

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor,
Ceftolozane-tazobactam (C/T) and ceftazidime-avibactam (CZA) were recently approved for the treatment of complicated intra-abdominal infections and complicated urinary tract infections (http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm427534.htm, http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm435629.htm, both accessed February 24, 2016). To date, only one study has simultaneously evaluated the activities of C/T and CZA in vitro against Pseudomonas aeruginosa, and few studies have evaluated the effects of these antibiotics on multi-drug resistant (MDR) gram-negative bacteria [123]. This study aimed to examine the activities of C/T and CZA against β-lactam-resistant Enterobacteriaceae and P. aeruginosa clinical isolates.
The isolates were recovered from clinical specimens at Barnes-Jewish Hospital (St. Louis, MO, USA) from September to December 2014. Specimen sources included respiratory, blood, urine, and wound samples. Isolates of Enterobacteriaceae were included if they tested non-susceptible to cefepime and/or had an extended-spectrum β-lactamase (ESBL)-producing phenotype. P. aeruginosa isolates were included if they tested non-susceptible to meropenem. We included carbapenem-resistant Enterobacteriaceae isolates recovered from August 2012 to December 2014; these strains were tested for the blaKPC and blaNDM genes by real-time PCR [45]. All isolates were negative for the blaNDM gene.
Frozen stocks of all isolates were subcultured twice consecutively on 5% sheep's blood agar (Hardy Diagnostics, Santa Maria, CA, USA) prior to antimicrobial susceptibility testing (AST). Species-level identification was confirmed by using the VITEK MS system (IVD v2.3.3, bioMérieux, Durham, NC, USA) [67]. AST was performed by using gradient diffusion (Etest, bioMérieux). In brief, a 0.5 McFarland standard suspension of each isolate was inoculated onto Mueller-Hinton agar (Hardy Diagnostics), and Etest strips were applied. Plates were incubated overnight at 35℃ in ambient air. Each day, QC strains (Escherichia coli ATCC 25922 and ATCC 35218, and P. aeruginosa ATCC 27853) were tested. C/T and CZA results and QC were interpreted by using Food and Drug Administration breakpoints. The categorical interpretation and QC ranges for all other antibiotics (BD BBL and Co., Sparks, MD, USA) were based on standardized disk diffusion criteria [8].
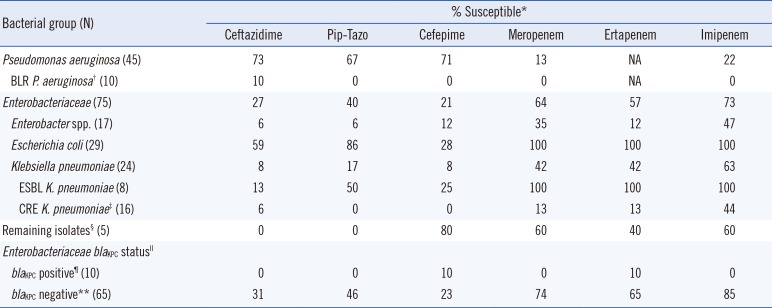
We evaluated 120 clinical isolates comprising 45 P. aeruginosa strains and 75 Enterobacteriaceae strains. Table 1 shows the overall β-lactam susceptibility profile. A subset of P. aeruginosa isolates (n=10, 22%), termed “β-lactam-resistant (BLR)”, were resistant to piperacillin/tazobactam, cefepime, meropenem, and imipenem.
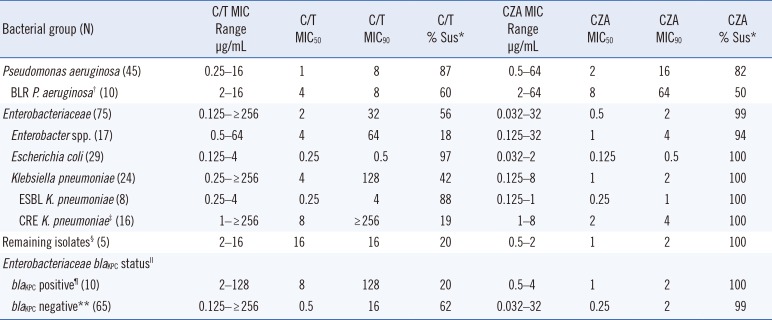
The 50% minimum inhibitory concentration (MIC50, 1 µg/mL) and 90% minimum inhibitory concentration (MIC90, 8 µg/mL) of C/T were lower for the P. aeruginosa isolates than for the Enterobacteriaceae isolates (2 µg/mL and 32 µg/mL, respectively; Table 2). Furthermore, 87% (n=39) of all P. aeruginosa isolates and 60% (n=6) of the BLR P. aeruginosa isolates were C/T-susceptible (Table 2).
Within the Enterobacteriaceae, the C/T data showed group-dependent differences. For example, the E. coli isolates had a low MIC90 (0.5 µg/mL), whereas the Enterobacter spp. had a higher MIC90 (64 µg/mL). Overall, 56% (n=42) of all Enterobacteriaceae isolates were C/T-susceptible (Table 2).
In contrast to the C/T results, the Enterobacteriaceae had lower MIC50 (0.5 µg/mL) and MIC90 (2 µg/mL) values for CZA compared to the P. aeruginosa isolates (2 µg/mL and 16 µg/mL, respectively; Table 2). Notably, 82% (n=37) of all P. aeruginosa isolates were CZA-susceptible (Table 2), whereas 99% (n=74) of Enterobacteriaceae isolates were CZA-susceptible. An Enterobacter spp. isolate was CZA-resistant (MIC of 32 µg/mL), but was found to be negative for the blaKPC and blaNDM genes by real-time PCR.
Comparison of the P. aeruginosa C/T and CZA results showed 87% (n=39) concordance with 35 isolates testing susceptible and four isolates testing non-susceptible to both antibiotics. For the Enterobacteriaceae, there was only a 57% concordance between the C/T and CZA results; 42 isolates tested susceptible and one isolate tested non-susceptible to both antibiotics. All remaining isolates were only CZA-susceptible.
The availability of new agents with anti-gram-negative activity holds promise for treating MDR organisms. CZA provides an alternative treatment for blaKPC-positive organisms, which are otherwise treated by agents with less desirable safety or efficacy profiles. Ceftolozane is a new cephalosporin with activity against P. aeruginosa, and in combination with tazobactam shows activity against ESBL-producing Enterobacteriaceae [9]. Notably, although two of the blaKPC-positive isolates were C/T-susceptible, we would not expect C/T to be clinically effective.
In summary, we report the activities of C/T and CZA against a collection of BLR Enterobacteriaceae and P. aeruginosa isolates. Our results suggest that C/T and CZA are active against and represent possible therapeutic options for infections with BLR gram-negative bacteria.
 XML Download
XML Download