

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Peripheral blood stem cell (PBSC) transplantation following myeloablative therapy is a mainstay of treatment for various types of malignancies [12]. Stem cell-rich populations for stem cell transplantation (SCT) are generated by enforced mobilization with granulocyte-colony-stimulating factor (G-CSF), with or without chemotherapy.
Two types of stem cell collection systems are currently utilized: manually modified and automated collection systems. The most commonly used system is the COBE Spectra apheresis system (Terumo BCT, Tokyo, Japan), which requires intermittent optical/manual input from the operator, making it labor-intensive and prone to user-dependent variability [34]. The quality of the cells collected with apheresis systems such as COBE has been reported to depend on the operator and stable blood flow [56].
The Spectra Optia MNC (Terumo BCT) has two programs for mononuclear cell (MNC) collections: the MNC program and the continuous MNC (CMNC) program [7]. We used the MNC program, which has electronic features, including optical sensors for continuous automatic monitoring and stabilization of the interface and monitoring of the collection flow line, as well as a novel tubing system that is specifically designed to reduce platelet (PLT) attrition. The CMNC program has a continuous collection mode, which is similar to the MNC program of COBE Spectra [589].
Although the two systems have been compared [6], we did not find a report of such a comparison study in Korea. Therefore, the aim of this study was to evaluate the differences between the Optia MNC and COBE Spectra MNC systems according to apheresis procedures and the parameters of apheresis, products, and collection.
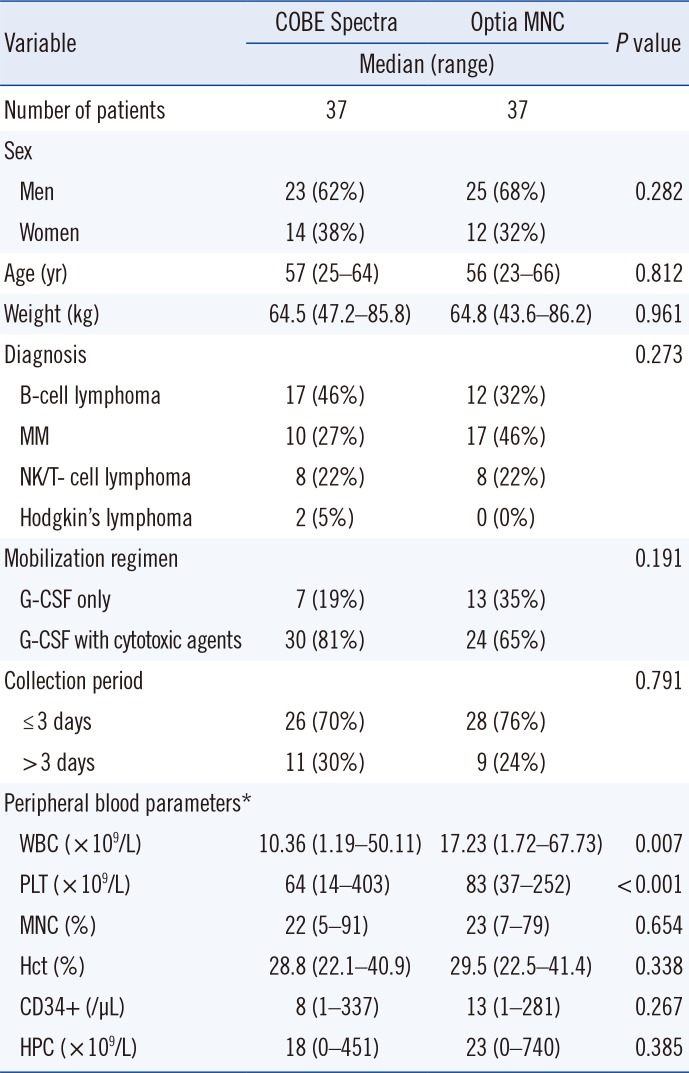
The study was approved by the Institutional Review Board in National Cancer Center, Korea (No. 2015-0272). The study included 74 patients who underwent autologous PBSC transplantation between July 2012 and July 2015, during which time both the Optia MNC and Spectra systems were used. The 74 patients comprised 48 (65%) men and 26 (35%) women with a median age of 56 yr (range, 23–66 yr). Of the 74 patients, 29 (39%) had B-cell lymphoma, 27 (36%) had multiple myeloma, 16 (22%) had natural killer (NK)/T-cell lymphoma, and 2 (3%) had Hodgkin's disease.
Stem cells were collected according to the institution's mobilization protocol, by using cytotoxic agents plus G-CSF (n=54, 73%) or G-CSF alone (n=20, 27%). Patients mobilized with cytotoxic agents plus G-CSF were injected once daily with 10 µg G-CSF/kg body weight, and PBSCs were collected on the day that the hematopoietic progenitor cell (HPC) count was ≥5/µL or the white blood cell (WBC) count was >3,000/µL [101112]. Patients mobilized with G-CSF alone were injected once daily for four days with the same dose of G-CSF prior to the apheresis procedure. WBC, PLT, MNC, and HPC counts, and Hct levels in the peripheral blood and PBSC products were determined by using an XE-2100 hematology analyzer (Sysmex Corporation, Kobe, Japan), with differential counts determined by manual counting. Peripheral blood parameters on each day of collection are shown in Table 1.
Stem cells were collected according to the manufacturer's recommendations [7], by using a central venous access (allowing for a flow of at least 65 mL/min). Large-volume leukapheresis to process more than 3–5-times the blood volume was performed with both devices for the collection each day. The whole blood-to-anticoagulant (3,000 IU heparin with 500 mL of acid-citratedextrose solution) ratio was 24:1 in both devices.
The collection pump rate set for the COBE procedures was 1.0–1.3 mL/min, and the separation factor remained constant during the apheresis procedure regardless of the actual WBC count. When we used the Optia MNC system, collection preference was determined by the device algorithm. Buffy coat collection from the elutriation chamber was triggered manually when the operator observed a buffy coat overflow earlier than the red blood cell sensor. Patients undergoing stem cell collection were assigned to the COBE or Optia MNC system in a random manner.
CD34+ cells were counted in pre- and post-apheresis peripheral blood samples and in a product sample by flow cytometry (FACS Canto II, Becton, Dickinson and Company, San Jose, CA, USA), using a single-platform assay (BD stem cell enumeration kit, Becton Dickinson and Company) [1314].
The CD34+ cell dose per kg body weight was determined. The apheresis target dose for one autologous SCT was ≥3×106 CD34+ cells/kg body weight before freezing. The collection efficiency was calculated by using the widely accepted ‘CE2’ model [1516] as follows: (Total CD34+ cells obtained from apheresis ×100)/[Peripheral CD34+ cells/µL×Apheresis volume processed (µL)].
PLT loss during apheresis was calculated by using the formula: % PLT loss=[(PLT per µL before apheresis-PLT per µL after apheresis)/PLT per µL before apheresis]×100 [1617].
All statistical analyses were performed by using Stata Statistical Software Release 12 (StataCorp LP, College Station, TX, USA). Descriptive data are presented as median with range. Comparisons were made by using Fisher's exact test, Mann-Whitney U test, as appropriate; P<0.05 was considered statistically significant.
The 74 patients underwent a total of 216 autologous apheresis procedures. There were no differences in sex, age, body weight, diagnosis, mobilization regimens, and duration of collection between the COBE and Optia MNC groups (Table 1).
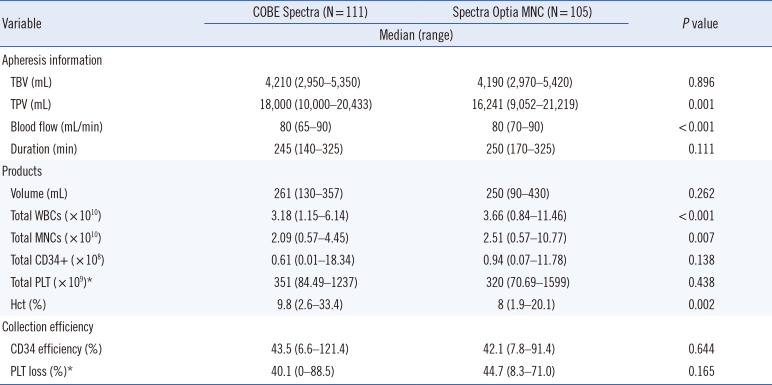
All procedures were well tolerated and no signs of clinical adverse events such as citrate toxicity were observed for any of the apheresis procedures. The details of performance of the two apheresis systems are summarized in Table 2. The total processed volume (TPV) was higher in the COBE group (P=0.001), whereas the flow rate was lower in the COBE group than in the Optia MNC group (77 mL/min vs 81 mL/min, P<0.001). However, the total procedure time was similar in the two groups (P=0.111). The parameters for stem cell preparations are summarized in Table 2. The volume of the stem cell preparations was similar in the two systems (P=0.262). Although WBC (P<0.001) and MNC (P=0.007) counts were significantly higher and Hct (P=0.002) was significantly lower in preparations collected by Optia MNC than by COBE, there were no significant differences in total CD34+ (P=0.138) and PLT (P=0.438) counts. The median CD34+ collection efficiency by the COBE and Optia MNC systems were similar (43.5% vs 42.1%, P=0.644), as were PLT losses after apheresis (40.1% vs 44.7%, P=0.165). Patients who received PLT transfusions before stem cell collection were excluded from the calculation of PLT loss (Table 2).
The present results showed that the performance of two apheresis systems, COBE and Optia MNC, was comparable for autologous PBSC collection. Although the TPV was higher and the blood flow rate was lower with the COBE system than with the Optia MNC system, the procedure did not differ significantly. The higher flow rate observed with the Optia MNC system was likely due to the ability of this instrument to maintain a high flow rate in the allowable range. However, a previous study reported that the collection time for the same TPV was longer with the Optia MNC system than with the COBE system owing to discontinuous collection [18]. Moreover, the TPV was smaller using the Optia MNC system, which induces early termination of apheresis when the target dose is reached, even if a full apheresis cycle has not been completed [8].
Previous studies have reported conflicting results about product volumes with these two systems. One study found that the product volume and TPV were lower with the Optia MNC system than with the COBE system [16]. Another study, which compared three different apheresis systems (COM.TEC [Terumo BCT], COBE, and Optia MNC) found that the product volume was lowest with the COBE system [18]. In contrast, our comparison of the Optia MNC and COBE systems showed no significant differences in product volume. Although sex, age, body weight, diagnosis, mobilization regimens, and collection duration were similar in the two groups, the peripheral blood WBC count was significantly higher in the Optia MNC group. Stem cell preparations obtained with the Optia MNC system may therefore have higher WBC and MNC counts. This result is in contrast to that of a previous study [19]. Although the peripheral blood PLT count was higher in the Optia MNC group, there were no significant differences in PLT counts in blood products and in PLT loss between the two groups. The Hct level in blood cell preparations was significantly lower in the Optia MNC group, consistent with previous findings [20]. This may reflect the chamber system in Optia MNC, which reduces non-target cells in the final product. Moreover, a similar CD34+ collection efficiency was observed in the two groups, consistent with previous studies. Although this study was conducted at a single center, the results demonstrate that the collection efficiencies of Spectra and Optia MNC are comparable.
 XML Download
XML Download