

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Improved pre-transplantation evaluation and the development of post-transplantation immunosuppressive therapy have led to a marked improvement in short-term graft survival in kidney transplantation. However, long-term graft survival remains unsatisfactory [1]. Immunologic responses of patients play pivotal roles in graft rejection or recurrence of underlying renal disease. Regulatory T cells (Tregs) promote a state of antigen-specific peripheral tolerance by suppressing activation and expansion of T effector cells, as reported in experimental models [23]; therefore, they play an important role in maintaining self-tolerance and in regulating graft rejection and graft-versus-host disease [45].
Forkhead box P3 (Foxp3) is a transcription factor that regulates Treg development and function and remains the most reliable marker for Treg [6]. Therefore, Foxp3 polymorphisms, which could affect the function and quantity of the Foxp3 molecule and thus result in Treg function defects, have been associated with various autoimmune diseases [78].
For kidney transplantation, the impact of Foxp3+ Tregs on graft outcomes seems conflicting in previous reports [9101112131415]. In some study, the presence of intragraft Tregs have been associated with favorable renal allograft outcome [910]. The FoxP3+ Treg/CD3+ T cell ratio positively correlated with graft function at two years after transplantation [9]. These cells could direct a FoxP3-induced immune response toward suppression of T effector cells, promoting renal graft acceptance with improved function. Lower level of intragraft Foxp3 mRNA predicts progression in renal transplants with borderline change [11]. The mRNA levels of Foxp3 in peripheral blood were higher in patients with operational tolerance or stable kidney graft function compared with patients with chronic rejection [1213]. However, other groups reported that mRNA for Foxp3 in the urine of recipients with acute rejection (AR) was higher than recipients with normal biopsy [14] and association of higher density of FoxP3+ cells with worse graft outcome in recipients with acute cellular rejection [15].
Recently, an association between Foxp3 polymorphisms and graft outcome has been reported also with conflicting results [161718]. Therefore, we analyzed the association of four Foxp3 single nucleotide polymorphisms (SNPs) (rs3761548 A/C, rs2280883 C/T, rs5902434 del/ATT, and rs2232365 A/G) with graft outcome in kidney transplantation.
METHODS
1. Subjects
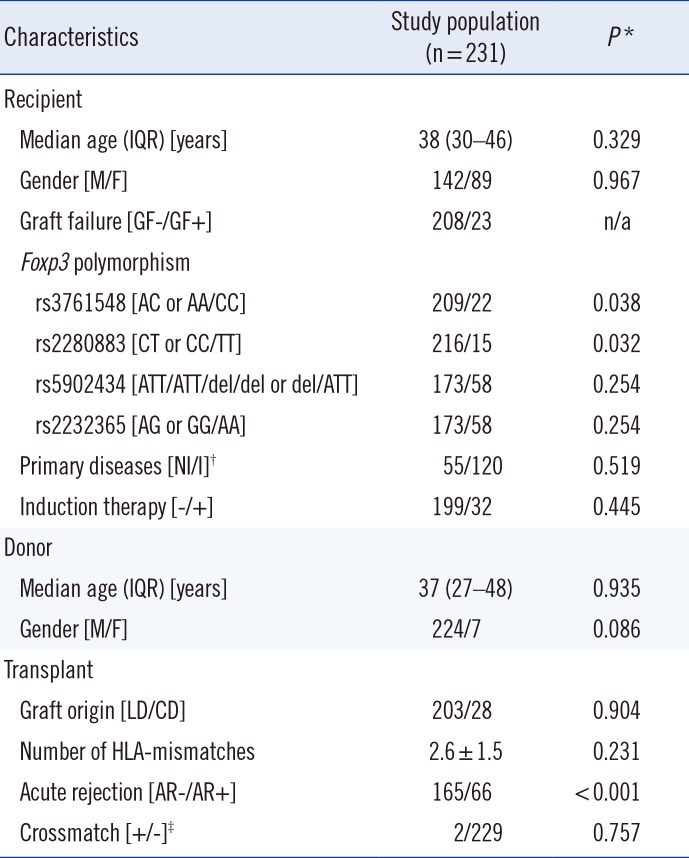
This study included 231 kidney transplantation cases performed between January 1996 and December 2004 at the Seoul National University Hospital, Seoul, Korea. The baseline characteristics of the 231 kidney transplant recipients are shown in Table 1. Residual DNA samples were collected after routine preoperative tests for HLA genotype. DNA samples from 195 healthy Korean individuals studied in our previous cohort were used as the normal controls [19]. Samples were preserved at –70℃ prior to the experiments performed for this study. The following recipient characteristics were collected retrospectively: age and gender of recipient; age and gender of donor; type of donor (living vs cadaveric donor); primary renal disease causing end-stage renal disease; number of HLA mismatches; number of HLA-DR mismatches; crossmatch result at the time of transplantation; duration of hemodialysis; type of immunosuppression; time of transplantation; occurrence and time point of biopsy-proven AR; recurrence and time point of primary renal disease; 1-, 3-, 5-, and 10-yr creatinine levels post-transplantation; and occurrence and time point of graft failure, defined as graft nephrectomy or return to hemodialysis. The study protocol was designed in accordance with the Declaration of Helsinki and approved by the institutional review board of Seoul National University Hospital (IRB No. 1306-121-501).
2. Analysis of Foxp3 Gene SNPs
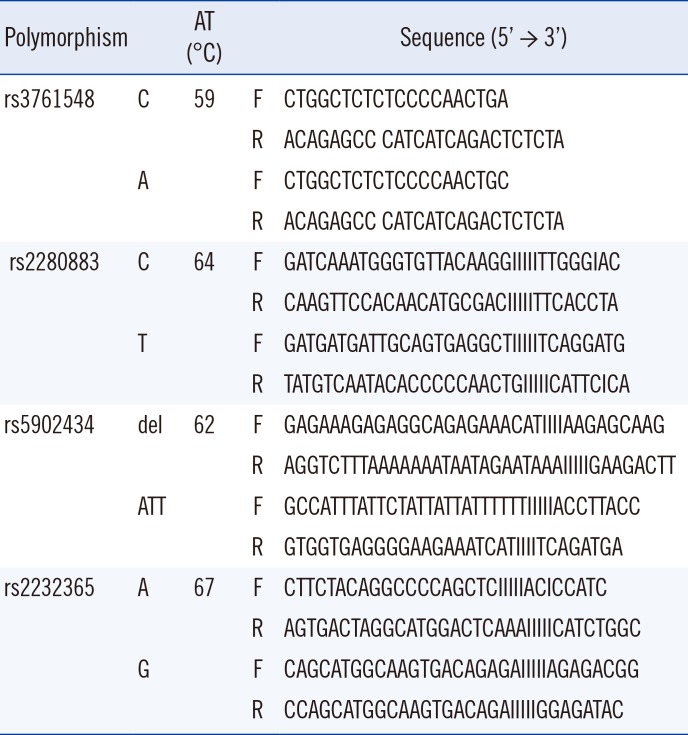
DNA was extracted from the peripheral blood of 231 patients who had kidney transplantation between January 1996 and December 2004 by using the LaboPass Genomic DNA Extraction Kit (COSMO, Seoul, Korea) or QuickGene DNA whole blood kit (Fujifilm, Tokyo, Japan) when HLA genotyping for pre-operation evaluation was performed. For 195 healthy controls, DNA was extracted using LaboPass Genomic DNA Extraction Kit (COSMO, Seoul, Korea) during the period of January 1999 and July 2001. All DNA samples were preserved at –70℃ prior to being used for Foxp3 polymorphisms analyses which were performed during the period of June 2015 and July 2016. Four Foxp3 polymorphisms (rs3761548 A/C, rs2280883 C/T, rs5902434 del/ATT, and rs2232365 A/G) were analyzed by PCR with sequence-specific primers (PCR-SSP) with some modifications [20] (Table 2). PCR was performed by using a 40-µL reaction mixture containing 40 ng DNA, 0.2mM of each primer, 0.8 µL of 10mM dNTP, 2.0mM MgCl2, 1.0 U Taq DNA polymerase (Roche Applied Science, Basel, Switzerland), and 4 µL of 10× reaction buffer. The PCR protocol consisted of an initial denaturation step at 95℃ for 5 min; 35 cycles of denaturation at 95℃ for 30 sec, annealing (temperatures detailed in Table 2) for 30 sec, and extension at 72℃ for 30 sec; and a final extension step at 72℃ for 5 min.
3. Statistical analysis
Differences of allele frequency and genotype frequency were compared by using a 2-sided Chi-square test or Fisher's exact test, as appropriate. The odds ratio (OR) was calculated by using a 95% confidence interval (CI). Potential associations of variables with graft survival were analyzed by using the Cox proportional hazards regression model. Death-censored graft survival was analyzed by using the Kaplan-Meier method and the log rank test. A P value of <0.05 was considered statistically significant. SPSS for Windows version 18.0 (SPSS, Chicago, IL, USA) was used for statistical analysis.
RESULTS
The frequencies of four Foxp3 SNPs in kidney transplant recipients were not statistically different from those of the normal controls (data not shown). Univariate Cox regression analysis indicated that the Foxp3 rs3761548 AC or AA genotype, rs2280883 CT or CC genotype, and AR episode were associated with graft survival (P=0.038, P=0.032, and P<0.001, respectively; Table 2).
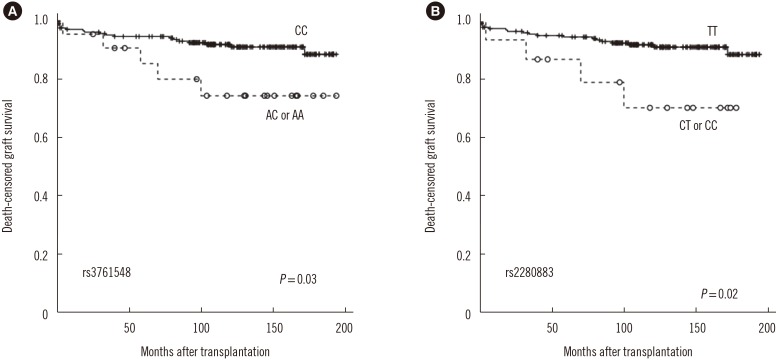
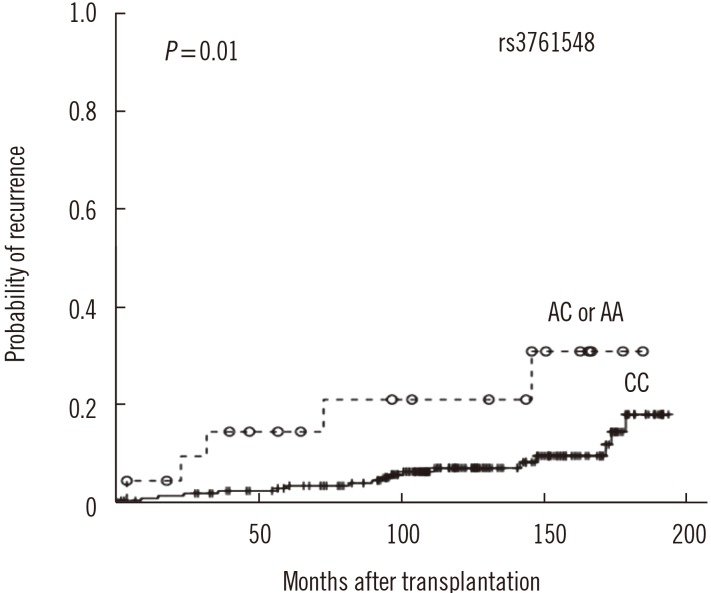
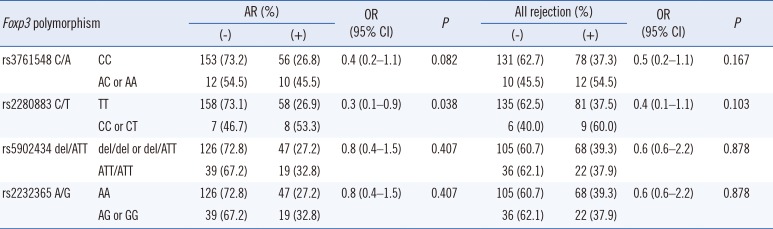
The 1-, 3-, 5-, and 10-yr creatinine levels post-transplantation did not differ according to the Foxp3 genotypes (data not shown). However, AR frequency was lower in patients with the rs2280883 TT genotype than in patients with the CT or CC genotype (26.9% vs 53.3%, P=0.035, OR=0.3, 95% CI 0.1–0.9; Table 3). Kaplan-Meier survival analysis indicated that patients with the rs3761548 CC genotype (n=209) showed better graft survival than those with the AC or AA genotype (n=22) (log rank test, P=0.03; Fig. 1A). Patients with the rs2280883 TT genotype (n=216) showed better graft survival than those with the CT or CC genotype (n=15) (P=0.02; Fig. 1B). Patients with the rs3761548 CC genotype (n=209) showed a lower rate of recurrence of the original glomerular disease than those with the AC or AA genotype (n=22) (P=0.01; Fig. 2).
DISCUSSION
In our study, both the rs3761548 AC and AA genotypes were associated with inferior graft survival and recurrence of primary renal disorders. The Foxp3 rs3761548 AA genotype has been associated with psoriasis [21], unexplained recurrent spontaneous abortion in Chinese individuals [22], and intractability of Graves' disease in Japanese individuals [23]. Recently, an association between the AA genotype and allograft rejection has been reported in kidney transplantation in Chinese individuals [16]. In addition, an association between the rs3761548 A allele and AR and between the rs3761548 AA genotype and lower graft survival have been reported in Indian individuals [18], which is similar to our findings. Polymorphisms in the promoter of the Foxp3 may alter the binding specificity of transcription factors, thus influencing transcription initiation, and therefore, might affect the function or quantity of Treg [24]. Oda et al [7] suggested that the rs3761548 AA genotype leads to a loss of binding with E47 and c-Myb, resulting in defective transcription of Foxp3. Qiu et al [16] demonstrated that patients with the AA genotype are more prone to allograft rejection in kidney transplantation and that Treg function is weaker in patients with the AA genotype than in those with the CC genotype.
The association of Foxp3 SNPs with recurrence of primary renal disorder has yet to be studied. The association of the Th1 response (high production of tumor necrosis factor-α and low production of interleukin-10) with a lower recurrence of IgA nephropathy following kidney transplantation has been reported [25]. The Treg response defect due to Foxp3 SNPs may affect the recurrence of primary glomerular disease. Further studies are needed to elucidate the association between various T cell responses and the recurrence of primary glomerular disease.
In our study, both the rs2280883 CT and CC genotypes were associated with inferior graft survival. The incidence of the Foxp3 rs2280883 CC genotype has been shown to be increased in infertile women without endometriosis in Brazil [26] and Graves's disease in China [27]; however, it was not associated with Graves' disease and juvenile idiopathic arthritis in the United Kingdom [28, 29] or with psoriasis in China [21]. To date, no study has analyzed the association of rs2280883 polymorphisms with allograft outcome following kidney transplantation, although polymorphisms of other genes relevant to host immune responses, such as FasL or IL-17, have been reported [30, 31]. Further studies involving a larger number of patients and other ethnic groups are needed to confirm the association of the rs2280883 CC genotype with renal allograft outcome.
In conclusion, our study revealed the association between the rs3761548 CC and rs2280883 TT genotypes and superior graft survival in kidney transplantation. These findings may help elucidate the role of Treg in kidney transplantation and predict renal allograft outcome.
 XML Download
XML Download