

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Glucose nonfermentative gram-negative bacilli (GNFB) such as Pseudomonas aeruginosa and Acinetobacter baumannii are opportunistic pathogens that cause infections mainly in hospitalized patients, especially in patients in intensive care units [12]. Most GNFB are naturally resistant to many antimicrobial agents and also acquire antimicrobial resistance easily. Therefore, GNFB infections are difficult to treat.
Carbapenem is the only available drug for treating GNFB infections in many cases. However, the recent increase of carbapenem resistance in GNFB has become a serious problem worldwide, particularly in Korea [3]. Most carbapenem-resistant P. aeruginosa and A. baumannii strains identified in Korea are also extensively drug-resistant (XDR) [4]. Few treatment options are currently available for treating infections caused by these notorious pathogens. Colistin (CL) and polymyxin B can be used for treating infections caused by XDR P. aeruginosa and A. baumannii; however, these drugs are associated with severe side effects, including nephrotoxicity and neurotoxicity [5]. Moreover, identification of appropriate therapeutic concentrations of these drugs in the blood is difficult [67]. Tigecycline is another promising antibiotic [8]. However, it cannot be used for treating P. aeruginosa infections due to natural resistance [9]. Furthermore, some researchers have reported the emergence of tigecycline-resistant A. baumannii in some countries [1011]. One classical treatment method often used for treating infections caused by multi-drug resistant (MDR) pathogens is administration of combinations of several antibiotics [12131415]. Some evidence suggests that these combinations are effective for treating infections caused by XDR GNFB.
In this study, we determined the extent of synergistic effects exerted by antimicrobial combinations on XDR P. aeruginosa and A. baumannii isolates collected from hospitals in Korea.
Go to : 
METHODS
In all, 77 XDR GNFB isolates (43 P. aeruginosa and 34 A. baumannii isolates), which were resistant to all tested antibiotics, except CL, were collected from eight university hospitals in Korea in 2007. Antimicrobial susceptibilities of these isolates were initially tested at each hospital by using CLSI disk diffusion method or Vitek 2 system (bioMerieux, Marcy l'Etoile, France).
The species of each isolate was determined at a coordinating laboratory, and minimum inhibitory concentration (MIC) of each antibiotic (piperacillin, piperacillin-tazobactam, ampicillin-sulbactam [AMS], cefotaxime, ceftazidime [CAZ], cefepime, aztreonam, imipenem [IPM], meropenem, gentamicin, amikacin, ciprofloxacin, trimethoprim-sulfamethoxazole, and CL) was determined by using CLSI agar dilution method [16].
The ability of each isolate to produce carbapenemases and metallo-β-lactamases (MBLs) was screened by Hodge test [17] and IPM-EDTA sodium mercaptoacetic acid double-disk synergy test [18], respectively. Results of these tests were confirmed by PCR to determine the presence of blaVIM, blaIMP, blaSIM, and blaOXA (blaOXA-23, blaOXA-24, blaOXA-51, and blaOXA-58) [19]. DNA was extracted from whole-cell lysates by boiling bacterial colonies. Amplification was performed in a 20-µL reaction mixture containing 1-µL heat-extracted DNA template, 10 pmol of each primer, and PreMix (Bioneer, Cheongwon, Korea) containing 1 U Taq DNA polymerase. Sizes of amplified products were confirmed by performing electrophoresis, and each confirmed amplified product was sequenced twice by using an automatic sequencer (model 3730xl; Applied Biosystems, Weiterstadt, Germany).
Checkerboard method was used to determine the degree of in vitro synergistic effects exerted by antimicrobial combinations used on 30 randomly selected isolates of XDR P. aeruginosa and A. baumannii each [20]. Antimicrobial combinations tested were IPM and CL, rifampin (RIF) and CL, and CAZ and CL for P. aeruginosa and IPM and CL, IPM and AMS, IPM and RIF, and RIF and CL for A. baumannii. Fractional inhibitory concentration index (FICI) was calculated by using the following formulae:
FICI were interpreted as follows: ≤0.5, synergistic effect; 0.5-4, additive/indifferent effect; and ≥4, antagonistic effect. Escherichia coli (ATCC 25922) and P. aeruginosa (ATCC 27853) strains were used for quality control.
Go to :
RESULTS
None of the XDR GNFB isolates examined was susceptible to any of the tested antibiotic, except CL. The MICs of β-lactams, aminoglycosides, and fluoroquinolones were very high for majority of XDR P. aeruginosa and A. baumannii isolates (Table 1). However, 38% (3/8) of MBL-producing P. aeruginosa isolates were intermediately sensitive to aztreonam and 86% (6/7) of OXA-23-negative A. baumannii isolates were intermediately sensitive to IPM.
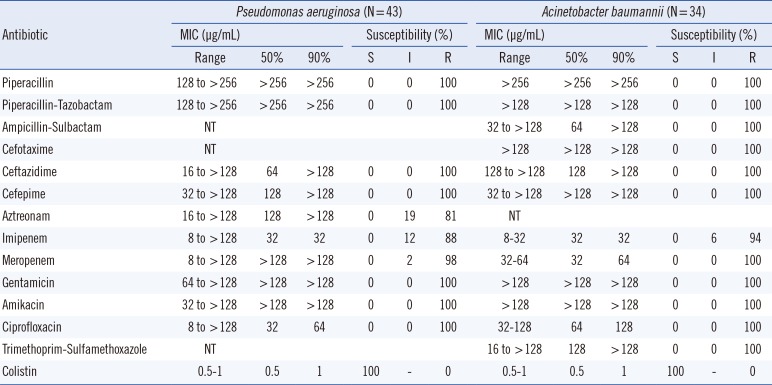
Table 1
Antimicrobial susceptibilities of extensively drug-resistant P. aeruginosa and A. baumannii isolates
![]()
Of the 43 XDR P. aeruginosa isolates, four were IMP-1- and VIM-2-producing isolates. Of the 34 XDR A. baumannii isolates, two were IMP-1-, VIM-2-, and SIM-1-producing isolates. Most MBL-negative XDR A. baumannii isolates yielded positive results for blaOXA-23 (82%), and all the A. baumannii isolates yielded positive results for blaOXA-51.
In the synergy test, FICI values for the antimicrobial combinations used could not be calculated for three P. aeruginosa isolates and five A. baumannii isolates because their MICs exceeded the expected values. Three antimicrobial combinations exerted only additive/indifferent effects on all XDR P. aeruginosa isolates irrespective of their MBL production status (Table 2). Proportions of XDR A. baumannii isolates that showed synergistic and additive/indifferent inhibition after treatment with the antimicrobial combinations used are as follows: IPM-AMS, 17% and 80% isolates, respectively; IPM-RIF, 13% and 81% isolates, respectively; IPM-CL, 13% and 87% isolates, respectively; and RIF-CL, 20% and 73% isolates, respectively (Table 3). Most A. baumannii isolates that showed synergistic inhibition produced MBLs. The extent of decrease of MICs in A. baumannii isolates ranged from one quarter to one sixteenths (FICI, 0.25-5). MICs of most antimicrobial concentrations tested decreased from high-level resistance range to susceptible and intermediate range (Table 4). None of the tested combinations exerted antagonistic effects.
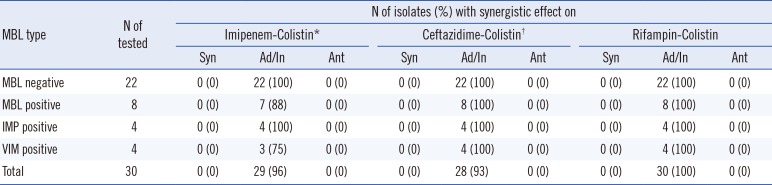
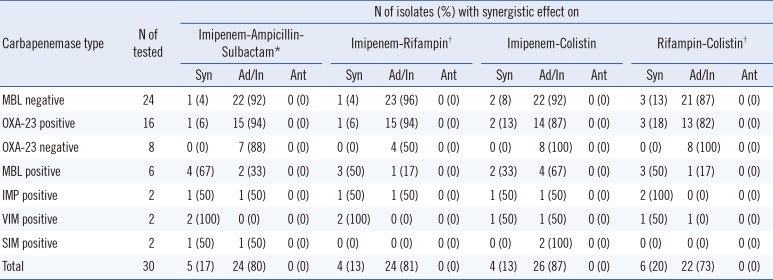
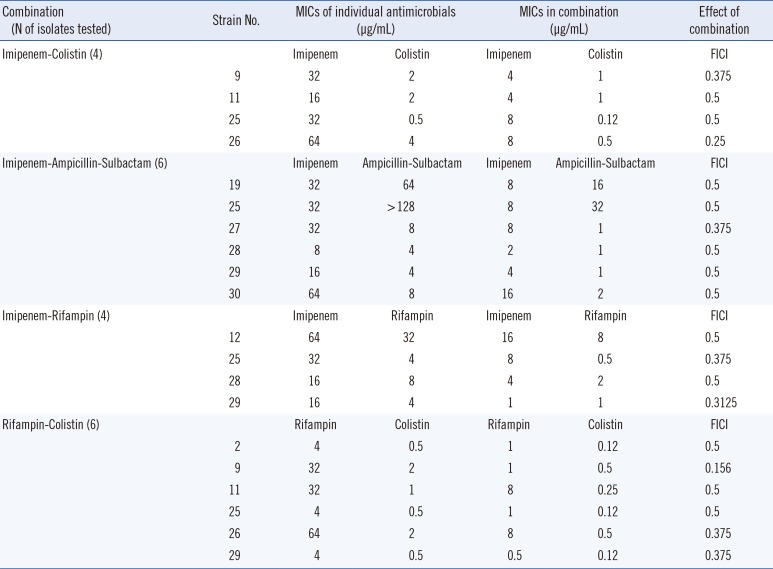
Table 2
Effects of antimicrobial combinations on extensively drug-resistant P. aeruginosa isolates
*FICI value of one strain in the VIM-positive group could not be calculated; †FICI values of two strains in the MBL-negative group could not be calculated.
Abbreviations: FICI, fractional inhibitory concentration index; Syn, synergistic (FICI, ≤0.5); Ad/In, additive/indifferent (FICI, 0.5-4); Ant, antagonistic (FICI, ≥4); MBL, metallo-β-lactamase.
![]()
Table 3
Effects of antimicrobial combinations on extensively drug-resistant A. baumannii isolates
*FICI value of one isolate in OXA-23-positive group could not be calculated; †FICI values of two isolates in SIM-positive group could not be calculated.
Abbreviations: FICI, fractional inhibitory concentration index; Syn, synergistic (FICI, ≤0.5); Ad/In, additive/indifferent (FICI, 0.5-4); Ant, antagonistic (FICI, ≥4); MBL, metallo-β-lactamase.
![]()
Table 4
Concentrations of antibiotic combinations that exerted synergistic effects on extensively drug-resistant A. baumannii isolates
![]()
Go to :
DISCUSSION
The recent increase in XDR GNFB infections in health-care settings has threatened public health in many countries. In Korea, the recent rates of carbapenem resistance are moderate to high for P. aeruginosa and A. baumannii. Moreover, MDR and XDR P. aeruginosa and A. baumannii isolates are commonly identified in Korea. Carbapenem resistance can result from enzyme production, porin loss, and active efflux. However, it is difficult to determine the exact mechanisms underlying carbapenem resistance, except enzyme production. Mechanisms underlying carbapenem resistance could not be determined for most P. aeruginosa isolates, except eight (19%) MBL-producing isolates (Table 2). Porin loss and active efflux might be the reasons for carbapenem resistance in most P. aeruginosa isolates examined in this study. Majority of XDR A. baumannii isolates produced β-lactamases, including MBLs and OXA-23 (Table 3).
Polymyxin B and polymyxin E (CL) are regarded as the last resort for treating infections caused by MDR or XDR gram-negative pathogens because of the recent spread of antibiotic resistance in many gram-negative bacilli even though severe toxicity. Two studies have suggested that polymyxin B and CL are good treatment options because many XDR P. aeruginosa and A. baumannii isolates were susceptible to these drugs [2122], which was consistent with the present results (Table 1). Resistance to polymyxins has been rarely observed recently; however, several mechanisms through which bacteria may acquire resistance to polymyxin B and CL have been proposed [2324]. A study by Matthaiou et al. [25] showed a relationship between inappropriate use of CL and development of resistance in P. aeruginosa and A. baumannii. Furthermore, Kim et al. [26] recently reported that mutations in pmrB could induce in vivo emergence of CL resistance in A. baumannii clinical isolates of sequence type 357. Thus, the threat of increasing resistance to polymyxin B and CL is a problem because these drugs need to undergo susceptibility testing before their use in clinical settings. Moreover, limitation of susceptibility method to these drugs may be problematic in clinical microbiology laboratories [2728]. Treatment with polymyxin B and CL has resulted in frequent nephrotoxicity and neurotoxicity, especially in patients with deteriorated renal function. Therefore, close monitoring and caution are often requested during their use. Combination therapy with antibiotics is often used for treating infections caused by MDR or XDR pathogens [12131415]. Because antimicrobial combinations exerting synergistic effects enable the use of reduced concentrations of individual drugs, such combinations may decrease the possible toxicities associated with high drug concentrations. Polymyxins act primarily on the cell wall by inducing rapid changes in the permeability of the cytoplasmic membrane of gram-negative bacilli, thereby permitting the entry of other antimicrobial agents into the cell. Various antimicrobial agents can be used in combination with CL. Antibiotics that are most frequently combined with CL include β-lactam antibiotics such as carbapenem and RIF. Landman et al. [29] reported that the combination of polymyxin B with IPM or RIF exerted synergistic effects in 80% and 90% cases, respectively, in a time-kill study on P. aeruginosa. In a study by Gunderson et al. [30], the combination of CL with CAZ exerted synergistic effects on two CL-susceptible MDR P. aeruginosa isolates. However, inconsistent results have been obtained by using the combination of carbapenems with CL for treating infections caused by MDR P. aeruginosa. Two studies have found that the combination of CL with meropenem only exerted additive/indifferent effects on MDR P. aeruginosa [3132]. A recent meta-analysis by Zusman et al. [15] involving 39 publications and 15 conference proceedings related to the in vitro examination of the combinations of polymyxins with carbapenems showed that the combination of polymyxins with IPM exerted synergistic effects on 60% P. aeruginosa isolates tested and antagonistic effects on 21% P. aeruginosa isolates tested.
Use of combination therapy can suppress the development of resistance in vitro. In this study, both IPM-CL and CAZ-CL only exerted additive/indifferent effects and did not exert synergistic effects on all XDR P. aeruginosa isolates irrespective of their MBL production status (Table 3). The combination of CL with RIF is generally recommended in regimens for treating infections caused by MDR and XDR gram-negative pathogens. However, the rates of synergy exerted by RIF-CL against different P. aeruginosa isolates ranged from 5.7% (2/35) to 16.6% (1/6) [3133]. Moreover, RIF-CL did not exert synergistic effects on any P. aeruginosa isolate in the present study (Table 2). The reason for this discrepancy is unknown, and further evaluation may be required to completely determine the effect of RIF-CL on various P. aeruginosa isolates.
The combination of sulbactam, which is effective against A. baumannii [34], with IPM exerted a synergistic effect on approximately 17% (5/30) XDR A. baumannii, of which four isolates produced MBLs. RIF exhibits bactericidal activity against A. baumannii
in vitro. A study by Timurkaynak et al. [31] showed that 64% of 25 MDR A. baumannii isolates were susceptible to RIF. Combinations of RIF with β-lactam antibiotics were effective in mouse model of A. baumannii-induced pneumonia [3536]. However, IPM-RIF only exerted a synergistic effect on as low as 13% (4/30) XDR A. baumannii isolates in our study. Many studies have shown that CL monotherapy is effective against MDR and XDR A. baumannii and that CL-RIF exerts synergistic and bactericidal effects [3738]. In this study, the rates of synergy exerted by IPM-RIF and RIF-CL were 13% and 20%, respectively (Table 3).
A study conducted in the UK by Wareham et al. [39] reported that combinations of polymyxin B with IPM, RIF, or azithromycin did not exert any synergistic effect on OXA-23-producing MDR A. baumannii isolates. We also observed that the rates of synergy of antimicrobial combinations were higher in MBL-producing A. baumannii isolates than in MBL-negative A. baumannii isolates (Table 3). However, a recent meta-analysis showed that combinations of polymyxins with IPM exerted synergistic effects on 56% A. baumannii isolates tested [15]. Among the antimicrobial combinations that exerted synergistic effects, MICs of IPM, AMS, and RIF decreased from resistant or intermediate range to susceptible range (Table 4). Moreover, the MIC of CL when used in combination decreased by 2-8 times compared with that when used alone. This finding implies that infections caused by isolates that are susceptible to the synergistic effects of antimicrobial combination can be treated by using conventional treatment regimens even when these isolates are resistant to individual drugs. This also means that the possibility of CL toxicity can be reduced. A recent retrospective cohort study involving 236 patients with XDR A. baumannii-induced pneumonia found that survival rates (in terms of 28-day mortality) of patients treated with combinations of CL with sulbactam, tigecycline, or carbapenem were superior to those of patients in the control group who were not treated with any active agent against XDR A. baumannii [40].
In conclusion, significant proportion of XDR P. aeruginosa isolates produced MBLs and majority of A. baumannii isolates produced MBL or OXA-23. All the three antimicrobial combinations, i.e., IPM-CL, RIF-CL, and CAZ-CL, exerted additive/indifferent effects on majority of or all XDR P. aeruginosa isolates. And, all the four antimicrobial combinations, i.e., IPM-CL, IPM-AMS, IPM-RIF, and RIF-CL, exerted synergistic or additive/indifferent effects on majority of A. baumannii isolates. However, clinical studies should be performed to validate the application of these in vitro results in patients because in vitro synergy may not be the same as in vivo synergy and to determine the exact mechanisms underlying in vivo synergy.
Go to :
 XML Download
XML Download