

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Serum level of amino-terminal pro-B type natriuretic peptide (NT-proBNP) is a prognostic marker of adverse outcomes among patients with preexisting and newly diagnosed heart failure (HF) [12]. NT-proBNP levels also correlate with acute coronary syndrome (ACS), and have slightly better prognostic sensitivity than cardiac troponin levels. In low risk patients, combining cardiac troponin and NT-proBNP in a "rule-out" marker-based model may provide an opportunity to safely discharge these patients without stress testing, which would spare individual patients and the healthcare system much effort and cost [34].
Numerous diseases, other than those involving the heart, such as septic shock, acute respiratory distress syndrome, acute pulmonary embolism, renal failure, and brain hemorrhage are also associated with an elevated serum NT-proBNP level [5]. Furthermore, age-related increases in sub-clinical cardiac abnormalities and reduced renal function may elevate NT-proBNP levels [5]. Therefore, an elevated NT-proBNP level alone is insufficient to predict mortality, and additional tools are needed to refine risk stratification.
High sensitivity C-reactive protein (hsCRP) is an acute-phase protein and an exquisitely sensitive systemic marker of inflammation or tissue damage with broad clinical monitoring utility. hsCRP has attracted interest as a prognostic marker in ACS because of the recognition that atherosclerosis is an inflammatory disease [6]. In addition, an elevated hsCRP level has been associated with adverse outcomes in patients with ACS [7] or chronic HF [8].
Fatty acid binding proteins (FABPs) are small soluble non-enzyme proteins (14-15 kDa) composed of 132 amino acids. FABPs are involved in the intracellular transport of long-chain bioactive fatty acids [9], and are one of the most abundant proteins in the heart, comprising 5-15% of the total cytosolic protein pool. Heart-type FABP (H-FABP) exists in high concentrations in the heart, but is not cardiac specific and occurs in other tissues, albeit at much lower concentrations [10]. Because it is small, H-FABP is secreted from injured cells during the early phase of damage [11]. In fact, H-FABP has been evaluated as an early biomarker for cardiovascular disease and as a prognostic indicator of adverse cardiac events [121314]. However, the relationship between serum H-FABP concentrations and outcomes has not been fully evaluated in patients with other diseases.
In this study, we assessed the prognostic value of combined measurement of acute reactant markers (H-FABP and hsCRP) with NT-proBNP in patients with ACS, non-ACS, and infection. We compared the sensitivity, specificity, and area under the ROC curve (AUC) with those of H-FABP, hsCRP, and NT-proBNP in patients with elevated NT-proBNP.
METHODS
1. Patient selection
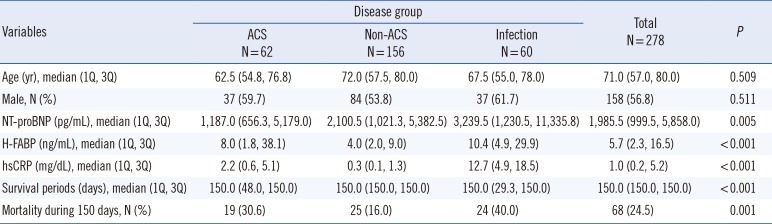
Two hundred seventy-eight patients with an increased serum NT-proBNP level that were admitted to, or visited, the outpatient clinic at Gachon University Gil Medical Center, Korea, during one month (January 2013), were enrolled. This study was approved by our institutional review board (GCIRB2013-23), and the requirement of informed consent was exempt according to the institutional review board. The clinical characteristics of the 278 patients are summarized in Table 1. We classified patients with an increased serum NT-proBNP level into three groups by etiology: 1) ACS and cardiac arrest (ACS group; n=62), 2) non-ACS cardiac disease (non-ACS group; n=156), and 3) infection and sepsis (infection group; n=60). The non-ACS group consisted of the regular follow-up of 156 patients with known cardiac disease (n=57), combined non-ACS diseases (n=42), HF (n=33), arrhythmia (n=10), valvular disease (n=9), aortic dissection (n=3), and cardiomyopathy (n=2).
2. Determinations of serum NT-proBNP, H-FABP, and hsCRP levels
H-FABP (HiSens h-FABP LTIA, HBI, Anyang, Korea) and hsCRP (Siemens Diagnostics, Tarrytown, NY, USA) levels were measured by using an immunoturbidimetric assay (Advia 2400 analyzer, Siemens Diagnostics). Serum levels of NT-proBNP were measured by using an electrochemiluminescence immunoassay on a Cobas e411 analyzer (Roche Diagnostics, Mannheim, Germany).
3. Clinical assessments
All 278 patients were followed up for 150 days post-enrollment. The study endpoint was a composite of death and survival, and was determined on study days 1, 7, 14, 21, 28, 60, 90, 120, and 150.
4. Statistical analyses
Data were analyzed by using SPSS version 17.0 software (IBM, Chicago, IL, USA). Baseline characteristics were assessed by using Kruskal Wallis test for continuous values and Fisher's exact test for categorical values. P values of <0.05 were deemed significant.
Correlation coefficients (adjusted by age and disease group) between markers and survival time were evaluated by partial correlation analysis. The correlation coefficient (r) can range from -1 to +1, with -1 indication a perfect negative correlation, +1 indicating a perfect positive correlation, and 0 indicating no correlation at all. If the r was analyzed to positive value, we could conclude positive correlation between two values. Reference ranges according to age were different in detecting NT-proBNP, and age was analyzed as a confounding factor.
The accuracies of NT-proBNP, H-FABP, and hsCRP for mortality prediction were assessed by ROC curve analysis, which was performed by using the Youden index J. This index is the point on the ROC curve furthest from the line of equality (diagonal line) and can be used to distinguish between non-informative (AUC=0.5), less accurate (0.5<AUC≤0.7), moderately accurate (0.7<AUC≤0.9), highly accurate (0.9<AUC<1), and perfect tests (AUC=1). Comparisons between AUC values of the markers were assessed by using MedCalc statistical software version 12.7.2 (MedCalc Software, Ostend, Belgium) using the method devised by DeLong et al [15].
The cumulative survival curves of NT-proBNP, H-FABP, and hsCRP levels were computed by using the Kaplan-Meier method and MedCalc software. Cox proportional hazard analysis was performed to determine the prognostic significance of NT-proBNP, H-FABP, and hsCRP, and disease groups were used as variables. Hazard ratios (HR) were adjusted by age.
RESULTS
H-FABP (P<0.001), NT-proBNP (P=0.005), and hsCRP (P<0.001) levels, survival period (P<0.001), and 150 day mortality (P=0.001) were statistically different between the three disease groups (Table 1). A significant difference in the median NT-proBNP levels was found in three disease groups (ACS group: 1,187.0 pg/mL, non-ACS group: 2,100.5 pg/mL, and infection groups: 3,239.5 pg/mL, P=0.005). A significant difference in the median H-FABP levels was also observed in disease groups (ACS group: 8.0 ng/mL, non-ACS group: 4.0 ng/mL, and infection group: 10.4 ng/mL). The median hsCRP level was also significantly different among the three groups (ACS group: 2.2 mg/dL, non-ACS group: 0.3 mg/dL, and infection group: 12.7 mg/dL).
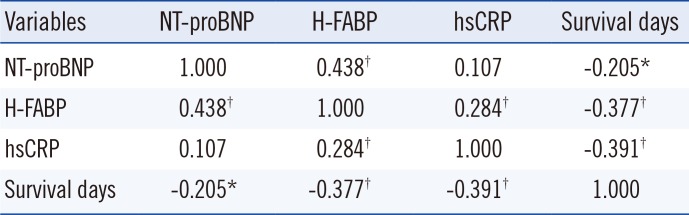
In the correlation analysis among the markers, Pearson's correlation coefficient (r) was 0.438 between NT-proBNP and H-FABP (P<0.001), 0.107 between NT-proBNP and hsCRP (P=0.075), and 0.284 between H-FABP and hsCRP (P<0.001). NT-proBNP (r=-0.205, P=0.001), H-FABP (r=-0.377, P<0.001), and hsCRP (r=-0.391, P<0.001) showed negative correlations between survival and elevated markers (Table 2).
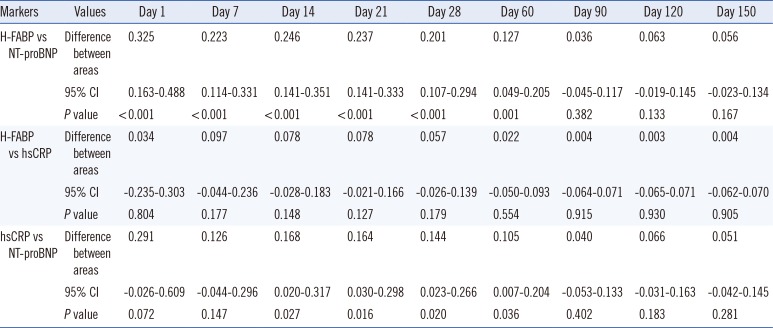
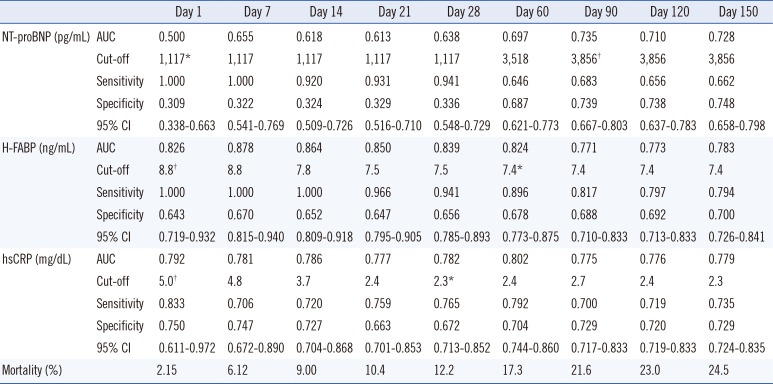
Because AUC is a measure of overall test performance, the prognostic performance of different markers can be assessed by comparing their AUCs. AUCs of the three markers in the 278 patients showed differences during the 60-day follow-up period. H-FABP was superior to NT-proBNP for predicting mortality in patients with an increased NT-proBNP level (Table 3, P≤0.001), whereas hsCRP was better than NT-proBNP as a prognostic marker of mortality from day 14 to 60 (Table 3, P=0.016-0.036).
In the 278 patients, the sensitivity, specificity, cut-off concentration, and prognostic efficiency of NT-proBNP, H-FABP, and hsCRP were analyzed by ROC curve analysis on days 1, 7, 14, 21, 28, 60, 90, 120, and 150 after enrollment. Patients were divided into three classes by marker concentration. Marker levels were determined to be the minimum and maximum values for discriminating mortality based on optimal cut-off values of the AUC in the NT-proBNP level (<1,117 pg/mL, ≥1,117 pg/mL<3,856 pg/mL, ≥3,856 pg/mL), H-FABP level (<7.4 ng/mL, ≥7.4 ng/mL<8.8 ng/mL, ≥8.8 ng/mL), and hsCRP level (<2.3 mg/dL, ≥2.3 mg/dL<5.0 mg/dL, ≥5.0 mg/dL) (Table 4). The AUC for H-FABP was larger than that of NT-proBNP or hsCRP until 60 days after sampling (Table 4).
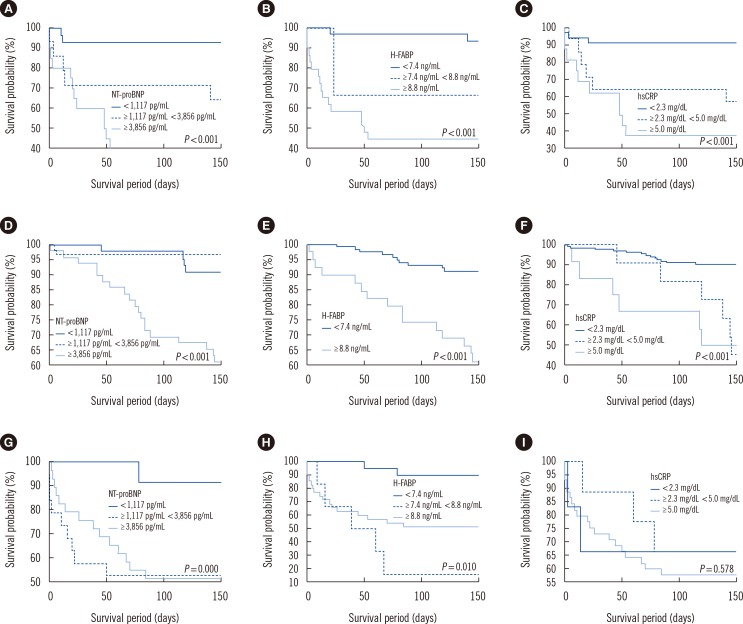
Kaplan-Meier curves showed that the elevated serum NT-proBNP and H-FABP levels were prognostic markers of mortality over 150 days in each disease group (Fig. 1), and mortality rates increased in proportion to NT-proBNP (Fig. 1A, D, G) and H-FABP levels (Fig. 1B, E, H). However, an elevated hsCRP level only affected mortality in the cardiac disease groups (Fig. 1C, F) over 150 days, and the mortality rate increased in proportion to the hsCRP level.
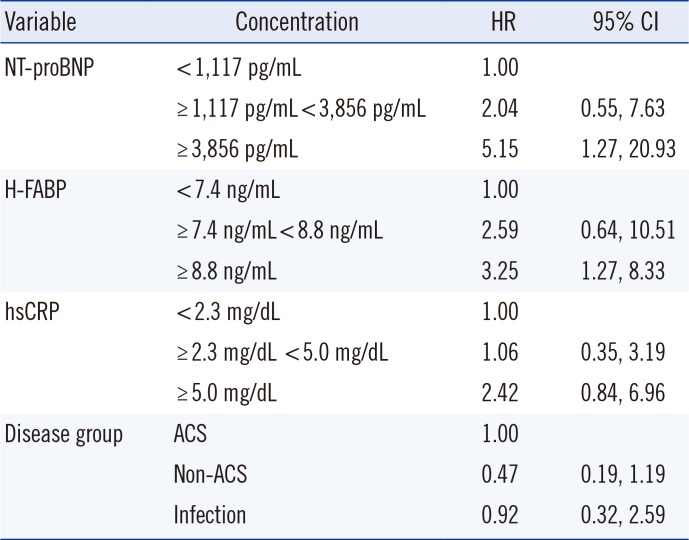
By multivariate Cox proportional hazards regression analysis adjusted for age, patients with an H-FABP of ≥8.8 ng/mL had a 3.25-fold increased risk of death as compared with patients in the reference group (<7.4 ng/mL) during the 150 day follow-up period (95% confidence interval [CI]: 1.27-8.33, Table 5). For NT-proBNP, patients with levels ≥3,856 pg/mL had a higher risk of death than the reference group (HR: 5.15; 95% CI: 1.27-20.93, Table 5). The concentration of hsCRP did not increase the risk of death compared with the reference group.
DISCUSSION
In this study, the usefulness of H-FABP and hsCRP serum levels, in combination with NT-proBNP serum levels, was investigated for risk stratification in patients with ACS, non-ACS, and infectious disease. In the 278 patients examined, concentrations of NT-proBNP and H-FABP showed positive correlations (r=0.438, P<0.001), and H-FABP was a superior marker to predict mortality than NT-proBNP. NT-proBNP and hsCRP did not show a statistical correlation; however, hsCRP was a superior prognostic marker than NT-proBNP. Concentrations of H-FABP and hsCRP were also positively correlated (r=0.284, P<0.001), but there was no significant difference in predicting mortality (Tables 3 and 4).
The AUCs of H-FABP were larger for all patients (0.824-0.878) at days 1, 7, 14, 21, 28, and 60 after enrollment than those of hsCRP (0.777-0.792) or NT-proBNP (0.500-0.697). H-FABP was a powerful marker of short-term mortality (until day 60), and the difference between the prognostic efficacies of H-FABP and NT-proBNP was remarkable in all patients. These findings indicate that H-FABP has a good prognostic accuracy for predicting mortality within 60 days. The result of survival analysis using the above-described cut-off levels showed that H-FABP levels were positively correlated with mortality in all three patient groups. Patients with an H-FABP level ≥8.8 ng/mL had a 3.25-fold increased risk of death as compared with patients in the reference group (<7.4 ng/mL) during the follow-up period (95% CI: 1.27-8.33, Table 5). These findings are concordant with those of others. For example, Viswanathan et al [16] reported an association between elevated H-FABP and the risks of 12-month mortality and myocardial re-infarction in 966 patients with suspected ACS, and Jo et al [17] found that H-FABP was an independent prognostic marker for predicting 28-day mortality in patients with severe sepsis and septic shock [17].
Among patients with elevated NT-proBNP, H-FABP, and hsCRP levels, there was a correlation with increased mortality in different disease groups (Fig. 1), except for hsCRP in the infection group. Regarding mortality prediction, hsCRP was useful in the ACS and non-ACS cardiac disease groups, but could not predict mortality in the infection group. In previous reports, increased serum concentrations of hsCRP were well correlated with functional limitations and prognosis in patients with cardiovascular diseases [781819]. However, some major studies found a poor correlation between hsCRP and mortality in patients with infection or sepsis [20]. Muller et al [21] and Kruger et al [22], in studies of community-acquired pneumonia, found that hsCRP levels were not a useful marker for predicting the clinical severity of pneumonia.
In the present study, in patients with an elevated NT-proBNP level, increases in serum H-FABP levels were identified as an independent predictor of short-term mortality (within 60 days), and correlated with mortality in three disease groups. Patients with H-FABP levels ≥8.8 ng/mL had a 3.25-fold increased risk of death as compared with patients in the reference group (<7.4 ng/mL) after adjusting for the age effect. Therefore, clinicians can estimate that patients with elevated levels of NT-proBNP and H-FABP, who have cardiac or infectious disease at admission or when visiting an outpatient clinic, had a higher risk of mortality than patients with lower levels had. Thus, it appears this simple evaluation using a combination of biomarkers would help clinicians devise risk stratification for mortality.
The limitation of this study was that blood samples were not obtained serially from time of symptom onset. Thus, we were unable to examine relationships between the three marker levels and disease status.
In conclusion, the combined measurement of H-FABP with NT-proBNP provides a highly reliable means of short-term mortality prediction for patients hospitalized for ACS, a non-ACS cardiac disease, or infectious disease.
 XML Download
XML Download