

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Smoking is a significant risk factor for a higher incidence of cancer and respiratory and cardiovascular diseases [12]. Accurate assessment of the epidemiology associated with current smoking status in different human populations is important for managing the negative effects of smoking and for developing a public health policy [3]. Although most assessments of smoking status are based on self-reported questionnaires, these are not completely objective and might underestimate the actual prevalence of current smokers, because respondents may conceal actual smoking habits [4]. Therefore, laboratory validation of biochemical markers is more accurate to assess current smoking status and health hazards associated with smoking [5].
Nicotine is the best marker of current smoking status because it is relatively unique to cigarettes; however, its half-life is short, between 2 and 3 hr. Approximately 90% of absorbed nicotine is transformed into its main metabolite, cotinine [6]. Cotinine is preferred over nicotine as a screening marker to identify current smokers because its average half-life is longer, approximately 18 to 20 hr [7]. Cotinine can be detected in different body fluids, including urine, blood, saliva, and seminal fluid, as well as hair [891011]. The choice of using urine samples is primarily influenced by practicability, because urine collection is noninvasive; however, this approach requires access to facilities for collection and can be problematic because of the relative ease of sample manipulation by subjects. Overall, many studies comparing nonsmokers with current smokers have consistently found that serum cotinine level can be used to accurately distinguish current smokers from nonsmokers [1213].
Racial/ethnic differences in rates of cigarette smoking and rates of nicotine and cotinine metabolism have been well described [1415]. A large Korean population study was conducted to investigate the optimal cut-off for urine cotinine levels for distinguishing current smokers from nonsmokers [16]. However, to the best of our knowledge, no studies have investigated the use of liquid chromatography–tandem mass spectrometry (LC-MS/MS) to measure serum cotinine and to determine the optimal cut-off for serum cotinine levels for differentiating current smokers from nonsmokers in the Korean population. In this study, we performed a correlation analysis of serum cotinine, assessing the relationship between serum cotinine measured using LC-MS/MS (henceforth, LC-MS/MS serum cotinine) and urine cotinine, and evaluated the optimal cut-off for serum cotinine levels in the Korean individuals.
Go to : 
METHODS
1. Data collection
Data were collected from healthy subjects (men and women) who underwent a comprehensive examination at Kangbuk Samsung Hospital Total Healthcare Center, Seoul, Korea, from January to February 2015. For smokers, only those who used cigarettes were included in the study; individuals currently using nicotine replacement therapy, electronic cigarettes, or other forms of nicotine (e.g., cigars) were excluded. On the basis of a retrospective review, subjects were randomly chosen to represent a broad distribution of urine cotinine levels. All subjects were free from any past or current disease states as well as any abnormal results of health check-up programs. The subjects were asked to complete a questionnaire about current smoking status. The questionnaire sought information about the number of cigarettes smoked daily, the age at smoking initiation, total smoking duration, and an estimate of the total number of lifetime cigarettes smoked. In total, 120 serum specimens were collected.
We obtained the results of the urine cotinine levels, which were assessed during a routine health check-up by the DRI Cotinine Assay for urine (Microgenics Corporation, Fremont, CA, USA) and Modular P (Roche Diagnostics, Rotkreuz, Switzerland). The DRI Cotinine Assay is a homogeneous enzyme immunoassay based on competition between cotinine labeled with the glucose-6-phosphate dehydrogenase enzyme and free cotinine. We applied a urine cotinine cut-off point of 100 ng/mL in reference to a previous study, in which nonsmoker urine cotinine levels did not exceed 100 ng/mL [17]. This level was lower than the manufacturer's recommended cut-off point of 500 ng/mL. On the basis of the manufacturer's recommended urine cotinine level, the subjects were classified into four groups: lower than analytical measurement range (AMR) (≤34 ng/mL; group 1), higher than AMR but lower than cut-off (34< and ≤100 ng/mL; group 2), lower than the manufacturer's recommended cut-off point (100< and ≤500 ng/mL; group 3), and above the manufacturer's recommended cut-off point (>500 ng/mL; group 4).
This study included 120 subjects with a mean age of 39.0 yr (range 27-62) who completed the questionnaire related to cigarette smoking and had already tested for urine cotinine. The subjects were randomly chosen to represent a broad distribution of urine cotinine levels in each group: 40 subjects in group 1, 20 in group 2, 40 in group 3, and 20 in group 4. The characteristics of the subjects are described in Table 1. The Institutional Review Board of our institute approved this study (2014-08-025).
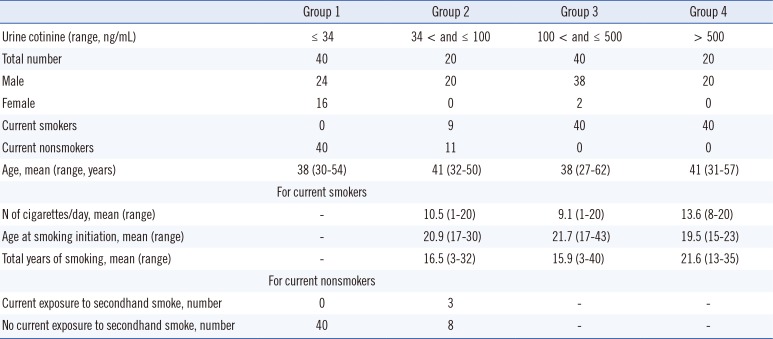
Table 1
Characteristics of subjects according to the groups based on urine cotinine levels
![]()
2. Determination of cotinine using LC-MS/MS
Serum cotinine levels were measured by using IMMULITE 2000 XPi (henceforth, IMMULITE serum cotinine) (Siemens Healthcare Diagnostics Inc., Flanders, NJ, USA) and LC-MS/MS (API-4000, Applied Biosystems, Foster City, CA, USA). The specimens were obtained prospectively and measured collectively at one time. IMMULITE 2000 XPi is a continuous random-access instrument that performs chemiluminescent immunoassay testing. For the measurement of LC-MS/MS serum cotinine, an additional performance evaluation analysis was performed. A stock solution of 4 mg/mL cotinine was prepared in methanol and stored at 4℃. Working solutions (10, 25, 50, 100, 500, 1,000, and 2,000 ng/mL) were prepared by serial dilution in deionized water. The calibrator was spiked with 100-µL aliquots of the working solution to yield a seven-point calibration curve (1, 2.5, 5, 10, 50, 100, and 200 ng/mL) for cotinine. A stock solution of 100 ng/mL cotinine-d3 internal standard (IS) was prepared in acetonitrile and stored at 4℃. A working solution of cotinine-d3 (10 ng/mL) was prepared by serial dilution in acetonitrile. The commercial sources for cotinine and cotinine-d3 were Sigma (Catalogue No. C5923, St. Louis, MO, USA) and CDN (Catalogue No. D3518, Quebec, Canada), respectively. Three levels of quality control (QC) materials (3, 80, and 160 ng/mL, respectively) were prepared by using an in-house method. A 100-µL aliquot of the QC sample, calibrator, or human sample; a 100-µL aliquot of the working IS; and an 800-µL aliquot of acetonitrile were mixed for 5 min and then centrifuged at 16,168g for 5 min. The supernatants were filtered by using a 0.22-µm syringe filter. Filtered samples were collected into 1-mL screw-capped vials.
The LC-MS/MS analysis was performed by using an Agilent 1,200 HPLC system interfaced with an API-4000 tandem mass spectrometer; the entire system was controlled by using the Analyst 1.4.2 program (Applied Biosystems). Chromatographic separation of cotinine and IS was achieved with a Kinetex 2.6u HILIC 100A column (2.1×150 mm2; 2.6-µm particle size; Phenomenex, Torrance, CA, USA). The temperature of the column was maintained at 40℃. A 3-µL aliquot of the filtered sample was injected into the column, and isocratic elution was performed in a mixed mobile phase [10 mM ammonium formate in 0.1% formic acid; acetonitrile=30:70 (v/v)] at a flow rate of 0.25 mL/min. The mass spectrometer was operated in the positive electrospray ionization mode, with a spray voltage of 5,500 V and a vaporizer temperature of 550℃. Ion source gas 1, ion source gas 2, curtain gas, and collision gas were set at 55 mL/min, 60 mL/min, 35 mL/min, and 5 mL/min, respectively. Multiple reaction monitoring transitions were monitored as follows: cotinine (m/z 177.2 → 97.9) and IS (m/z 180.2 → 100.9). The measured serum concentration was unconjugated cotinine, considering that we did not perform hydrolysis or an enzymatic procedure.
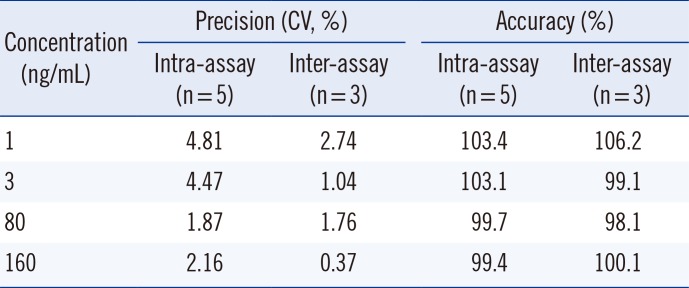
We evaluated serum cotinine measurements using LC-MS/MS, which included selectivity, accuracy, precision, and linearity. Fig. 1 shows the selectivity of this method. No noticeable interferences were observed in the chromatograms. Cotinine and IS were separated from the noise peaks, and IS was sufficiently separated from the front ghost peak. The intra-assay and inter-assay precision and accuracy were determined by using blank serum samples spiked with aliquots of cotinine solutions at four concentrations. Five samples of each concentration were prepared and the solutions were measured on the same day as that of the intra-assay. Inter-assay reliability was determined by measuring the calibration curve on three different days. The precision and accuracy are shown in Table 2. The quantitation limit of cotinine was 1 ng/mL. The standard curve was linear over the concentration range 1 to 200 ng/mL (r2 >0.99, with r as the regression constant).
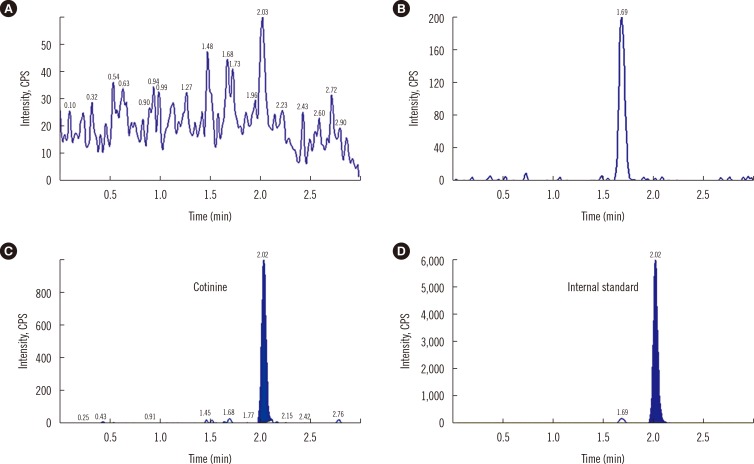 | Fig. 1Selectivity of serum cotinine using LC-MS/MS (A) Noise peaks (B) Front ghost peak (C) Cotinine (D) Internal standard (IS). No noticeable differences are observed in the chromatograms. Cotinine and the IS are separated from the noise peaks, and IS is sufficiently separated from the front ghost peak.Abbreviation: cps, counts per second; LC-MS/MS, liquid chromatography-tandem mass spectrometry.
|
Table 2
Intra-assay and inter-assay precision and accuracy of serum cotinine using LC-MS/MS
![]()
3. Statistical analysis
The IBM SPSS program version 18.0 (IBM, Armonk, NY, USA) was used for statistical analyses. Pearson correlation analysis was used to investigate the correlations between IMMULITE serum cotinine, urine cotinine, and LC-MS/MS serum cotinine levels. ROC curve analysis was used to identify the optimal cut-off for IMMULITE serum cotinine levels for distinguishing current smokers from nonsmokers. A P value of <0.05 was considered statistically significant.
RESULTS
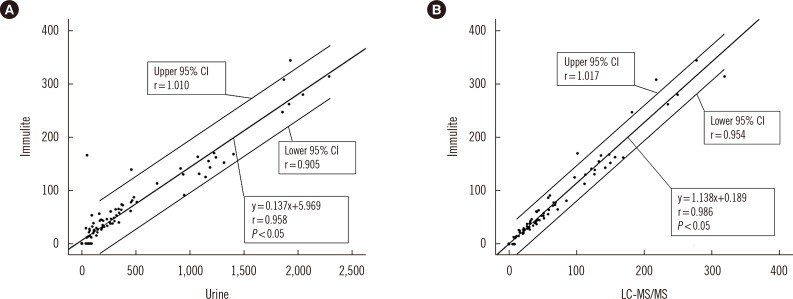
IMMULITE serum cotinine correlated with urine cotinine, with a correlation coefficient (r) of 0.958 (Fig. 2A). In addition, IMMULITE serum cotinine correlated with LC-MS/MS serum cotinine, with a correlation coefficient of 0.986 (Fig. 2B).
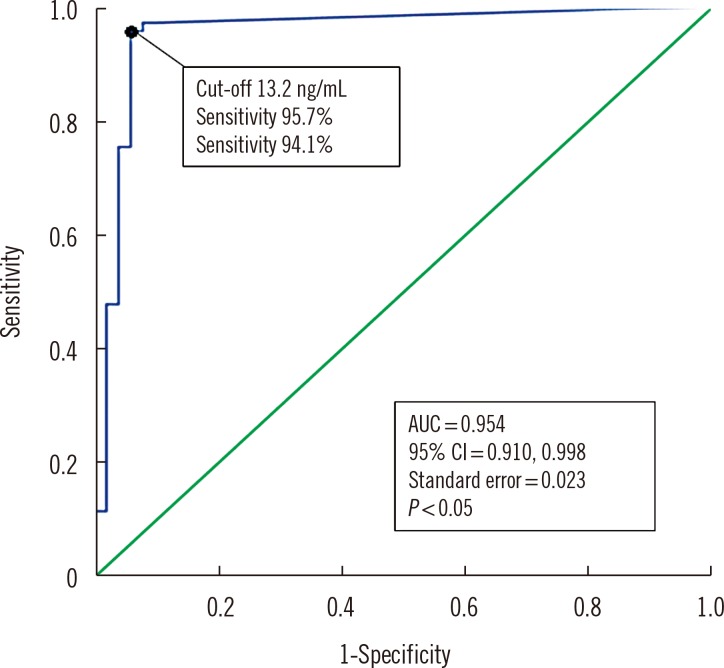
The optimal IMMULITE serum cotinine cut-off level for distinguishing smokers from nonsmokers was 13.2 ng/mL, with 95.7% sensitivity (95% confidence interval [CI], 87.0-98.9%), 94.1% specificity (95% CI, 82.8-98.5%), 95.7% positive predictive value (PPV), and 94.1% negative predictive value (NPV). The area under the curve (AUC) was 0.954 (95% CI, 0.910-0.998) (Fig. 3).
DISCUSSION
There is an overlap in cotinine values between less intense or less frequent active smokers and persons heavily exposed to secondhand smoke, and this overlap warrants the selection of a cut-off point that separates active smokers from nonsmokers exposed to secondhand smoke [14]. In Korea, a large population study based on a data set from the Korea National Health and Nutrition Examination Survey (KNHANES) from 2007 to 2010 reported that the optimal cut-off for urine cotinine levels for distinguishing current smokers from nonsmokers was 95.6 ng/mL in Korean males and 96.8 ng/mL in Korean females [16]. In addition, several studies have evaluated urine cotinine levels in the Korean population [18192021]. In a previous study, a discrepancy was detected among both self-reported smokers and nonsmokers, suggesting that the validity of questionnaires could be improved and highlighting the need for a more sensitive and reliable noninvasive biomarker of cigarette smoking [22]. Although self-voiding urine is a very useful noninvasive sampling method for measuring cotinine levels, subjects can manipulate the sampling procedure through water dilution or sample exchange, which can lead to false-negative results. In these cases, the measurement of serum cotinine levels was shown to be more reliable for differentiating misrepresentation of cigarette smoking status.
In our study, among the subjects who responded as nonsmokers, three showed an IMMULITE serum cotinine level higher than 13.2 ng/mL, indicating misrepresentation of smoking status. The first subject (NS11) had an IMMULITE serum cotinine level of 154 ng/mL, a LC-MS/MS serum cotinine level of 136.3 ng/mL, a urine cotinine level of 49 ng/mL, with the self-questionnaire indicating that the subject was currently exposed to secondhand smoke. In the second subject (NS3), these levels were 53.1 ng/mL, 51.2 ng/mL, and 93 ng/mL, respectively, whereas in the third subject (NS1), these levels were 28.9 ng/mL, 27.1 ng/mL, and 39 ng/mL, respectively. Both subjects reported that they were currently not exposed to secondhand smoke. The discrepancies between self-reported nonsmokers and serum cotinine levels higher than our optimal cut-off might be due to inaccurate information about smoking status or high exposure to secondhand smoke [2123]. The first subject (NS11), although currently exposed to secondhand smoke, had the highest level of IMMULITE serum cotinine among the three subjects, and it is highly likely that this subject falsely responded regarding current smoking status. Moreover, it is also probable that the second and third subjects (NS3 and NS1, respectively), who were self-reported nonsmokers and denied current exposure to secondhand smoke, falsely reported their current smoking status.
Among the subjects who responded as smokers, three showed an IMMULITE serum cotinine level lower than 13.2 ng/mL. The first subject (S65) had an IMMULITE serum cotinine level of 0 ng/mL, an LC-MS/MS serum cotinine level of 0 ng/mL, a urine cotinine level of 39 ng/mL and reported smoking 10 cigarettes per day; in the second subject (S66), these levels were 0 ng/mL, 7.3 ng/mL, and 56 ng/mL, respectively, and this subject reported smoking four cigarettes per day; in the third subject (S69), these levels were 11.6 ng/mL, 8.3 ng/mL, and 88 ng/mL, respectively, and this subject reported smoking 20 cigarettes per day. A previous study showed that discrepancies between self-reported smokers and serum cotinine levels lower than the optimal cut-off point might be due to occasional smoking or smoking a small number of cigarettes per day [23]. After cessation of smoking, blood and urine cotinine concentrations can decline to nonsmoking levels within 3-4 days [2425]. We suggest that the second subject (S66), who reported smoking the fewest cigarettes among the three subjects, showed a low level of IMMULITE serum cotinine because of occasionally smoking a small number of cigarettes per day. The first and third subjects (S65 and S69, respectively) might have shown low levels of IMMULITE serum cotinine because of occasional smoking. However, we could not contact these subjects for additional information regarding their exact smoking status before the health check-up or to recheck the self-reported questionnaire related to cigarette smoking.
Cotinine levels can vary depending on the racial/ethnic background. For example, at the same daily level of cigarette smoking, higher serum cotinine concentrations are observed in blacks than in whites, which is a result of slower cotinine metabolism and a greater intake of nicotine per cigarette among black individuals [2627]. A large population study conducted in the United States based on the National Health and Nutrition Examination Survey (NHANES) data set from 1999 to 2004 reported that the optimal cut-off for serum cotinine levels for differentiating current smokers from nonsmokers was 3.08 ng/mL in adults, with sensitivity of 96.3% and specificity of 97.4%. The optimal cut-offs differed by race/ethnicity, with levels of 5.92 ng/mL, 4.85 ng/mL, and 0.84 ng/mL in non-Hispanic blacks, non-Hispanic whites, and Mexican Americans, respectively [14].
Compared with the serum cotinine cut-off of 10 ng/mL, which is used in the US Centers for Disease Control and Prevention (CDC) studies [28293031], our study showed a relatively higher cut-off of 13.2 ng/mL in the Koreans. There could be several reasons for this difference. First, the Koreans may have a slower metabolism of cotinine relative to the individuals assessed in the NHANES study. Second, the Koreans may experience a greater intake of nicotine per cigarette or a greater exposure to secondhand smoke. Third, there are differences in cotinine measuring methods between the two studies; while the NHANES study used the HPLC/atmospheric pressure ionization tandem mass spectrometry method, our study used the chemiluminescent immunoassay method.
Several studies have demonstrated the important role of cytochrome P450 2A6 (CYP2A6) in the C-oxidation of nicotine to generate cotinine [323334]. The degree of variation in the metabolism of nicotine in humans may be due to the variable expression of CYP2A6 [7]. A previous study in the Korean population showed that heterozygotes of the CYP2A6*4 allele tend to possess a lower metabolic ratio, and homozygotes of the CYP2A6*4 allele were completely deficient in cotinine formation [35].
There are several limitations in our study. First, the sample size was relatively small. Second, we could not obtain subject data related to CYP2A6 alleles or to drugs. Third, our study was retrospective. Considering the selection of subjects, it would have been preferable to perform a controlled trial where several variables (e.g., the daily number of cigarettes smoked, age at smoking initiation, total smoking duration, and total number of lifetime cigarettes smoked) are steadily monitored. A large, controlled population study to investigate the optimal cut-off for serum cotinine levels would be useful in the future.
To the best of our knowledge, this is the first study to comparatively investigate serum cotinine levels using LC-MS/MS and to determine the optimal cut-off for serum cotinine levels for distinguishing current smokers from nonsmokers in the Korean population. We suggest that, relative to other racial/ethnic groups, the higher serum cotinine cut-off of 13.2 ng/mL in the Koreans found in our study is most likely due to the slower metabolism of cotinine, differences in smoking behavior, or secondhand smoke exposure status. The present results could provide guidelines for differentiating current Korean smokers from nonsmokers.
Go to :
 XML Download
XML Download