

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tuberculosis (TB) is a major global health concern. In 2014, there were 9.6 million new cases of active TB worldwide and 12% of these cases involved coinfection with HIV and 1.5 million deaths, including 400,000 deaths among patients infected with HIV [1]. About 480,000 incident cases of multidrug-resistant TB were estimated to be caused by Mycobacterium tuberculosis organisms resistant to at least isoniazid and rifampin in 2014 [1].
The standard treatment for TB comprises an intensive phase with isoniazid and rifampicin, as well as pyrazinamide and ethambutol for two months, followed by a continuation phase that comprises the concomitant use of isoniazid and rifampicin for further four months [234]. Although the standard 6-month treatment regimen is highly effective for drug-susceptible TB, the use of multiple drugs over long periods of time can cause frequent adverse drug reactions [56]. These adverse reactions could result in interruption or discontinuation of anti-TB treatment, with subsequent risks of treatment failure and drug resistance [7]. The most common and important adverse reaction is hepatotoxicity because this is associated with the three most important first-line drugs: isoniazid, rifampin, and pyrazinamide [56]. Hepatotoxicity is most frequently dose-related; however, some cases are caused by drug hypersensitivity [8].
In addition, some patients with drug-susceptible TB do not respond adequately to treatment and develop treatment failure and drug resistance [910]. The current recommended doses of anti-TB drugs are based on the patient's body weight [1112]. Because drug concentrations and pharmacokinetics vary markedly among patients, this approach can cause adverse drug reactions because of toxic drug levels as well as the development of antibiotic resistance and treatment failure due to suboptimal drug levels [131415]. Therapeutic drug monitoring (TDM), which is individualized drug dosing guided by serum drug concentrations, could reduce the incidence of adverse drug reactions and increase the likelihood of successful treatment outcomes [161718].
Numerous factors affect the pharmacokinetics (PK) of drugs [19]. Pharmacogenetics is the study of interindividual variations in DNA sequence that are related to a drug response [20]. In recent years, several studies have demonstrated that some genetic polymorphisms are associated with susceptibility to adverse drug reactions such as hepatotoxicity [212223]. Furthermore, the nutritional state affects drug exposure and treatment outcomes in TB patients [242526]. Deficiency of some nutrients such as vitamin D is associated with an increased risk of TB and poor treatment outcomes [272829].
The anti-TB drugs currently in use were developed over 40 yr ago [30]. Although several promising novel agents have been developed for the treatment of multidrug-resistant TB in recent years [3031], these new drugs will not be readily available for the treatment of drug-susceptible TB in the future. Therefore, optimizing current treatment regimens is important to improve the effectiveness of treatment of TB. This article reviews the current knowledge on the clinical usefulness of TDM, pharmacogenetics, and the assessment of nutritional state in the management of patients with TB to improve anti-TB treatment response.
TDM OF ANTI-TB AGENTS
1. Basic principles of TDM for TB patients
TDM is currently widely used to optimize the efficacy and safety of many commonly used drugs [32]. To maximize patient exposure to these drugs while avoiding or limiting toxicity, several studies on anti-TB drug PK, pharmacodynamics (PD), and TDM have been reported [1633]. Patients infected with HIV and those with type 2 diabetes have been reported to be confronted with a risk of poor drug absorption and drug–drug interactions [1632]. In cases with inadequate exposure to anti-TB drugs and a possible suboptimal treatment response, treatment failure risk and toxicity increase [16]. The inefficacy of the drugs might be due to faulty administration, poor storage conditions and product quality, counterfeit product, or interactions [34]. Published guidelines typically describe interactions between two drugs, whereas the situation is more complex clinically and TDM is often the best available tool for resolving multidrug interactions and providing patients adequate and safe drug doses [1635]. TDM can assist in clinical decision-making [36].
The indications for TDM are prioritized to patients who fail to show sputum culture conversion within two months of standardized treatment, those with adverse drug reactions, and/or multiple risk factors such as HIV infections, type 2 diabetes, gastrointestinal tract problems causing malabsorption, or those who are severely ill [1832]. For these patients, TDM can be helpful in shortening the time to achieve treatment response and completion [163237].
A recent review of the evidence for measuring drug concentrations of first-line anti-TB drugs in adults stated that the routine measurement of drug concentrations in the general TB population is not warranted because most previous studies were limited by small sample sizes and yielded insufficient evidence [32]. Well-designed prospective randomized controlled studies are needed to determine the role of measurement of drug concentrations during anti-TB therapy [1638].
2. Practical aspects of TDM for anti-TB agents
To measure serum or plasma anti-TB drug concentrations, chromatography-based methods such as HPLC-ultraviolet detection, HPLC-fluorescence detection, and HPLC–tandem mass spectrometry (MS/MS) have been introduced [42]. LC-MS/MS is particularly useful as a simple and rapid analytical method for simultaneous, quantitative determination of 20 anti-TB drugs including both first-line and second-line anti-TB drugs [42].
Blood samples for TDM should be collected in plain red-top tubes [36]. Heparin-containing green-top tubes can also be used (except in the case of injectable drugs), and the tubes should be placed on ice when the blood collection site is far from a laboratory [16]. Promptly centrifuged serum samples should be harvested and frozen after the blood draws to mitigate concerns about the stability of anti-TB drugs at room temperature, particularly isoniazid and ethionamide [1636]. A recent report regarding the use of TDM indicated that dried blood spots with a lower blood volume can be used as an alternative to conventional serum sampling methods for some anti-TB drugs, and would reduce costs, especially in areas with limited resources such as low-income countries or in pediatric populations [4041]. Further studies are needed to validate the clinical and analytical efficacy of this method including refining drug-specific protocols for analytical validation and quality control [41].
3. Recent guidelines for TDM in TB patients
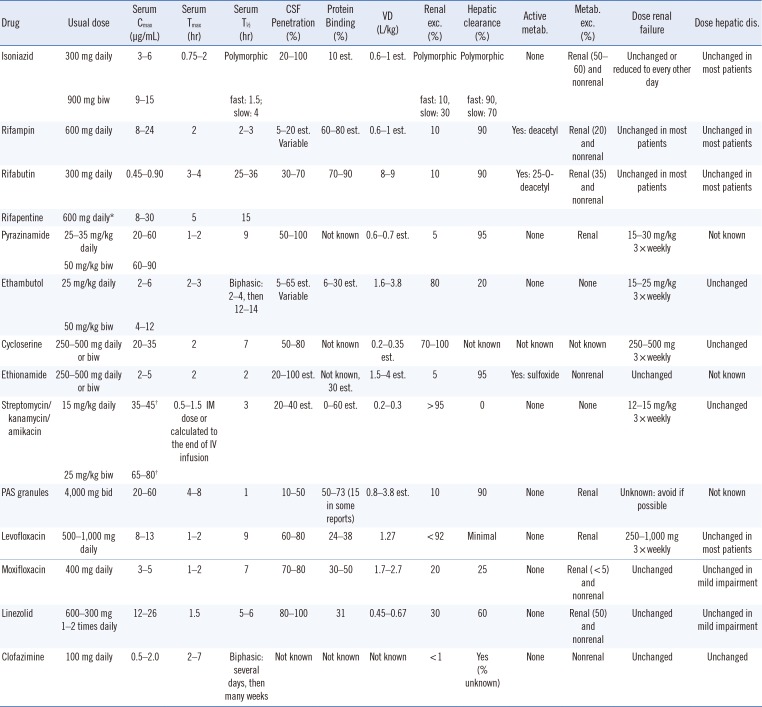
The guidelines for TDM in TB treatment introduced in 2002 were updated recently [1633]. The peak concentrations (Cmax) may have more significance for several anti-TB drugs than the trough concentrations, and the trough concentrations of numerous anti-TB drugs are usually too low (below the limit of detection of the measurement assays) [16]. Therefore, 2-hr post-dose samples to estimate the peak concentrations can be collected, with the exception of certain drugs such as rifabutin, for which 3-hr samples are more appropriate (Table 1) [16]. Considering the variability of oral drug absorption and the fact that single time points may miss the correct time that reflects the actual peak, typically 6-hr post-dose (7 hr for rifabutin) second samples provide more information about drug absorption status [16].
Dose adjustment should be based on both drug exposure and the minimal inhibitory concentration (MIC) of the M. tuberculosis strain to attain the optimal PK/PD profile [18]. Although the area under the concentration-time curve (AUC) to MIC (AUC/MIC) is the most important PD parameter for most anti-TB drugs, estimating the AUC requires several blood samples (minimum of six or seven samples) and, therefore, is impractical [36]. Moreover, limited sampling strategies to determine the sampling time that is most informative for the AUC have been introduced for several drugs [39].
Another approach for estimating PK parameters and achieving a specific therapeutic target is to use a maximum a posteriori estimation Bayesian approach; however, this is rather time-consuming and requires a sophisticated software [16]. Because not every dose increase results in increased drug exposure, follow-up at 1–2 weeks after dose adjustment to ensure that the target drug concentrations are reached is required [18].
PHARMACOGENETICS OF ANTI-TB AGENTS
1. Genetic polymorphisms of drug-metabolizing enzymes associated with anti-TB agents
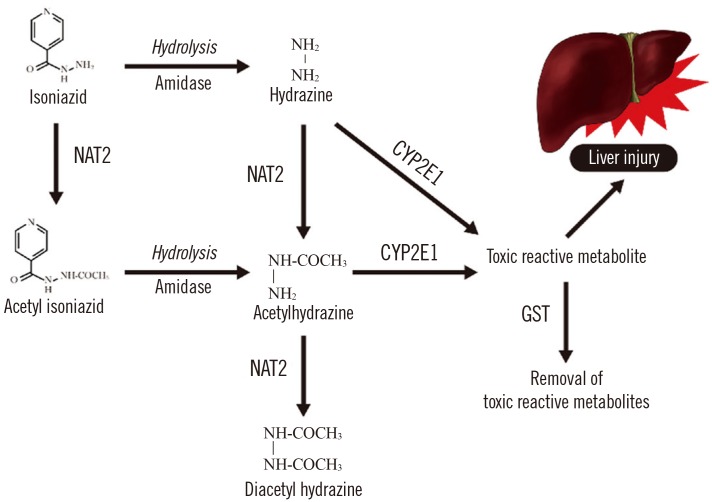
Pharmacogenetics-based testing involves genetic testing to assess the risk of an adverse response in a patient or the likelihood of a patient responding to a given drug, which facilitates drug selection and dosing [4041]. Polymorphisms of N-acetyl transferase 2 (NAT2), cytochrome P450 2E1 (CYP2E1), and glutathione S-transferase (GST1) have been reported to increase patients' susceptibility to isoniazid-induced hepatotoxicity (Fig. 1) [38]. The NAT2 rapid acetylators and CYP2E1 rapid metabolizers show increased concentrations of hepatotoxic metabolites, while the GST1 rapid metabolizers show decreased concentrations [38]. Some studies reported that the HLA, uridine 5′-diphosphate (UDP)-glucuronosyltransferase (8UGT), nitric oxide synthase (NOS), broad complex, tramtrack, bric-a-brac (BTB) and cap ‘n’collar type of basic region leucine zipper factor family (CNC) homolog (BACH), and Maf basic leucine zipper protein (MAFK) polymorphisms have roles in isoniazid-induced hepatotoxicity by modifying antioxidant enzymes expression [38].
2. Practical aspects of genotyping for therapy with anti-TB agents
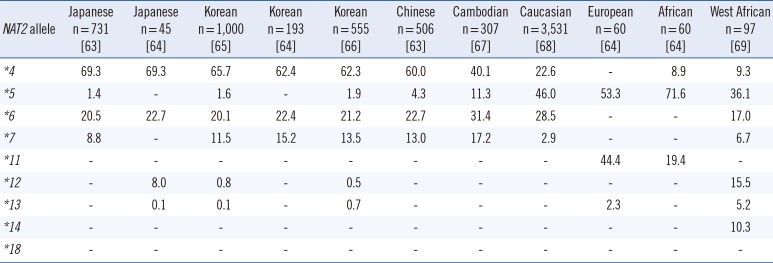
The NAT2 genotype is a biomarker listed on the rifampin, isoniazid, and pyrazinamide (Rifator) drug label in the Food and Drug Administration Table of Pharmacogenomic Biomarkers in Drug Labels [45]. The label contains information relating to the metabolism of isoniazid by acetylation and dehydrazination. In addition, it states that rifampin and isoniazid can induce or inhibit particular CYP450 enzymes and, therefore, could affect the metabolism of concomitantly administered drugs that are metabolized by these enzymes [45]. NAT2 genotype and assigned phenotype are summarized in Tables 2, 3, and 4.
The following single nucleotide polymorphisms (SNPs) at seven different sites of the NAT2 gene are considered to have a serious phenotypic effect on N-acetylation activity: rs1801279 (c.191G>A), rs1041983 (c.282C>T), rs1801280 (c.341T>C), rs1799929 (c.481C>T), rs1799930 (c.590G>A), rs1208 (c.803A>G), and rs1799931 (c.857G>A) [42].
Pharmacogenetic analysis for genotyping of drug-metabolizing enzyme polymorphisms can be performed by using various methods such as sequencing, polymerase chain reaction, restriction fragment length polymorphism, and high-throughput microarray (such as SNPstream) [42]. DNA sequencing is still considered the gold standard for NAT2 genotyping [42].
3. Genotype-based dosing guidelines for anti-TB drugs
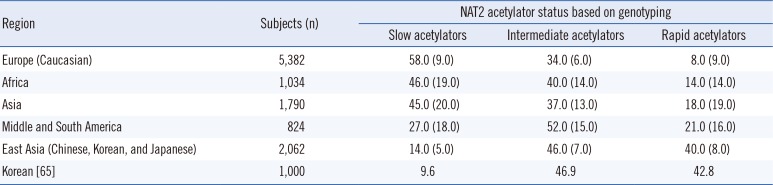
International dosing guidelines consider the patient genotype by the Clinical Pharmacogenetics Implementation Consortium (CPIC) [43]. However, the Royal Dutch Association for the Advancement of Pharmacy - Pharmacogenetics Working Group (DPWG), and other professional societies do not provide genotype-based dosing guidelines for anti-TB drugs [44]. Furthermore, evidence suggests that the acetylation status of an individual based on genetic variants in the NAT2 gene markedly contributes to the mechanism of drug-induced hepatotoxicity and/or drug efficacy [384145]. Slow acetylators of isoniazid may be more susceptible to drug-induced hepatotoxicity because of higher blood concentrations of the drug than rapid acetylators are, and the high frequency of slow and intermediate acetylators in the Asian population suggests that these populations are more susceptible to isoniazid-induced hepatotoxicity [384145].
Several pharmacogenetic anti-TB therapies have been proposed, in which the daily dose of isoniazid is optimized according to the NAT2 genotype [414647]. A recent randomized controlled trial of pharmacogenetics-based therapy revealed that an NAT2 genotype-guided regimen in Japanese TB patients reduced isoniazid-induced liver injury and early treatment failure during the 6-month four-drug standard treatment of TB [44]. This observation suggests the potential usefulness of NAT2 genotype-guided dose stratification of isoniazid in chemotherapy for TB [46]. In that study, NAT2 genotype-guided isoniazid dosing stratification comprised 7.5, 5, and 2.5 mg/kg for rapid, intermediate, and slow acetylators compared with the conventional standard treatment of 5 mg/kg isoniazid [46]. In Korea, a prospective study of NAT2 genotype-guided isoniazid dosage regimen for patients with TB also ensured they achieved therapeutic concentrations of isoniazid [47]. In that study, the equation obtained using regression analysis determined that the best-predicted isoniazid concentration was as follows: isoniazid concentration (mg/L)=13.821-0.1×(body weight, kg)-2.273×(number of high-activity alleles of NAT2 genotype; 0, 1, and 2) [47]. The model revealed that the frequency of being within the therapeutic range of 3.0–6.0 mg/L was higher in the model-based treatment group than it was in the standard treatment group in 53 newly enrolled patients (80.8% vs 59.3%) [47]. Well-designed prospective studies are needed to determine the role of pharmacogenetics-based dosage adjustment and measurement of drug concentrations in monitoring hepatotoxicity symptoms and optimizing pharmacotherapy [32].
ASSESSMENT OF NUTRITIONAL STATUS OF TB PATIENTS
1. Nutritional status of TB patients
Addressing comorbid conditions can improve anti-TB treatment responses and should be considered as a part of the standard of care for TB patients. TB could worsen undernutrition, which could further weaken the immunity [46]. Furthermore, undernutrition has been reported to be a risk factor for the progression of TB infection to active TB disease, and its presence at the initial diagnosis of active TB has been reported to be a predictor of increased risk of death and TB relapse [4849]. Food and nutritional care are essential for successful health promotion and TB prevention. The WHO guidelines on nutritional care and support for TB patients states that their nutritional status should be assessed at diagnosis and throughout treatment, and they should receive appropriate counseling based on their nutritional status [48].
2. Methods and practical aspects of assessing nutritional status
Nutritional requirements can be roughly divided into macronutrients such as carbohydrate, protein, and fat, and micronutrients such as essential vitamins and trace elements [50]. Nutritional assessment including anthropometric, biochemical, clinical, and dietary components is an integral part and starting point of appropriate nutritional care [48]. Age-appropriate anthropometric measures are required including height and weight such as weight-for-length or weight-for-height Z-score in children less than five years of age, body mass index (BMI)-for-age-and-sex Z-score in children and adolescents aged 5-19 yr, and BMI in adults and mid-upper arm circumference in children less than five years of age and pregnant women [4851]. A detailed nutrition and diet history, as well as an assessment of symptoms associated with weight loss, can assist in the identification of underlying diseases including non-dietary causes of malnutrition [49]. In addition, important comorbidities such as HIV, diabetes mellitus, or alcohol or drug abuse, and the availability of adequate food and household food security should be assessed [51].
Symptoms and signs of nutrition deficiency are frequently ambiguous and could be due to non-nutritional causes [50]. Therefore, biochemical assessments using laboratory tests enables the identification of deficiencies in specific nutrients [52]. Nutrients such as vitamins and trace elements are present in very minute concentrations, and techniques for the analysis of those nutrients should be sensitive enough to analyze concentrations of micrograms or even nanograms per liter; considerable care must be taken when measuring such compounds to avoid contamination [52]. Various direct and indirect assays such as measurement of enzymatic activity or nutrient metabolites are used to assess the quantity of nutrients in specimens such as blood, tissue, and urine [36]. Analytical techniques for clinical measurement of vitamin concentrations include the photometric, fluorimetric, and competitive protein binding assays, radioimmunoassay, HPLC, and LC-MS/MS. Furthermore, methods for trace element analysis include spectrophotometry, atomic absorption spectrophotometry (AAS), inductively coupled plasma optical emission (ICP-OES), and inductively coupled plasma mass spectrometry (ICP-MS) [36].
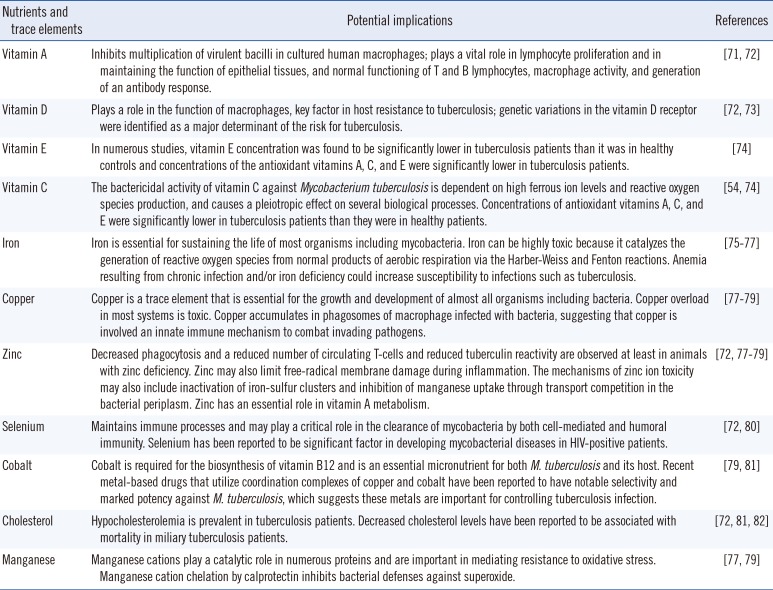
Altered circulating concentrations of vitamins A, E, and D, as well as iron, zinc, selenium, and copper have been reported in TB patients [4853]. Measurable nutrients and trace elements and their potential implications in TB infection and immunity are summarized in Table 5. A study on the status of four serum trace elements (cobalt, copper, zinc, and selenium) in Korean TB patients reported that serum cobalt and copper concentrations were higher in TB patients than in the controls [53]. Serum zinc and selenium concentrations in Korean TB patients were significantly lower and comparable to those in previous studies performed in populations of other ethnicities such as Ethiopians, Italians, and Indonesian, while reported serum copper concentrations are inconsistent [53]. In Korean TB patients, serum copper levels at diagnosis were significantly lower in rapid responders (negative sputum culture after 1 month of anti-TB treatment) than in other responders [53]. Low concentration of vitamins A, E, and D, as well as iron, zinc, and selenium usually return to normal after two months [46]. However, whether the low concentration is related to metabolic processes, the disease itself, or insufficient dietary intake, and its association with clinical outcomes for anti-TB treatment are unclear [48]. Although data are limited, and the relationship between serum concentrations and clinical outcomes of anti-TB treatment remain to be clarified, those studies suggest the potential usefulness of micronutrient status assessment in predicting therapeutic responses in TB patients and the future therapeutic approaches. A recent study revealed that M. tuberculosis is extraordinarily sensitive to destruction by vitamin C-induced Fenton reaction, which suggests the possible benefits of adding vitamin C to an anti-TB regimen and that the development of drugs that generate an oxidative burst could be useful in anti-TB treatment [54].
3. Nutritional supplementation for TB patients
Evidence of the effect of nutritional supplementation on TB prevention and health outcomes in TB patients is lacking [50]. Among the vitamins, the most extensively investigated is vitamin D [2755]. Vitamin D stimulates macrophage-mediated killing of M. tuberculosis and regulates this modality by inducing mechanisms to inactivate some aspects of the immune response and modulate others [56]. Although the function of vitamin D in immune responses in TB infection and treatment has been evaluated, no clear or consistent benefit of nutritional support in clinical improvement has been shown [56]. Only the vitamin D status and its supplementation in Korean TB patients using a variety of diagnostic methods have been assessed, but the results are inconsistent [57585960]. However, in cases of vitamin D supplementation, previous trials assessing sputum conversion could be misdirected if the major action of vitamin D in active TB disease is the mitigation of the inflammatory and immune responses [56]. This would be more appropriately evaluated by assessing tissue damage or prevention of relapse, rather than by the acceleration of sputum conversion; however, such trials are prolonged, and more difficult and costly to perform [56]. Future prospectively designed randomized controlled trials involving other vitamins and trace elements and those supplements are needed to determine whether food or energy supplementation promotes better treatment outcomes or improves the quality of life for TB patients [48].
CONCLUSIONS
Although TB is largely a curable disease, it remains a major cause of morbidity and mortality worldwide. Multiple factors are associated with the host-pathogen interaction including genetic factors of the host and the nutritional status, and may be related to the risk of TB infection. Those factors must be considered for effective TB control. Therefore, TDM during treatment and pharmacogenetics-based individualized dosing guidelines of anti-TB drugs show promise for optimizing anti-TB treatment. In addition, the assessment and management of comorbid conditions including poor nutritional status could improve the anti-TB treatment responses and, therefore, should be considered as a part of the standard of care for TB patients.

 XML Download
XML Download