

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A reference interval is very important to medical practitioners in their interpretations of laboratory test results because the reference interval is a critical factor in clinical decision-making [1]. Regarding guidelines for defining reference intervals, they should be established on the basis of sufficient number of healthy people according to some partitioning criteria, such as age, sex, and ethnic background [2].
Partitioning into age groups according to sex is commonly applied to the establishment of reference intervals. Reference intervals for children need to be established because children differ in physiological development according to their age. However, there are some limitations and ethical considerations with respect to recruiting a large sample of healthy children to establish reference intervals [1345]. There are some textbooks that provide reference intervals for children. However, most of these textbooks are based on test results retrospectively obtained from hospital-based pediatric subjects and traditional analyzers that are no longer used [67]. Also, some reference intervals were established by using a small number of children and covered a wide range of ages because of ethical considerations about the collection of blood samples from healthy children.
The Seoul Metropolitan Government Public Cord Blood Bank (Allcord) has been providing medical check-ups at approximately one year of age for children who donated their cord blood. This medical check-up includes a complete blood count (CBC) and serum iron status for identifying iron-deficiency anemia. Therefore, we could obtain values for clinical chemistry as well as for hematology and iron state-related clinical chemistry from the leftover samples from a large number of healthy community children at one year of age.
In this study, we established the reference intervals of hematology and clinical chemistry analytes for 1-yr-old children. Moreover, we analyzed the effect of the type of feeding (breast or formula) during the first 6 months on serum iron status at one year of age.
METHODS
1. Subjects and data collection
We conducted a retrospective analysis of the children who received a 1-yr medical check-up between 2010 and 2014. We selected data from children who were in good health according to the questionnaire responses, interview, and physical examination at the time of blood sampling. The questionnaire includes questions regarding the child's disease and allergic history after birth, medication history, feeding methods, and current condition. A physical examination, including measurement of body temperature, was performed by a pediatric physician. All of the children were full-term babies who were suitable for cord blood donation. Blood sampling was performed within one calendar month before or after the child's first birthday. Data from children in an iron-deficient state needed to be excluded to establish the reference interval for the hematology and chemistry tests. Therefore, we excluded data obtained from children who showed any of the followings: a mean corpuscular volume (MCV) lower than 70 fL, a ferritin level lower than 10 ng/mL, and a transferrin saturation less than 10% [8910].
A total of 887 children were initially enrolled: 446 boys (50.3%) and 441 girls (49.7%). Data obtained from children with suspected iron deficiency were excluded from the data used to establish reference intervals. A total of 534 children were enrolled as the reference sample group to establish reference intervals for hematology analytes: 247 boys (46.3%) and 287 girls (53.7%). Their mean age was 363 (range, 335-395) days. The mean±SD body weight was 10.5±1.4 kg for boys and 9.9±1.5 kg for girls. The mean±SD height was 77.2±3.4 cm for boys and 75.4±3.5 cm for girls. If the blood sample volume was insufficient, only hematology tests were performed. Therefore, of the 534 children in the reference sample group, 177 (77 boys [43.5%] and 100 girls [56.5%]) were enrolled as the reference sample group to establish reference intervals for chemistry analytes. To evaluate the effect of the type of feeding during six months after birth on serum iron status, data obtained from children with information about the feeding methods were included. This study was reviewed and approved by the Institutional Review Board at Boramae Hospital (IRB No. 16-2013-75).
2. Hematology and clinical chemistry tests
The hematology and clinical chemistry tests were performed as soon the blood samples were obtained. Hematology tests (CBC count) were analyzed by using an automated blood cell counter (XE-2100; Sysmex, Kobe, Japan). The following hematology values were analyzed: Hb; Hct; red blood cell (RBC) count and indices such as the MCV, mean corpuscular Hb (MCH), mean corpuscular Hb concentration (MCHC), and red cell distribution width (RDW); white blood cell (WBC) count and differential count; and platelet count. The chemistry tests were performed using an automated chemistry analyzer (Modular Analytic; Roche Diagnostics, Indianapolis, IN, USA).
The following clinical chemistry values were analyzed: total calcium (Ca), inorganic phosphate (P), glucose, blood urea nitrogen (BUN), creatinine (Cr), uric acid, total cholesterol, total protein, albumin, total bilirubin, alkaline phosphatase (ALP), AST, ALT, γ-glutamyl transpeptidase (GGT), total carbon dioxide (total CO2), triglyceride (TG), and HDL cholesterol (HDL-C) and LDL cholesterol (LDL-C). Ca was measured by using a reagent from Denka Seiken (Tokyo, Japan). P was measured by using a reagent from Wako Pure Chemical Industries (Osaka, Japan). Glucose, BUN, uric acid, total cholesterol, AST, and ALT were measured by using reagents from Shin Yang Pharmaceutical (Seoul, Korea). Cr, ALP, GGT, total CO2, TG, and LDL-C were measured by using reagents from Roche. Total protein, albumin, and total bilirubin were measured by using reagents from Asan Pharmaceutical. HDL-C was measured by using a reagent from Daiichi Pure Chemicals (Tokyo, Japan). The serum iron and transferrin iron-binding capacity (TIBC) were analyzed by using the same automated chemistry analyzer (Modular Analytics; Roche Diagnostics). Iron and unsaturated iron-binding capacity for the calculation of TIBC were measured by using reagents from Asan Pharmaceutical (Seoul, Korea). Transferrin saturation was calculated as the ratio of serum iron and TIBC multiplied by 100. Serum ferritin was analyzed by using an automated immunoassay system (Architect i1000SR; Abbott Diagnostics, Chicago, IL, USA) and reagents from Siemens Medical Solutions (Malvern, PA, USA).
3. Establishment of reference intervals
All calculations for determining reference intervals were based on the CLSI guideline (C28-A3c) [2]. The largest or smallest value was evaluated as an outlier and was excluded if the absolute difference between the largest or smallest value and the next largest or smallest value was equal to or greater than onethird of the range of all values. The mean, SD, and the 2.5th and 97.5th percentiles of the values of each test item were calculated. Data distributions were evaluated by using the Kolmogorov-Smirnov test, and reference intervals were determined by using the parametric method (mean±2 SD) for parameters following a Gaussian distribution. For parameters that did not follow a Gaussian distribution, reference intervals were determined by using a nonparametric method (2.5-97.5th percentile). The Student's t-test or Mann-Whitney U test, according to the distribution of data, was performed to ascertain the differences in mean values between boys and girls. The individual reference intervals according to sex were established when the mean difference between 2 groups was at least 25% of the interval between the 2.5th and 97.5th percentiles as estimated from the overall sample of the reference sample group.
4. Analysis of the effect of the type of feeding during the first 6 months after birth on serum iron status
According to the feeding method during the first six months after birth, we divided the children into four groups: only breastfeeding, mainly breastfeeding (with formula feeding subsidiary to breastfeeding), only formula feeding, and mainly formula feeding (with breastfeeding subsidiary to formula feeding). Data distributions were evaluated by using the Kolmogorov-Smirnov test. ANOVA or the Kruskal-Wallis test, according to the distribution of data, was performed to compare serum iron status according to the feeding groups. Differences were considered to be statistically significant when the P value was less than 0.05. All of the statistical calculations were performed by using SPSS version 12.0 (IBM Corp., Chicago, IL, USA).
RESULTS
1. Reference intervals for hematology and clinical chemistry analytes for 1-yr-old children
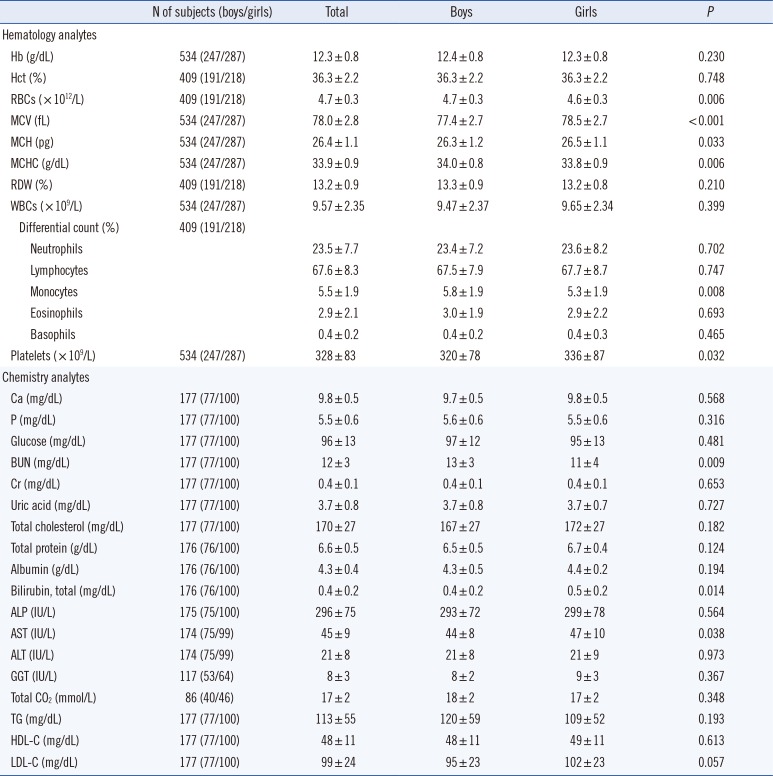
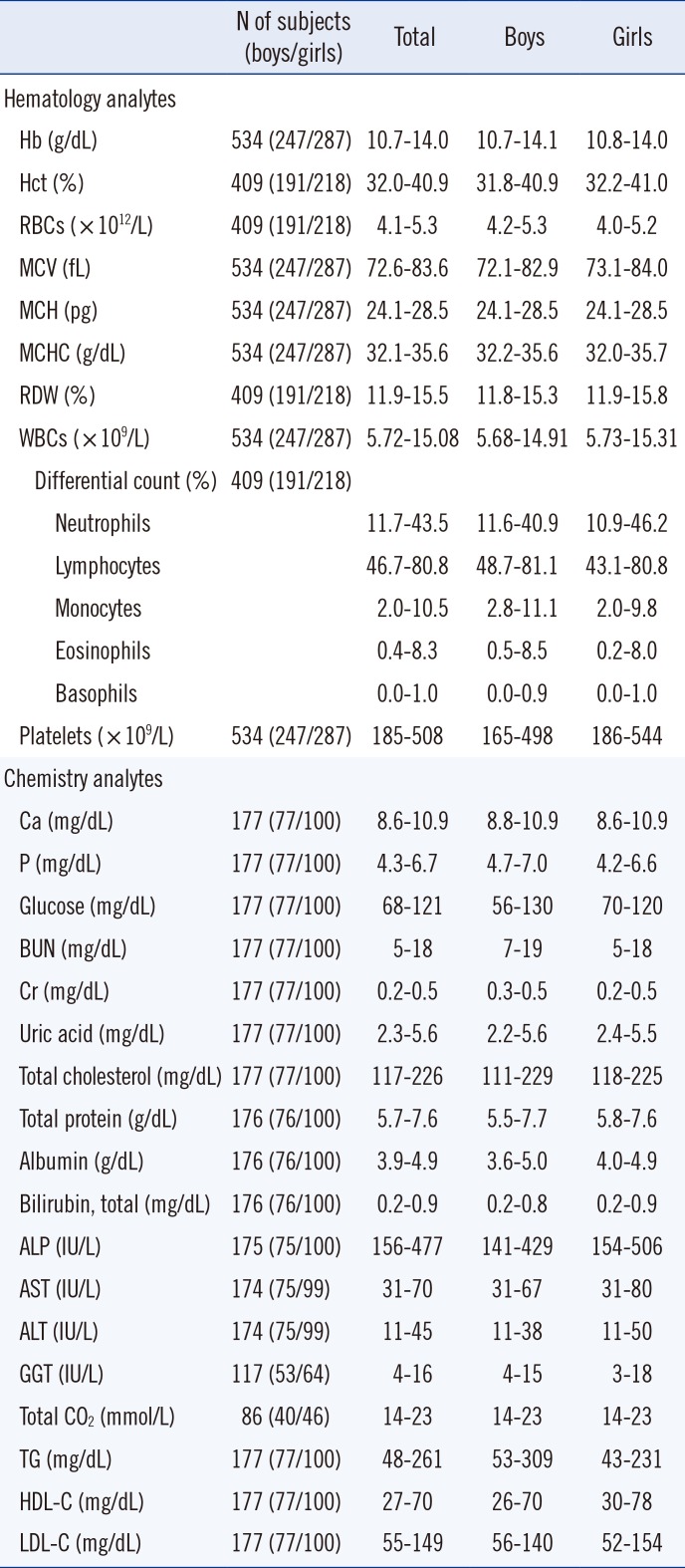
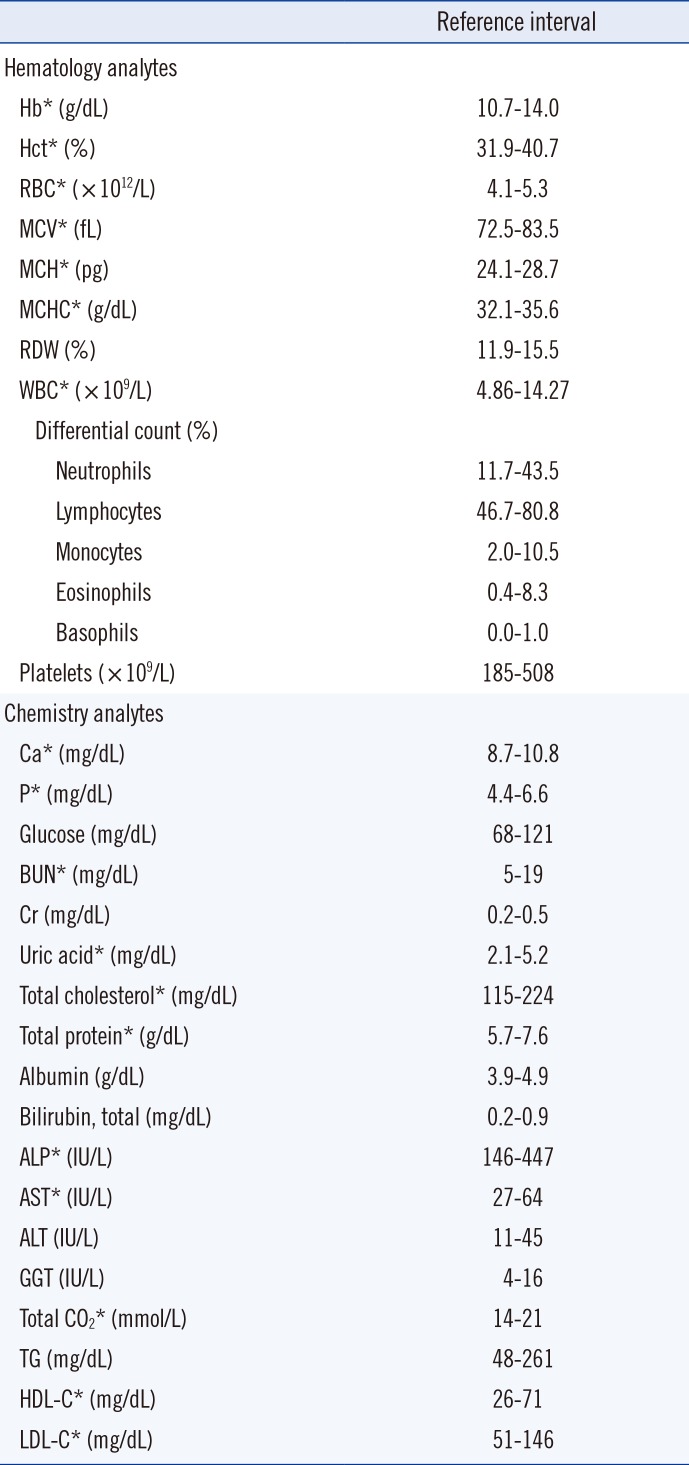
The hematology and clinical chemistry analyte values (mean±SD) of all children and those according to sex are shown in Table 1. The 2.5th and 97.5th percentile values of all children and those according to sex are shown in Table 2 (See Supplemental Data Table S1 for the values of further subdivided percentiles). Among the hematology analytes, the mean RBC count, MCV, MCH, MCHC, percentage of monocytes, and platelet count and, among chemistry analytes, the mean BUN and total bilirubin values showed significant differences according to sex. However, the mean differences between the sexes were less than 25% of the interval between the 2.5th and 97.5th percentiles estimated from the overall reference sample group. Therefore, we established the reference intervals without subgroup partitioning. Hb, Hct, RBC count, MCV, MCH, MCHC, and WBC count among hematology analytes and Ca, P, BUN, uric acid, total cholesterol, total protein, ALP, AST, total CO2, HDL-C, and LDL-C among chemistry analytes followed a Gaussian distribution. Therefore, the reference intervals for these analytes were established by using a parametric method (mean±2 SD). The reference intervals for the remaining analytes were established by using a nonparametric method (2.5-97.5th percentile). The reference intervals for the overall parameters are shown in Table 3.
2. The effect of the type of feeding during the first 6 months after birth on serum iron status
We obtained feeding information from 264 of 887 children: 136 in the only breastfeeding group (51.5%), 55 in the mainly breastfeeding group (20.8%), 16 in the only formula-feeding group (6.1%), and 57 in the mainly formula-feeding group (21.6%). The serum iron status according to the feeding group is shown in Table 4.
All of the parameters for iron status, such as serum iron levels, TIBC, ferritin levels, and transferrin saturation, significantly differed among the feeding groups (P <0.001). As the serum iron level, TIBC, and transferrin saturation data followed a Gaussian distribution, we could perform multiple-comparison tests. The multiple-comparison tests revealed that the serum iron levels of the only formula-feeding and mainly formula-feeding groups were significantly higher than the serum iron level of the only breastfeeding group. The serum iron level of the only formula-feeding group was also significantly higher than that of the mainly breastfeeding group. The TIBC of the mainly formula-feeding group was significantly lower than the TIBC of the other groups. The transferrin saturation values of both formulafeeding groups were significantly higher than those of the both breastfeeding groups. As the serum ferritin level data followed a non-Gaussian distribution, a multiple-comparison test could not be performed. However, the ferritin levels in both formula-feeding groups were higher than those in both breastfeeding groups. Overall, serum iron and ferritin levels were higher in the formulafeeding groups than in the breastfeeding groups.
DISCUSSION
In this study, which included a large number of 1-yr-old children, we established reference intervals of hematology and clinical chemistry analytes. Ethical considerations regarding the collection of blood samples from healthy children have been a strong limitation for the establishment of pediatric reference intervals [511]. In particular, blood sampling from healthy children of the 1-yr age group was very difficult with respect to ethical considerations. Recently reported studies of pediatric reference intervals did not include a younger age group [1213]. Therefore, reference intervals of children in textbooks represent retrospective data from hospitalized children [36].
Prospective and community-based studies for pediatric reference intervals have been performed for a large number of healthy children from Sweden, Canada, Denmark, and Germany [14151617181920212223]. These studies presented pediatric reference intervals for hematology and clinical chemistry parameters as well as hormones and lipids. Recently, reference intervals of clinical chemistry analytes for Korean children have been reported [12]. Children younger than two years of age could not be included as reference individuals owing to the small number of subjects.
The present study was conducted with children of a limited age group (one year of age). However, it is meaningful because a large number of healthy children in the household population of this age were included as reference individuals. We obtained the hematologic results from a sufficient number of healthy 1-yr-old children, with more than 500 results in total, and more than 200 results for each sex. Regarding the clinical chemistry results, we obtained more than 120 results from healthy children, except GGT and total CO2 owing to the low volume of blood samples. The number of reference individuals reflected a lack of presenting the sex-specific reference intervals. However, because the mean differences between boys and girls were less than 25% of the interval between the 2.5th and 97.5th percentiles, the overall reference intervals without subgroup partitioning were presented with a sufficient number of reference individuals.
To select healthy children, we excluded data obtained from children with suspected iron deficiency. In previous studies, iron deficiency was determined through the following parameters: MCV, ferritin, transferrin saturation, and soluble transferrin receptor level [8910]. However, as the soluble transferrin receptor level was not determined in our study, we excluded the complete data of children if even one of the parameters deviated from the criteria for excluding children with iron deficiency from healthy reference individuals.
The WHO has indicated the cutoff indicating anemia for 1-yr-old children as a Hb less than 11.0 g/dL [24]. Therefore, some studies have adapted the criterion of Hb less than 11.0 g/dL for excluding iron-deficiency anemia [825]. However, Hb levels are neither sensitive nor specific for iron status [26]. Furthermore, many previous studies have reported that the lower limit of the reference interval for Hb in young children is less than 11.0 g/dL [618]. In our study, the lower limit of the reference interval for Hb of 1-yr-old children was 10.7 g/dL for boys and 10.8 g/dL for girls. The German study established a reference interval for hematologic parameters using the same automated blood cell counter (Sysmex XE-2100) as in the present study [18]. Regarding the Hb level of 1-yr-old children, the German study showed a lower value of the lower limit of the reference interval of Hb than the present study. Also, the German study showed a higher level of the upper limit of the reference interval of the WBC count than the present study. The German study and previously published studies were performed on apparently healthy children among inpatients and outpatients [618]. Therefore, we proposed that these findings may be affected by the lower limit of the reference interval for Hb and the upper limit for the WBC count. The Swedish study established a reference interval for hematologic parameters using a different automated blood cell counter (Siemens Advia 2120) from our study; however, they evaluated healthy children recruited from community daycare centers and schools [21]. They reported a lower limit of the reference interval for Hb of young children (between six months and seven years of age) of 10.7 g/dL (i.e., less than 11.0 g/dL) for both sexes, which is consistent with our results.
In the present study, the platelet count of girls was significantly higher than that of boys, agreeing with the results of the German study and other previous studies [618]. The red cell indices (MCV, MCH, and MCHC) showed significant differences (P<0.001, P=0.033, and P=0.006, respectively) according to sex, but the differences were not substantial. Among the clinical chemistry analytes, BUN, total bilirubin, and AST showed significant differences according to sex. These results are in contrast with those obtained in previous studies reporting that young children before puberty showed no significant sex difference in the reference intervals of clinical chemistry analytes [1819].
The concentrations of serum lipids such as total cholesterol, HDL-C, LDL-C, and TG have been reported to be affected by the type of feeding (breastfeeding or formula-feeding) [2728]. Our statistical analysis revealed no significant differences in total cholesterol, HDL-C, LDL-C, or TG among the four feeding groups. Therefore, we presented the reference intervals independent of the feeding methods.
We also analyzed the effect of feeding during the first six months after birth on serum iron status. The duration of breastfeeding is associated with an increased risk of iron-deficiency anemia. Moreover, formula feeding strongly affects serum ferritin levels, and therefore, it is associated with a decreased risk of iron-deficiency anemia [8]. In addition, the time of introducing complementary feeding has been reported to affect the iron status of breastfeeding children [2930]. In the present study, most children (257/264, 97.3%) started weaning at approximately six months of age, and there was no significant difference in iron status according to the time of weaning (data not shown). Serum iron and ferritin concentrations and transferrin saturation were higher in children who were exclusively or mainly fed formula than in children who were exclusively or mainly fed breast milk during the first six months. Consequently, our study also showed that formula feeding affected iron status. In particular, the mean value of the ferritin concentration of the only breastfeeding group was 12 ng/mL, which was close to the level of the iron-deficiency state (<10 ng/mL).
This study was performed only in 1-yr-old children. Therefore, the pattern of age-dependent change in the hematology and clinical chemistry analytes could not be identified. However, this study was the first study to determine reference intervals based on a large number of samples collected from community-based healthy children in Korea. The results of our study provide basic data for the hematology and clinical chemistry analytes for the interpretation of the test results of 1-yr-old children.

 XML Download
XML Download