

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
On May 20, 2015, Middle East respiratory syndrome coronavirus (MERS-CoV) was confirmed for the first time in an infected patient in the Republic of Korea. Although the primary case traveled to the United Arab Emirates and Saudi Arabia, the patient did not initially report his recent travel in those countries [1]. This case led to transmission of MERS-CoV both within a hospital and between hospitals and eventually resulted in the largest outbreak of MERS-CoV infections outside the Arabian Peninsula.
At that time, we had limited information on MERS-CoV, and only a few clinical laboratories were prepared to perform molecular diagnostic testing for the virus. During the longer than two months of the outbreak, 186 confirmed cases were diagnosed by real-time reverse transcription PCR (rRT-PCR) of MERS-CoV, and specimens from tens of thousands of suspected cases, including individuals who contacted the confirmed cases, were submitted for this testing. Many clinical laboratories were instructed to set up facilities to perform MERS-CoV rRT-PCR on site in a short time to fight against the transmission of this virus in their own institutes.
An earlier outbreak in 2009 of a novel strain of H1N1 influenza virus A (H1N1 influenza) affected laboratories worldwide, with a potentially tremendous impact on the practices of clinical laboratories [2]. The outbreak of H1N1 influenza also had a great influence in the Republic of Korea. The field of molecular testing for pathogens has been expanded in clinical laboratories, and the molecular testing industry has responded quickly with the production of new molecular test kits. Numerous studies, including viral etiology, epidemiology, risk factors, clinical and laboratory characteristics, and diagnostic tests, have been reported [3]. Despite the fact that clinical laboratory practice was a critical element in the response to the H1N1 influenza outbreak, there are only a few reports regarding this aspect of testing [245].
The ability of clinical laboratories to respond appropriately to an outbreak is significant in pathogen control. Therefore, it is crucial to understand the current status of clinical laboratories in the Republic of Korea in order to be well prepared for any future emerging infectious diseases. In this article, we present the results of a survey of clinical laboratory practices during the 2015 MERS-CoV outbreak.
Go to : 
METHODS
The study population consisted of clinical laboratories performing diagnostic testing for MERS-CoV in medical institutions (hospitals and medical centers) and referral medical laboratories among clinical laboratories accredited by the Korean Laboratory Accreditation Program [6].
This survey was an initiative of the MERS-CoV Laboratory Response Task Force of the Korean Society for Laboratory Medicine. We conducted a survey of 49 clinical laboratories. A short questionnaire to assess clinical laboratory practices related to MERS-CoV diagnostic testing was sent by email to the directors and the clinical pathologists (laboratory physicians) in charge of the clinical laboratories performing MERS-CoV tests. The survey focused on the number of tests and the number of positive test results for MERS-CoV, turnaround time (TAT), request process, collection and transportation of specimens, testing and reporting, communication of results, laboratory safety, and reagents and equipment.
Go to :
RESULTS
A total of 40 clinical laboratories (81.6%, 40/49), including 35 medical institutions and 5 referral medical laboratories, responded to the survey. The number of beds in the medical institutions was as follows: <500 beds, 3 institutions (8.6%); 500-1,000 beds, 20 (57.1%); and >1,000 beds, 12 (34.3%). All clinical laboratories used rRT-PCR as the detection method for MERS-CoV.
1. Testing volume and specimen type
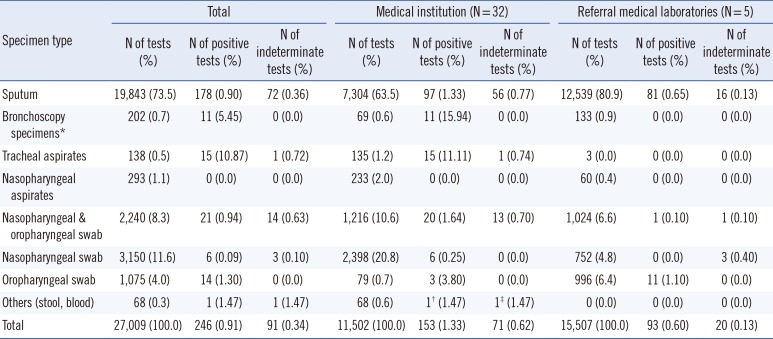
The number of MERS-CoV rRT-PCR tests performed was collected from 32 medical institutions and five referral medical laboratories. Data up to July 15, 2015 were collected according to the day and specimen type. A total of 27,009 MERS-CoV rRT-PCR tests were performed at 32 medical institutions (N=11,502) and five referral medical laboratories (N=15,507) (Table 1 and Fig. 1). The proportion of medical institutions was significantly underestimated because one tertiary care hospital submitted responses for the survey but not the specimen list, and the numbers of MERS-CoV rRT-PCR tests and positive specimens at this institution would have been predominant in the reporting medical institutions. MERS-CoV rRT-PCR testing at all medical institutions and referral medical laboratories increased dramatically in early June (Fig. 1). The number of clinical laboratories that initiated MERS-CoV testing increased in the first two to three weeks (Fig. 2). Daily test volumes peaked on June 24 (1,088 tests) and began to decrease thereafter (Fig. 1). Among the 27,009 MERS-CoV rRT-PCR specimens, 246 (0.9%) and 91 (0.3%) specimens were positive and indeterminate, respectively (153 and 71 specimens at medical institutions, 93 and 20 specimens at referral medical laboratories; Table 1).
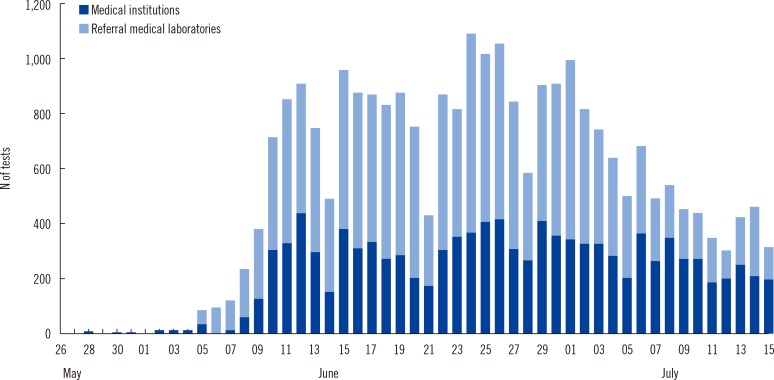 | Fig. 1Number of Middle East respiratory syndrome coronavirus (MERS-CoV) tests performed in Korea from May 28 to July 15.
|
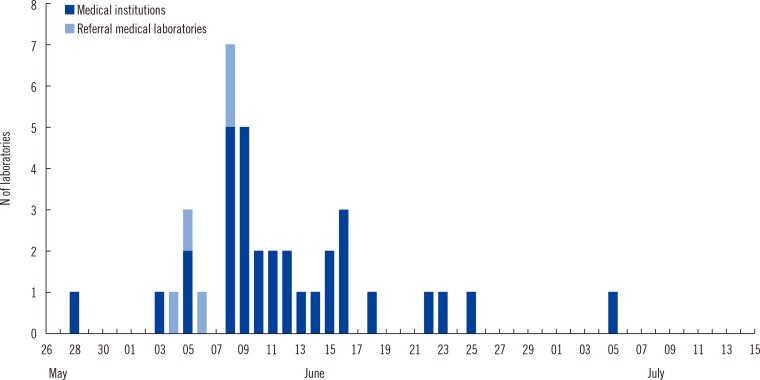 | Fig. 2Number of clinical laboratories that started Middle East respiratory syndrome coronavirus (MERS-CoV) testing in Korea from May 28 to July 15.
|
Table 1
Number of MERS-CoV tests and positive and indeterminate results according to the specimen type
![]()
Most of the specimens for MERS-CoV rRT-PCR were sputum (73.5%). A total of 74.7% of all specimens tested and 82.9% of positive specimens were specimens from the lower respiratory tract, such as sputum, bronchoscopy specimens, or tracheal aspirates (Table 1). All nasopharyngeal aspirates (N=293) were negative for MERS-CoV rRT-PCR.
2. Turnaround time
The TAT is defined as the time from the receipt of specimens in the laboratory to the reporting of the results. Unfortunately, 35% of the laboratories (nine medical institutions and five referral medical laboratories) were not able to provide or analyze data on TAT.
The median TAT was 5.29 hr (first and third quartile, 4.11 and 7.48 hr) for 26 medical institutions, and the minimum and maximum median TAT (first and third quartile) were 4.00 hr (3.35 and 5.10 hr) and 26.46 hr (19.59 and 31.36 hr), respectively. The median TAT of more than a half of the laboratories (57.7%) was less than 6 hr. The results were reported within 24 hr in all medical institutions except one (Table 2).
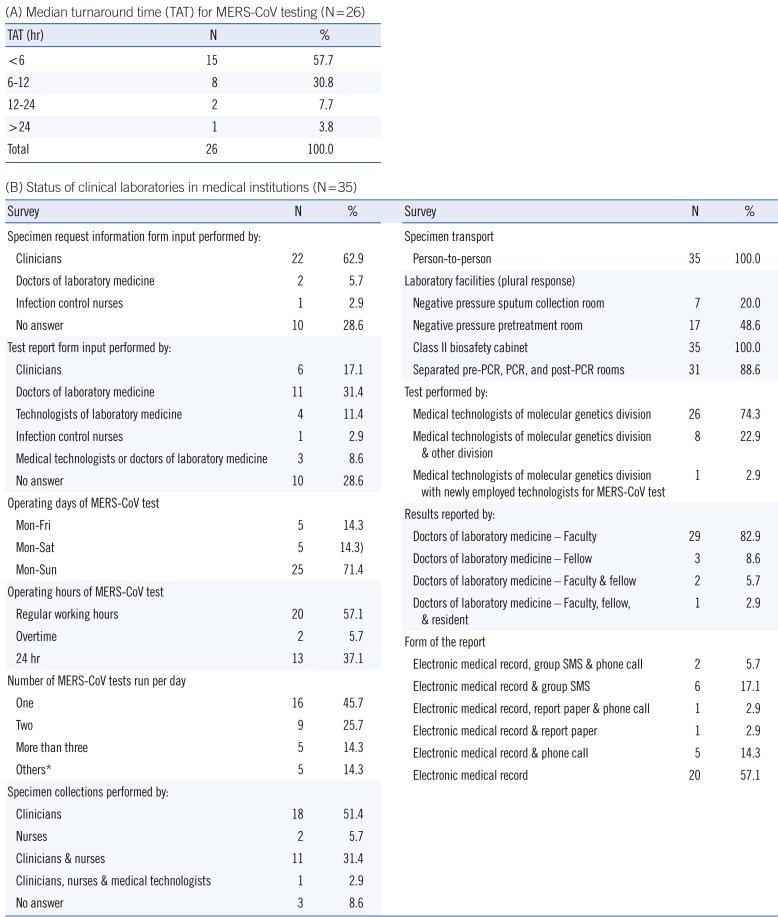
Table 2
Turnaround time and status of clinical laboratories in medical institutions
| (A) Median turnaround time (TAT) for MERS-CoV testing (N=26) | ||
|---|---|---|
| TAT (hr) | N | % |
| <6 | 15 | 57.7 |
| 6-12 | 8 | 30.8 |
| 12-24 | 2 | 7.7 |
| >24 | 1 | 3.8 |
| Total | 26 | 100.0 |
![]()
In the referral medical laboratories, the results were reported in less than 6-9 hr (during weekday daytime) or 9-15 hr (during weekday nights and weekends).
3. Status of clinical laboratory operation
Table 2 shows the current status of clinical laboratories in medical institutions with respect to their response to the outbreak of MERS-CoV infections. Many laboratories were able to perform testing throughout the week (71.4%, 25/35) and ran tests once or twice per day. Specimen was collected mainly by clinicians, and all specimens were directly transported person-to-person. In most cases, clinicians filled out the specimen request information form, and doctors of laboratory medicine completed the test report form. Most of the MERS-CoV rRT-PCR tests were performed only by clinical laboratory technicians of molecular genetics divisions (74.3% of 35 laboratories). The test results were primarily reported by clinical pathologists via electronic processing. Laboratory biosafety preparedness in response to the MERS-CoV outbreak included class II biosafety cabinets (100%, 35/35); separated pre-PCR, PCR, and post-PCR rooms (88.6%, 31/35); negative pressure pretreatment rooms (48.6%, 17/35); and negative pressure sputum collection rooms (20.0%, 7/35).
As shown in Table 3, the current status of clinical laboratories in referral medical laboratories was similar to that of medical institutions in many aspects. Specimens were transported twice or three times a day.
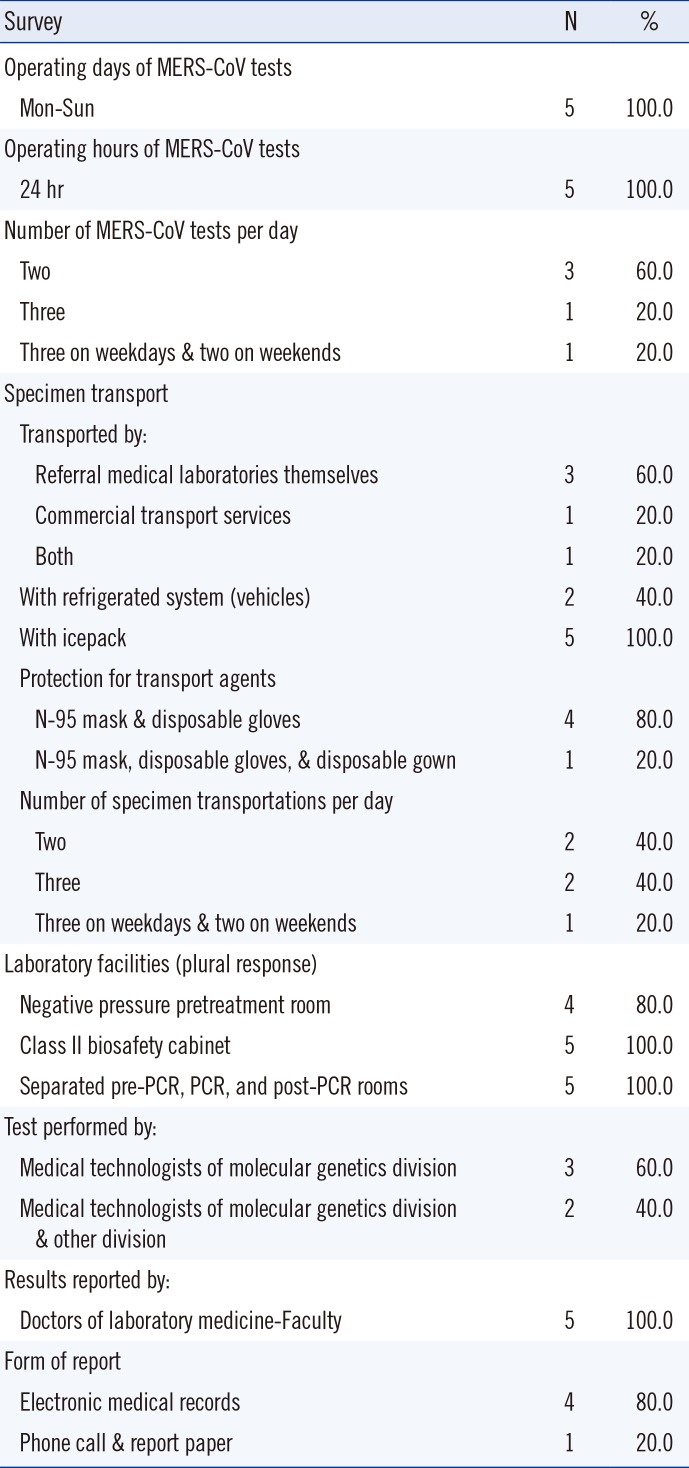
Table 3
Status of clinical laboratories in referral medical laboratories (N=5)
![]()
4. Pretreatment of specimens, reagents, and equipment
Many laboratories (75%, 30/40) used phosphate-buffered saline for pretreatment of sputum specimens. All reagents for the detection of MERS-CoV were components of ready-made kits, and the PowerChek MERS Real-time PCR Kit (KogeneBiotech, Seoul, Korea) was the most commonly used kit (72.5%, 29/40). Most laboratories used CFX96 (Bio-Rad Laboratories, Hercules, CA, USA) or ABI7500 or 7800 systems (Life Technologies, Carlsbad, CA, USA) for rRT-PCR (85.0%, 34/40) (Table 4).

Table 4
Pretreatment, reagents, and equipment for MERS-CoV testing in 2015 outbreak in Korea
Abbreviations: MERS-CoV, Middle East respiratory syndrome coronavirus; PBS, phosphate-buffered saline; NALC, N-acetyl L-cysteine; DW, deionized water; KogeneBiotech, KogeneBiotech PowerChek MERS-CoV real-time PCR kit; SolGent, SolGent DiaPlexQ MERS-CoV virus detection kit; Bioneer, Bioneer AccuPower MERS-CoV real-time RT-PCR kit; NANOBIOSYS, NANOBIOSYS MERS-CoV corona virus detection kit; BIO-RAD CFX96, BIO-RAD CFX96 real-time PCR system; ABI7500 or 7500 Fast, Life Technologies ABI7500 or 7800 real-time PCR system; Bioneer Exicycler, Bioneer Exicycler 96 real-time PCR system; LG SLAN, LG Life Sciences SLAN real-time PCR system; NANOBIOSYS G2-4, NANOBIOSYS real-time PCR G2-4.
![]()
Go to :
DISCUSSION
The emergence of novel viral pathogens and the evolution of pandemics have presented a new and complex challenge to public health care systems at every level [1378]. The outbreak of H1N1 influenza eventually turned out to be relatively mild, despite the fear it engendered as the potential early stage of a pandemic. Breban et al. [9] suggested that MERS-CoV does not yet have pandemic potential. Nevertheless a MERS-CoV outbreak recently occurred in the Republic of Korea, and its characteristics were very different from those of the outbreak of H1N1 influenza. The MERS-CoV outbreak was more serious than expected, and numerous problems arose concerning infection control and prevention in hospitals and among the general public.
Because clinical laboratories are usually on the front lines for the detection of emerging pathogens, the ability of these laboratories to respond to an outbreak is critical for infection control and prevention. The elements of clinical laboratory preparedness and responsiveness include availability of personal protective equipment and its appropriate use, availability and use of appropriate testing supplies, adequacy of staffing, and infrastructure requirements including laboratory space [2]. In 2012 and 2013, the European Centre for Disease Prevention and Control (ECDC) and the WHO Regional Office for Europe conducted a joint survey [10]. Although the number of countries that had laboratory capabilities to detect and confirm MERS-CoV increased in 2013 (55.8%, 29 of 52 countries) compared with 2012 (47.8%, 22 of 46 countries), a half of the countries were still unable to test MERS-CoV [10].
The present study reveals a snapshot of the current status and capability of clinical laboratories to respond to the MERS-CoV outbreak in the Republic of Korea. Most clinical laboratories participating in the survey were considered to have sufficient capacity to respond to the outbreak. Immediately after the MERS-CoV rRT-PCR test was approved, many laboratories were able to perform testing seven days a week and the number of tests reported increased dramatically. The median TAT of more than a half of the laboratories (57.7%) was shorter than 6 hr, and the minimum median TAT was 4.00 hr. The results were reported within 24 hr in all medical institutions except one. One limitation of our study is that even though we obtained responses from the majority of medical institutions and referral medical laboratories, the results may not be fully representative for a number of reasons. Data were collected before the end of the MERS-CoV outbreak and did not include some major medical institutions and public health laboratories such as the Korea Centers for Disease Control and Prevention. In addition, our results report the number of MERS-CoV rRT-PCR tests, and not the number of MERS-CoV cases.
Previously, Sousa et al. [11] suggested that the use of upper respiratory specimens (e.g., nasopharyngeal swabs) for MERS-CoV diagnosis might not be as sensitive as the use of lower respiratory tract specimens. The laboratory diagnostic guidelines for MERS-CoV testing of the Korean Society for Laboratory Medicine recommended using specimens from the lower respiratory tract. In the present survey, the number of positive results from MERS-CoV rRT-PCR was significantly higher in specimens obtained from the lower respiratory tract (1.01%, 204/20,183) compared with specimens from the upper respiratory tract (0.6%, 41/6,785) (P=0.002, chi-square test). Therefore, the specimen type is expected to have a significant impact on diagnostic sensitivity and should be considered when testing emerging pathogens.
For laboratory biosafety in response to the MERS-CoV outbreak, class II biosafety cabinets were adequately supplied but high-end engineering facilities such as negative pressure sputum collection and pretreatment rooms were not readily available. However, no laboratory-acquired infections were reported during the outbreak, thus standard precautions with droplet precautions appeared to be sufficient for the prevention of laboratory-acquired infection of MERS-CoV. Nonetheless, improvements in engineering laboratory biosafety are needed for preparedness to test agents with a higher biosafety level.
Clinical laboratories have the primary responsibility for testing specimens to support clinical decision-making. Although public health laboratories also test specimens to aid clinical decisions, their roles in surveillance, strain identification, and tracking of drug resistance are arguably their main priorities [12]. Moreover, clinical laboratories often have resources available that allow for rapid expansion [12]. In conclusion, the results of this survey contribute to the comprehensive view of clinical laboratory response in the Republic of Korea to the recent outbreak of 2015 MERS-CoV. On the basis of currently available data, clinical laboratories in Korea were able to expand their diagnostic capacity in a short time and achieve a TAT of shorter than nine hours with testing seven days per week to response to the recent MERS-CoV outbreak, although the delay in the early period of the outbreak should be improved. Therefore, clinical laboratories should be ready for the maintenance and enhancement of laboratory responses in preparation for future emerging infections.
Go to :
 XML Download
XML Download