosis in <30-day-old newborn infants with maternal-fetal infections.
The presence of the following immunocompromised conditions was documented: solid organ cancer, hematologic malignancy, type 2 diabetes mellitus (DM), chronic kidney disease, chronic respiratory disease, chronic liver disease, stroke, and autoimmune disease treated with corticosteroids.
The term CFR refers to non-pregnancy associated mortality within 30 days of the sample collection date.
Listeriosis was considered to be ‘healthcare-associated’ if (a) the onset of listeriosis symptoms occurred 48 hours post admission and there was no evidence of infection at admission; if (b) infections were acquired at other hospitals prior to transfer to the study hospitals; or if (c) infections were acquired during a previous admission within two weeks of presentation. Otherwise, listeriosis was considered to be community-associated, as previously reported [1718].
Antimicrobial agents were categorized into three groups: first-line antimicrobial agents, defined as monotherapy or combinations of penicillin or ampicillin and gentamicin; alternative antimicrobial agents including trimethoprim-sulfamethoxazole, erythromycin (excluding ineffective use for pregnancy-associated infections) [19], vancomycin (excluding ineffective use for CNS infections) [20], imipenem, or meropenem; and other drugs classified as inadequate antimicrobial agents [10].
2. Statistical analysis
Incidence rates ratios (RRs) and 95% confidence intervals (CI) were calculated by comparing the mean incidence between 2006–2013 and 2014–2016.
In all variables included in the statistical analysis, we assessed whether they followed a Gaussian distribution using the Shapiro-Wilks test. We described the case characteristics using medians and interquartile ranges (IQRs). The significance of the differences between groups was tested with Fisher's exact test for qualitative data and the Mann-Whitney U test for quantitative data.
To obtain odds ratios (ORs), univariate and multivariate regressions were performed using logistic regression. Dependent variables included in the multivariate regressions were selected using Akaike's information criterion (AIC) based on forward stepwise logistic regression. The presence of variance inflation factors was also examined for all parameters of the multiple regression models.
All reported P values are two-tailed, and P values <0.05 were considered to indicate statistical significance. All statistical analyses were performed using the R statistical software (Version 0.99.893— 2009–2016; R Studio, Boston, MA, USA).
RESULTS
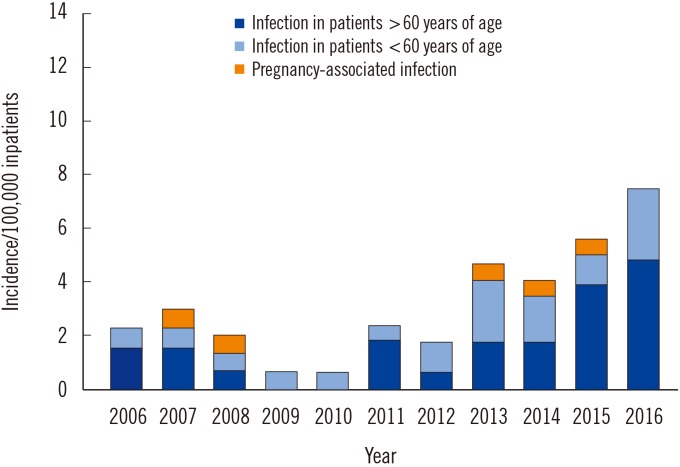
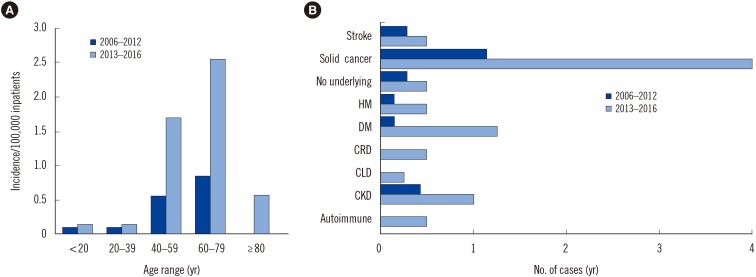
Although the annual incidence of listeriosis was stable from 2006–2012, it has increased since 2013 (Fig. 1). The incidence of listeriosis was significantly higher in 2013–2016 than in 2006–2012 (RR 3.1; 95% CI 1.79–5.36; P<0.001), mainly because of the increase in patients >60 years of age (RR 3.69; 95% CI 1.70–8.02; P<0.001) and those with underlying diseases such as solid organ cancer and DM (Fig. 2).
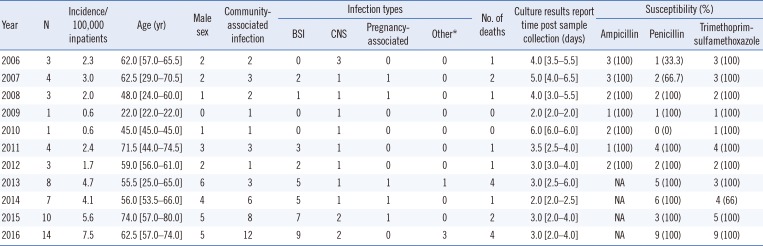
Table 1 describes the clinical characteristics of cases by year. No statistically significant differences were observed in patient sex, infection type, isolate source, or CFR. Fig. 2 illustrates the increased annual incidence of three groups: pregnancy-associated infections, patients >60 years of age, and patients <60 years of age. There was no significant difference in pregnancy-associated infections; however, the incidence of patients >60 years of age increased.
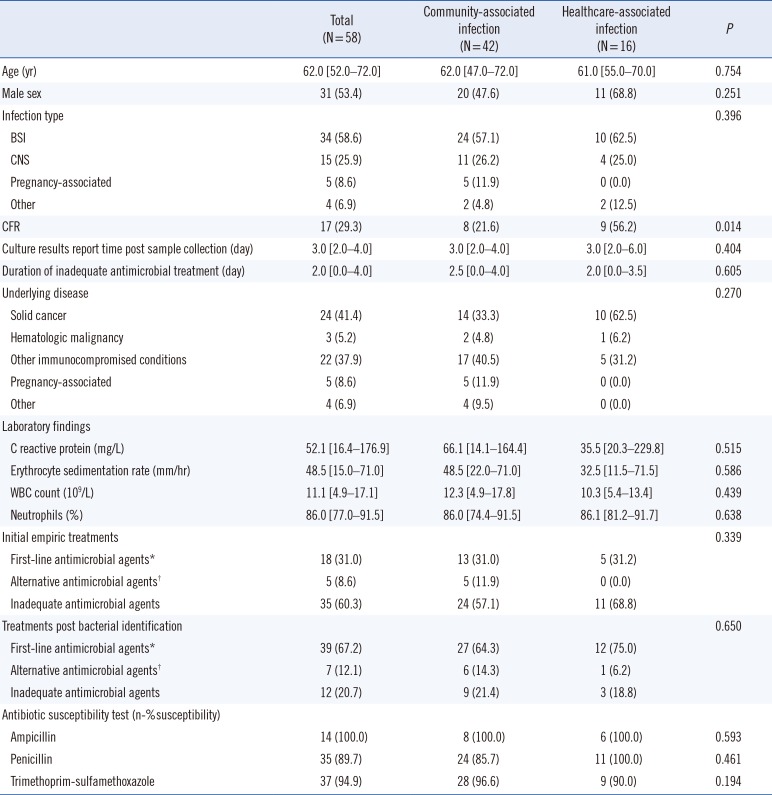
The median age of all 58 patients was 62 years (IQR, 52–72 years). Thirty-one (53.4%) patients were males. Patient demographic and baseline characteristics according to community- and healthcare-associated infections are summarized in Table 2. Forty-two cases were classified as community-associated infection, and 16 cases were classified as healthcare-associated infection. Of the infections, 58.6% were BSIs, 25.9% were CNS infections, 8.6% were pregnancy-associated infections, and 6.9% consisted of other infections such as peritonitis (three of four cases) and pneumonia (one of four cases). Inadequate antimicrobial agents were most frequently observed in initial empiric treatment (60.3%), and first-line antimicrobial agents were selected in 31% (18 of 58) of cases; treatment regimen was mostly altered to first-line antimicrobial agents after obtaining culture results (median delay of 0 day; IQR, 0–2 days). All 14 isolates tested for antimicrobial susceptibility were susceptible to ampicillin, whereas only two of the 39 isolates showed resistance to trimethoprim-sulfamethoxazole and four of the 39 isolates were resistant to penicillin. There were no statistically significant differences between the community- and healthcare-associated infection groups in terms of median age at diagnosis, sex, or infection type. Of the non-pregnancy associated cases, 17 patients died within 30 days of sample collection. The healthcare-associated infection group showed a higher mortality rate than the community-associated infection group (56.2% vs 21.6%, P=0.014).
MLST analysis of 19 available L. monocytogenes isolates from hospital “A” revealed that seven isolates belonged to genetic lineage I and 12 isolates belonged to genetic lineage II and that there were 13 different sequence types (ST) present (Table 3). The remaining 39 isolates had not been frozen and therefore could not be analyzed. The most commonly identified genotype was ST9 (four isolates), followed by ST7, ST1, and ST2 (two isolates each). No dominant sequence type was apparent.
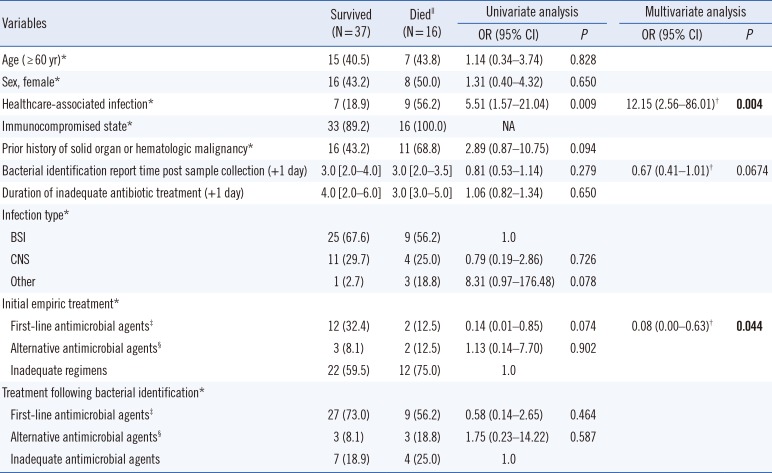
Variables associated with CFR are described in Table 4. Univariate analysis showed that healthcare-associated infection was associated with CFR (OR, 5.51; 95% CI, 1.57–21.04; P=0.0093). Multivariate analysis showed that healthcare-associated infection (adjusted OR, 12.15; 95% CI, 2.56–86.01; P=0.004) and empirical treatment with first-line antimicrobial agents (adjusted OR, 0.08; 95% CI, 0.00–0.63; P=0.044) were associated with CFR.
DISCUSSION
Human listeriosis is a rare disease; however, its incidence has increased in recent years in many countries [11521]. Our data also demonstrated a significant increase of listeriosis at three Korean hospitals since 2013. It was mainly due to an increase in patients over the age of 60 years and patients in an immunocompromised state due to conditions such as solid organ cancer or type 2 DM.
Listeriosis exhibited a high CFR (29.3%) in our study. Using multivariate analysis, we found that healthcare-associated infections constitute a risk factor related to higher CFR compared with community-associated infections. In addition, the initial selection of appropriate empiric antimicrobial agents was associated with a low CFR. Therefore, initial empiric treatment should be chosen carefully in patients with healthcare-associated listeriosis.
However, it is difficult to select an adequate initial regimen because listeriosis does not present with any specific symptoms, and many classes of antimicrobial agents that are widely used in clinical settings, such as cephalosporins [15] and quinolones [22], are not effective against L. monocytogenes infection. In our study, only 18 of 58 (31.0%) patients were treated initially with ampicillin- or penicillin-based regimens, whereas 35 patients (60.3%) were treated with inadequate empirical regimens, including cephalosporins (18 patients, 27.6%), quinolones (nine patients, 15.5%) and no empirical antibiotics (eight patients, 13.8%). Although 24 of 35 patients who received inadequate initial empirical regimens were immediately changed over to adequate drugs (median, 2.0 day), such as ampicillin or penicillin once culture results were obtained, this was not reflected by a statistically significant difference in CFR.
A previous meta-analysis has suggested that L. monocytogenes should not be considered in febrile infants because of the very rare incidence of listeriosis at that age [23]. In addition, the annual incidence of pregnancy-associated listeriosis has decreased significantly since 1985, presumably because of preventive campaigns aimed at pregnant women [242526]. However, an increased incidence of listeria in adults over 60 years of age has been reported in several studies [11527]. Therefore, the initial empiric treatment against L. monocytogenes, especially in healthcare-associated infections, should be carefully considered in groups at high-risk for listeriosis such as elderly and immunocompromised patients.
Because no major STs were found in the MLST analysis, the increased incidence we observed was likely due to sporadic cases rather than an outbreak. We compared the STs of L. monocytogenes obtained by MLST with those reported in previous studies in other countries [2829]. CC8 was a major global L. monocytogenes isolate because of its high biofilm forming capacity and its ability to persist in food industrial processes and subsequently contaminate food [30]. According to our results, only one of the 19 isolates was identified as CC8, while the most common ST (four of 19 isolates) was CC9, consistent with the frequency described by Cantinelli et al [28]. The fact that CC8 was not the major ST in our study may be due to differences in regional or dietary habits in Korea.
Our study had a number of limitations. It was a retrospective study, and only 19 of 58 isolates were subjected to MLST analysis, which could have biased the results and decreased the likelihood of identifying major type isolates. In addition, several important medical record details, such as infection source of listeriosis, were not available for most patients. However, although human listeriosis is a food-borne disease, it is difficult to determine the food source of infection because of the long incubation time of L. monocytogenes [7].
This study demonstrated an increased incidence of listeriosis in elderly patients and those in an immunocompromised state at three Korean hospitals. Healthcare-associated infections caused by L. monocytogenes were associated with a high CFR and adequate initial empirical treatments appeared to reduce CFR, suggesting that careful consideration of the empirical antimicrobial regimen for elderly or immunocompromised patients admitted to the hospital is warranted. Multi-center, prospective studies including a larger number of patients with listeriosis would help support our recommendations concerning careful initial empiric treatment of healthcare-associated infections.
 XML Download
XML Download