

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The manual tube method is the reference method for pre-transfusion testing; however, it involves a sophisticated and time-consuming process [1]. Moreover, this test has drawbacks with respect to the reporting of results owing to the subjective nature of the interpretation of variables, which largely depends on the skill and experience of the technician [2]. This issue results in human errors, indicating that such subjective interpretations should be avoided to guarantee safe transfusion [3]. Many laboratories in tertiary-care hospitals have begun to routinely use automated systems for this purpose [45], because of the increasing demand for tests such as routine blood group testing, cross-matching, and antibody screening [6]. The use of an automated system has many well-known advantages [678]. Currently, various automated systems are available, and laboratories can select the most appropriate analyzer for their specific needs [6]. Especially, the AutoVue system (ORTHO AutoVue Innova System; Ortho-Clinical Diagnostics, Raritan, NJ, USA), has been widely used and has well-known advantages. On the basis of several studies, the system showed high concordance rate with manual method and also has shorter turnaround time than the manual method or the other systems [6910]. In addition, the system has high detection rate of alloantibodies compared with other methods [6101112]. Despite these studies, there was no study focused on specific reaction patterns or strength.
Our hospital's laboratory for transfusion services offers a 24-hr service to all departments of the hospital, including the emergency unit. Approximately 25,000 tests are performed annually for ABO typing before transfusion in this laboratory. In addition to ABO typing tests, antibody screening and cross-matching tests are routinely performed with manual methods. Without an automated system, this results in a heavy workload, leading to significant operational problems [3].
Although automated analyzers have many advantages, they occasionally show discrepant results between forward and reverse typings of the blood samples [13], such as weak cell or serum reaction, and extra serum reaction. In previous studies, such discrepant results were more frequently observed in reverse typing than in forward typing [314]. Especially, weak serum reactions are frequently observed with blood samples from immunocompromised patients, the elderly, and children [15]. Such discrepant results cause interruptions in the work process and may require manual processing, even when they do not affect the confirmation of ABO blood types. In addition, in our experience, discrepant results can show up during continuous follow-up. Moreover, automated analyzers can show specific error messages of technical origin. Therefore, the reference manual method is still considered useful for the retesting and confirmation of results obtained with automated analyzers.
In this study, we confirmed the proportion of samples that needed to be reevaluated by the reference manual method for ABO blood typing in a routine work process. In addition, we investigated the causes of the discrepancies seen in the results obtained with an automated system, with a particular focus on weak serum reactions.
METHODS
1. Blood samples
Blood samples were obtained from a transfusion service laboratory of a tertiary-care hospital in Korea, which routinely performs blood-typing for pre-transfusion testing. The study was conducted on samples obtained over a 7-month period, from August 2015 to February 2016. From the 13,261 samples collected in total, 148 samples that were tested only by the manual method because of an insufficient sample amount (including samples collected from infants, up to 1 yr of age) were excluded. The remaining 13,113 samples were tested with the AutoVue system, and all samples were retested by the manual method for confirming ABO types. The samples were collected in ethylenediamine tetraacetic acid tubes and were deemed adequate for testing (lipemic or hemolytic samples were rejected and new samples were requested).
2. ABO typing using the AutoVue system
The 13,113 samples were tested with the AutoVue system following the manufacturer's recommendation. The AutoVue system is a fully automated system based on column agglutination technology. The device uses barcoded samples, and the test results are recorded automatically at the final step. The analyzer has specific cassettes (ABO-Rh D/Reverse Typing Cassette; Ortho-Clinical Diagnostics, Inc.) that consist of six columns, five of which contain glass beads, buffers, and reagents including anti-A, anti-B, anti-D, A1 cells, and B cells (0.8% Affirmagen, A1 and B cell suspension; Ortho-Clinical Diagnostics, Inc.) for ABO and D typing (in this study, we only used the ABO typing columns). The sixth column serves as a negative control well; it only contains the red cell suspension of the sample. During the centrifugation of the cassettes, non-agglutinated red cells sink to the bottom of the column, while agglutinated red cells remain at different levels of the column according to the amount of agglutination. The reactions are graded as –, 0.5+, 1+, 2+, 3+, or 4+ by the system's software to represent the strength of the reaction. Each sample is classified into a specific blood group according to the results of forward and reverse typings interpreted by the system's software. In addition, uninterpretable results (unsuccessfully graded results) are displayed with specific error messages.
3. ABO typing by the reference manual method
The same 13,113 samples were retested by the manual method following the laboratory's standard procedure and manufacturer's recommendations. The samples were centrifuged before the test. For forward typing, one drop each of anti-A and anti-B reagent (Blood typing reagent IgM monoclonal; Millipore, Livingston, West Lothian, UK) was added to each test tube containing one drop of a 2–5% red cell suspension. For reverse typing, one drop of each of A and B cell reagents (3% Affirmagen; Ortho-Clinical Diagnostics, Inc.) was added to each test tube containing two drops of the plasma sample. As an auto control, the red cells and serum of the sample were reacted together in another test tube. The results were interpreted macroscopically and graded as –, 0.5+, 1+, 2+, 3+, or 4+. The ABO types were recorded according to the results of forward and reverse typings.
4. Evaluation of forward and reverse discrepancy of the AutoVue
In case of discrepancy between forward and reverse typing results, the samples were retested with the automatic analyzer. Samples that showed discrepant results after retesting were tested by additional manual methods. Among the 297 samples yielding discrepant AutoVue results, 284 (13 samples from stem cell transplant [SCT] recipients were omitted) were re-evaluated by using anti-AB (ABO3; DIAGAST, Loos, France), anti-H (monoclonal; ImuMed, Bammental, Germany), and anti-A1 (Dolichos biflorus lectin; ImuMed) reagents. One drop of each of anti-AB, anti-A1, and anti-H reagent was added to each test tube containing one drop of a 2–5% patient red cell suspension. The results were interpreted macroscopically and graded as –, 0.5+, 1+, 2+, 3+, or 4+. In case of suspected ABO subgroup samples (samples showing weak red cell or mixed field reaction) after this test, we recommended an ABO genotyping to the patient's physician and followed up the result. Genotyping was done by another laboratory. For further evaluation of the remaining discrepant results, we used antibody screening, antibody identification, and the Coombs test for samples showing extra serum reaction (results were again graded as 0.5+, 1+, 2+, 3+, or 4+ as described above). We measured total immunoglobulin in the samples still showing weak serum reaction (<2+ reaction grade) by the manual method to check the actual immunoglobulin level. If cold agglutinins were suspected, the sample was incubated at 37℃ and at room temperature for 30 min after saline washing, and then retested.
5. Interpretation of test results
The results were described as the reaction grades obtained with each method. The results obtained with the AutoVue system and the manual method were interpreted as discrepant according to the following in-house criteria. Firstly, a forward typing result showing a ≤2+ reaction grade (weak red cell reaction) and a mixed field reaction were regarded discrepant. Secondly, a reverse typing result showing a <2+ reaction grade (weak serum reaction) was regarded discrepant because serum reactions are usually weaker than cell reactions [1516]. Finally, results showing extra cell or serum reactions (including any reaction grade) were regarded as discrepant results.
In addition, because we found that serum reactions in the AutoVue tended to be weaker than those in the manual method during the study period, we traced the samples with 2+ AutoVue serum reaction grades (not including mixed field and extra serum reaction) and compared the results with those of the manual method.
Finally, the samples showing discrepant results on the AutoVue system were classified into their predicted blood group before confirmation by the manual method. The final reported ABO blood type results were confirmed by the manual method with further evaluation.
6. Statistical analysis
The percentage of discrepant results of the AutoVue system was calculated. The proportions of samples showing a weak serum reaction in the two methods were calculated. Statistical analyses were performed by using the SPSS software (SPSS Statistics, ver. 18; IBM, Armonk, NY, USA). P value <0.05 was considered statistically significant.
RESULTS
1. Results of ABO blood typing by the AutoVue system
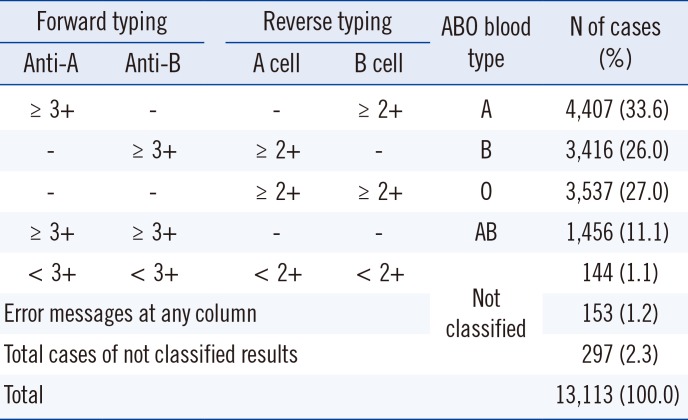
In total, 13,113 samples were tested by using the AutoVue system for ABO blood typing. Among them, 12,816 samples (97.7%) were successfully graded and classified into ABO blood groups. The remaining 297 samples (2.3%), including 153 samples with system error messages, showed discrepant forward and reverse typing results (Table 1). Among the successfully graded samples, 4,407 samples were of blood type A, 3,416 samples were of blood type B, 3,537 samples were of blood type O, and 1,456 samples were of blood type AB.
2. Results of ABO blood typing by the manual method
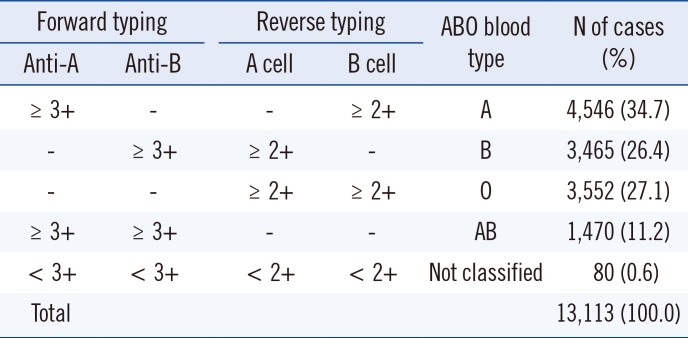
Of the 13,113 samples retested with the manual method, 13,034 samples (99.4%) were successfully graded and classified into an ABO blood group. The remaining 79 samples (0.6%) showed discrepancy between forward and reverse typing results (Table 2). Among the successfully graded results, 4,547 samples were of blood type A, 3,465 samples were of blood type B, 3,552 samples were of blood type O, and 1,456 samples were of blood type AB. Except for the samples that showed discrepant AutoVue results, the same results were obtained with the manual method as with the AutoVue system.
3. Discrepant results from the AutoVue system and the manual method
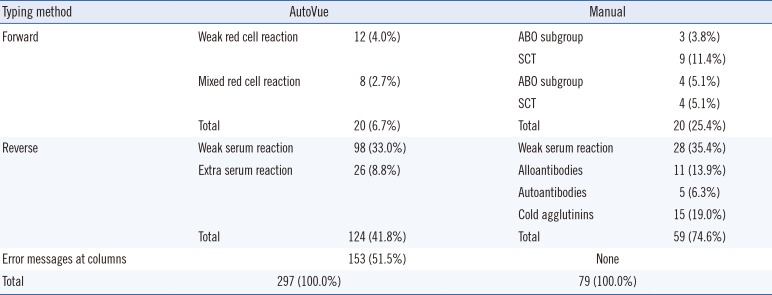
Among the 13,113 samples, discrepant results were produced for 297 samples (2.3%) by the AutoVue system and for 79 samples (0.6%) by the manual method. The 297 samples showing discrepant AutoVue results were re-evaluated by the manual method as well as by additional methods (Table 3). Twenty and 124 samples showed forward and reverse typing discrepancies, respectively. In the AutoVue system, forward typing revealed 12 weak cell reactions; three were of ABO subgroups, and nine were samples from SCT recipients in the manual method. Eight samples showed mixed field reactions; four were of ABO subgroups, and four were samples from SCT recipients. Among the samples showing weak serum reactions in reverse typing with the AutoVue system, 23 samples showed <2+ reaction grade, five had actual, low immunoglobulin level, and 70 showed normal serum reaction (no discrepancy) in the manual method. Among 26 samples showing extra serum reaction, there were 11 samples with alloantibodies, five with autoantibodies, and 10 with cold agglutinins in the manual method. The five samples with cold agglutinin were detected only by the manual method. The remaining 153 samples only showed a specific system error message. The error messages are indicated as numbers, each representing a specific technical problem, such as too many cells, light too low or high, wrong liquid level, empty well, indeterminate reaction except for a mixed field reaction. Such messages show up when the system cannot read the cassette or the system cannot interpret the results. Such errors could not be verified by the manual method because they are specific to the AutoVue system.
4. Discrepancies caused by weak serum reaction in the AutoVue system
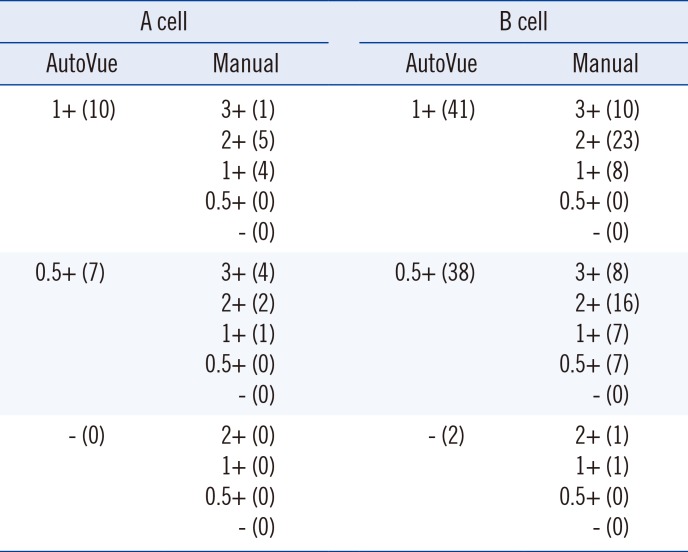
Among the 297 samples showing discrepancy, 98 samples showed a weak serum reaction in the AutoVue system (Table 4). Among these, 79 samples (80.6%) showed a greater reaction grade in the manual method than in the AutoVue system (P=0.01). The remaining 19 samples showed the same reaction grade with both methods. Weak serum reactions were more frequently observed in samples reacted with B cells (81, 82.7%) than in those reacted with A cells (17, 17.3%) (P=0.01).
Among the 98 samples showing a ≤1+ reaction grade in the AutoVue system, 70 samples (71.4%) showed a ≥2+ reaction grade (no discrepancy) with the manual method (P=0.05). Only 28 samples (28.6%) showed ≤1+ reaction grade of serum typing with both methods. Among these, five samples (17.9%) had a low immunoglobulin level, 15 samples (53.6%) had normal immunoglobulin level, and the immunoglobulin of the remaining eight samples (28.6%) was not evaluated (P=0.48).
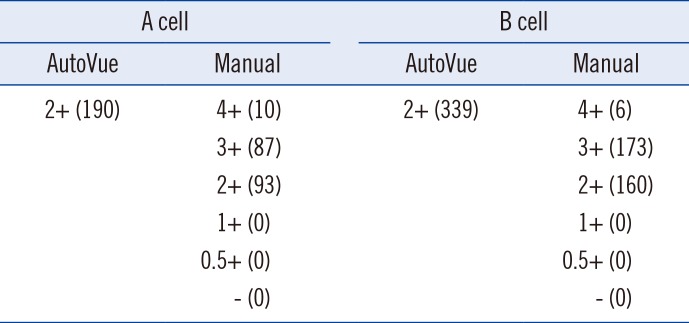
5. Results showing a 2+ serum reaction in the AutoVue system
The AutoVue system showed weaker serum reactions than the manual method; therefore, we compared 2+ serum reaction grade results of the system with the results obtained with the manual method for these samples (Table 5). Of the 529 samples showing a 2+ reaction grade in the AutoVue system, 276 samples (52.2%) showed a ≥3+ reaction grade in the manual method. The remaining 253 samples (47.8%) showed the same reaction grade with both methods. This finding revealed discrepancy between the 2+ reaction grade results between both methods.
DISCUSSION
Blood group typing is increasingly being automated in many laboratories [7]. In addition to blood typing, automated tests have also been used for the screening of unexpected antibodies and cross-matching in pre-transfusion evaluations [2317]. The AutoVue system is based on column agglutination technology, which is known to have higher sensitivity than the manual tube method. Furthermore, this automated system has already been shown to have good efficiency and standardized interpretation, with good quality assurance and other reliable properties [6].
However, this automated system occasionally shows discrepant results, requiring retesting with the manual method for the confirmation of ABO grouping. Therefore, we re-evaluated 13,113 AutoVue-typed samples with the manual method in a routine work process. As AutoVue forward typing yielded only 20 discrepant results (6.7%) whereas 124 discrepant results (41.6%) were observed with reverse typing, we focused on the latter in this study.
Among the 98 samples showing a weak serum reaction, 79 samples (80.6%) showed a greater reaction grade in the manual method than in the AutoVue system, 70 samples of which (71.4%) showed a normal serum reaction (≥2+ reaction grade) in the manual method. This result was not affected by the lot number of reagents used in the system over the course of the study (eight different lots of reagents were used during the study period) (P=0.8). This result might reflect inherent differences between the two methods, because the AutoVue system uses a 0.8% red cell reagent while the manual method uses 3% red cells. Among these 98 samples, a weak serum reaction was more frequently observed in the samples reacted with B cells than in those reacted with A cells. The reasons for this difference are unknown at present, but could be related to a biological aspect [18] and/or reagent-specific reaction. Among the 28 samples showing a weak serum reaction in both methods, 14 samples were from immunocompromised patients and the weak reaction of the remaining 14 samples could not be explained on the basis of the patients' clinical courses. Five of these samples (17.9%) showed low immunoglobulin levels, and 15 samples (53.6%) had normal immunoglobulin levels; however, the difference was not statistically significant because of the small sample size. This difference may be due to age-related factors and the patient's immune status. Therefore, these patients should be examined closely for a more precise evaluation. Further, our results suggest that samples showing <2+ reaction grade in reverse typing with the AutoVue system might actually show a weak or normal serum reaction in the manual method; therefore, such results should be evaluated by the manual method. By contrast, all samples showing a 2+ reaction grade in the AutoVue system showed a ≥2+ reaction grade in the manual method, suggesting that these results do not need to be re-evaluated with the manual method.
Moreover, there were several samples with extra serum reactions, ABO subgroup, derived from SCT patients, or eliciting error messages, indicating that the manual method will still be needed in the work process for confirmation. One hundred fifty-three samples (1.2%) produced error messages on the AutoVue system; these results will need to be further evaluated with respect to technical aspects of the system. Nevertheless, the samples requiring confirmation represent only a small proportion of the total (297 samples, 2.3%), suggesting that these extra steps would not cause substantial interruption of the routine work process. In addition, the cold agglutinins detected exclusively with the manual method were not clinically significant, and therefore, did not require additional evaluation.
This study had limitations. Firstly, because of limited in-house resources, we had to outsource the ABO genotyping of samples. This might have affected the discrepant results by the manual method, especially for ABO subgroups. Secondly, because of limited sample amounts, we could not measure the total immunoglobulin level in eight out of 28 samples showing weak serum reactions in the manual method.
In conclusion, 297 AutoVue-tested samples (2.3%) needed to be re-evaluated with the manual method because of discrepant results; however, the majority of samples (12,816, 97.7%) tested in the AutoVue system showed comparable results by the manual method. The AutoVue system for blood typing appears to be adequate for use in laboratories with a high workload and shortage of expert technicians. This study provides support for any laboratories with a blood bank considering using the manual method because of discrepant results, especially in reverse typing, from an automated system for blood typing.
 XML Download
XML Download