

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nowadays, commercial nucleic acid amplification tests (NAATs) are used in clinical laboratories for direct detection of toxigenic Clostridium difficile in stool specimens [1234]. Recently, more than 10 commercial NAATs have been approved by the United States Food and Drug Administration (US FDA). Some of these use PCR techniques, including the multiplex technique, while the others utilize a loop-mediated isothermal amplification (LAMP) or helicase-dependent amplification (HAD) method to detect the presence of C. difficile toxins or regulatory genes [456]. The tcdB gene (coding for TcdB) is usually chosen as a NAAT target because tcdB is produced by almost all toxigenic C. difficile strains [7]. The tcdA gene (coding for TcdA) is less frequently used because roughly 3.3% toxigenic strains from Europe have been reported to be tcdA-negative and a higher prevalence of tcdA-negative C. difficile strains has been reported throughout Asia, including Korea and Japan [8910]. However, some NAATs use tcdA as a target for toxigenic C. difficile because a conserved region of the tcdA gene exists in almost all toxigenic strains, even in strains deficient for TcdA production (ribotype 017) [11].
The growing market for US FDA-approved NAATs reflects the need for rapid and accurate diagnosis of C. difficile infection (CDI). However, NAATs have some limitations as practical methods because they require a special DNA extraction procedure to eliminate PCR inhibitors from stool specimens and are more expensive than EIA, culture, or cytotoxicity cell neutralization assays (CCNA) [234]. Still, increasing mortality/morbidity and recurrence of CDI demand rapid and reliable methods for direct detection of toxigenic C. difficile in stool specimens [12].
The Xpert C. difficile assay (Cepheid, Sunnyvale, CA, USA) uses disposable unitary cartridges, which contain all reagents necessary for multiplex real-time PCR [13]. This assay targets tcdB, cdt (binary toxin), and tcdCΔ117. DNA extraction and amplification are completely automated, and the turn-around time is around 60 min. The Illumigene C. difficile assay (Meridian Bioscience, Cincinnati, OH, USA) uses a LAMP technique targeting a conserved region of the tcdA gene [13]. This assay can also detect toxigenic strains deficient for toxin A (like ribotype 017). Its DNA extraction is manual. DNA is amplified by using illumipro-10 (Meridian Bioscience) under isothermal conditions (65℃); the amplification process produces magnesium pyrophosphate as a byproduct, which increases turbidity of the reaction solution and determines whether a sample is positive. The turn-around time is around 60 min.
Xpert and Illumigene have been widely evaluated by several authors, while BD MAX Cdiff (Becton Dickinson Diagnostics) and IMDx C. difficile for Abbott m2000 (IntelligentMDx, Waltham, MA, USA) assays have been recently introduced in commercial markets.
The BD MAX Cdiff assay amplifies the tcdB gene by real-time PCR [14]. DNA extraction and amplification are completely automated and performed in microfluidic chambers, allowing fast temperature changes and short thermocycling times. The turn-around time is around 100 min. The IMDx C. difficile for Abbott m2000 assay uses real-time PCR for the detection of C. difficile tcdA, tcdB, and toxin B variant (tcdBv) genes in a 96-well plate [14]. Automated sample lysing and target amplification/detection are performed on the m2000 RealTime System (Abbott Laboratories, Abbott Park, IL, USA). The turn-around time is around 180 min.
This study aimed to evaluate the performance of four commercial NAATs (Xpert C. difficile, BD MAX Cdiff, Abbott IMDx, and Illumigene C. difficile) on the same set of stool specimens, to reduce test variables and to compare results with those of TC (bacterial culture and a PCR assay for tcdA and tcdB) for direct detection of tcdA and/or tcdB in stool specimens.
Go to : 
METHODS
1. Specimens
In total, 339 stool specimens were collected from patients with clinical signs compatible with CDI, who were hospitalized at a teaching hospital in Seoul between November 2013 and April 2014. Among 339 specimens, 303 were prospectively collected, and 36 stool specimens collected retrospectively had previously been determined to be positive for C. difficile with tcdA-tcdB+ genes via TC. All retrospective specimens were thawed once and tested within two hours of thawing. The Institutional Review Board of Sanggye Paik Hospital, Seoul, Korea approved the study protocol.
2. Culture and identification of C. difficile
Semi-quantitative culture for C. difficile was performed as previously described [1], and the extent of growth was rated as follows: grade 1, <10 colonies; grade 2, 10-100 colonies; and grade 3, >100 colonies. Briefly, a stool specimen (1.0 mL) was mixed with an equal volume of 70% isopropanol and incubated at room temperature for 30 min. One drop (100 µL) was inoculated onto pre-reduced C. difficile selective agar (CDSA, Becton Dickinson, MD, USA), and the plate was incubated at 37℃ under anaerobic conditions (GasPak EZ Anaerobe Pouch; Becton Dickinson) for 72 hr. C. difficile colonies were identified on the basis of typical morphological features, spore staining, and odor, by using an ANC identification test kit (bioMérieux SA, Marcy-l'Etoile, France). Any Clostridium spp. other than C. difficile growing on culture media was defined as Clostridium spp. other than C. difficile (OTCD).
3. Multiplex PCR assay for tcdA, tcdB, and tpi
Multiplex PCR for tcdA, tcdB, and triose phosphate isomerase (tpi) was performed for 106 C. difficile isolates, as previously described [15]. The PCR product for tpi was 230 bp if the isolate was C. difficile. The PCR product for tcdA was 369 bp if the gene was intact and 110 bp if the isolate contained the variant gene (tcdA-tcdB+). The PCR product for tcdB was 160 bp if the gene was intact.
4. NAATs
1) The Xpert C. difficile assay (Xpert) was performed according to manufacturer's instructions as previously described [13]. Briefly, a stool specimen was collected on a swab from the container and transferred into the sample reagent vial. The vial was vortexed for 10 sec, and the solution was pipetted into the chamber of the cartridge. The cartridge was then inserted into the Xpert instrument, and the test was performed by using the GeneXpert C. difficile assay program.
2) The BD MAX Cdiff assay (Max) was performed according to manufacturer's instructions as previously described [14]. Briefly, a 10-µL stool specimen was added to the sample buffer tube, mixed thoroughly, and vortexed for 60 sec. The sample was extracted and eluted by using magnetic-bead technology DNA extraction. During extraction, 475 µL of the sample was extracted and eluted into 25 µL. The eluate was neutralized and transferred to a master mix tube to rehydrate PCR reagents, and 4.2 µL of the mixture was amplified in the cartridge well.
3) The IMDx C. difficile for Abbott m2000 assay (IMDx) was performed according to manufacturer's instructions as previously described [14]. Initially, sample buffer tubes were created by adding 2.5 mL of Tris-EDTA (TE) buffer to individual tubes. A flocked swab was dipped in the vortexed stool specimen, transferred to the sample buffer tube, swirled, and left immersed in the buffer. The instrument mixed 100 µL of the sample with 400 µL of proteinase K and 200 µL of the process control. Amplification reaction mixtures were prepared by the addition of 15 µL of bacterial lysates to amplification reagents in an Abbott 96-well optical reaction plate. The plate was then manually sealed and transferred to the Abbott m2000rt instrument for amplification and detection.
4) The Illumigene C. difficile assay (Illumigene) was performed according to manufacturer's instructions as previously described [13]. Briefly, a stool specimen was transferred to the sample diluent and vortexed, and 5-10 drops were squeezed into an Illumigene extraction tube. The tube was heated at 95℃ for 10 min and vortexed; 50 µL of the extracted sample was transferred to an Illumigene reaction buffer tube. After vortexing, 50 µL was transferred to the test chamber of the Illumigene assay device containing appropriate beads. The Illumigene device was then inserted into an Illumipro-10 for amplification and detection.
5. Statistical analysis
All statistical analyses were conducted by using SAS version 9.2 (SAS Inc., Cary, NC, USA). Statistical differences in the sensitivity and specificity between four NAATs were analyzed by using the McNemar test. Extents of growth of semi-quantitative culture between the grades were compared by using Chi-square for trend. P value <0.05 was considered statistically significant.
Go to :
RESULTS
Of 303 prospectively collected stool specimens, 70 (23.1%) were culture-positive for C. difficile (23.1%), and 233 (76.9%) were culture-negative (183 cases of no bacteria isolated and 50 cases of OTCD). Of 70 C. difficile positive isolates, 49, 2, and 19 were tcdA+tcdB+, tcdA-tcdB+, and tcdA-tcdB- strains, respectively, and all were tpi-positive. For evaluation of ability to detect tcdA-tcdB+ strains, 36 tcdA-tcdB+ strains were isolated from retrospectively collected specimens. Therefore, total number of TC positive cases was 87 (Table 1).
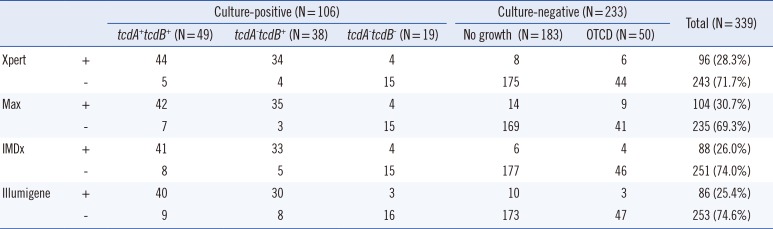
Table 1
Evaluation of four nucleic acid amplification tests, Xpert, Max, IMDx, and Illumigene, in comparison with toxigenic Clostridium difficile culture in stool specimens
![]()
Concordance rate between the four NAATs was 90.3% (306/339). For 306 concordant cases, there were 11 TC-negative/NAATs co-positive cases, and 6 TC-positive/NAATs co-negative cases. Among 33 NAAT discordant cases, 18 were positive only in one of the NAATs (Xpert, 1; Max, 12; IMDx, 1; Illumigene, 4) (Table 2). Sensitivities, specificities, positive predictive values (PPV), and negative predictive values (NPV) of each NAAT were analyzed with 303 prospective stool specimens. Based on TC results, sensitivity and specificity were 90.0% and 92.9% for Xpert, 86.3% and 89.3% for Max, 84.3% and 94.4% for IMDx, and 82.4% and 93.7% for Illumigene, respectively. After reanalyzing data according to consensus standard criteria (either positive in TC or positive in at least two of four NAATs), sensitivities and specificities were 92.7% and 100% for Xpert, 88.4% and 95.7% for Max, 82.6% and 100% for IMDx, and 78.3% and 98.3% for Illumigene, respectively (Table 3). PPV/NPV was 71.4%/97.9% for Xpert, 62.0%/97.0% for Max, 75.4%/96.7% for IMDx, and 72.4%/96.3% for Illumigene based on TC results and 100%/97.9% for Xpert, 85.9%/96.6% for Max, 100%/95.1% for IMDx, and 93.1%/93.9% for Illumigene
based on consensus results.
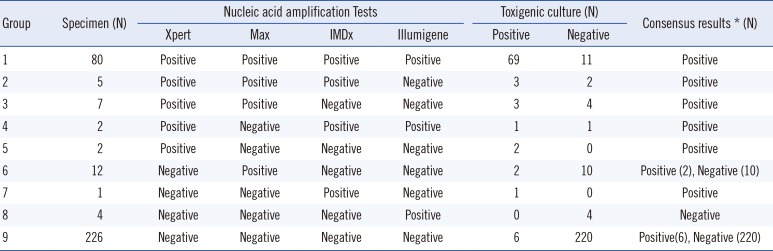

Table 2
Concordant and discordant results among nucleic acid amplification tests in comparison with toxigenic culture and consensus results
![]()
Table 3
Sensitivity and specificity of four nucleic acid amplification tests, Xpert, Max, IMDx, and Illumigene, in comparison with toxigenic culture and consensus standard results
![]()
Of 38 tcdA-tcdB+-positive specimens, positivity rates of Xpert, Max, IMDx, and Illumigene were 89.5% (34/38), 92.1% (35/38), 89.5% (34/38), and 81.6% (31/38), respectively.
Positivity rates of the four NAATs were associated with those of semi-quantitative cultures (Table 4). Positivity rates of Xpert, Max, IMDx, and Illumigene were 77.8%, 66.7%, 66.7%, and 55.6% in grade 1, respectively, but were increased in grade 2 and maximized in grade 3 compared with grade 1 (Chi-square for trend, P<0.05).
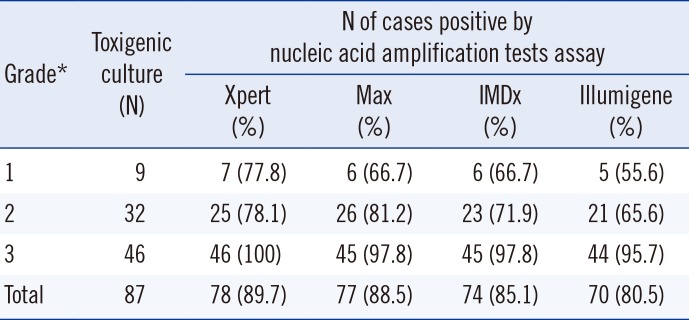
Table 4
Association between four nucleic acid amplification tests, Xpert, Max, IMDx, and Illumigene, in semi-quantitative toxigenic C. difficile culture-positive cases
![]()
Go to :
DISCUSSION
Toxigenic culture (TC) based on bacteriologic culture has been used as a reference standard for evaluation of diagnostic test kits because it is more sensitive than CCNA, EIA, or 2- or 3-step algorithms for detection of C. difficile [12341617]. Although detailed procedures of TC are somewhat variable, TC provides an increased yield of C. difficile compared with CCNA [12345]. However, the sensitivity of NAATs has been reported to be very high, sometimes even higher than that of TC [51318]. Therefore, it is unclear whether positive results of NAATs are true or false positives, although NAATs have been used as a reference standard in some studies. In our study, of 87 TC-positive cases, six were negative in all four NAATs. However, 11 cases were negative in TC but positive in all four NAATs (Table 1). These results suggested that NAATs are more sensitive than TC, although there is no perfect reference method for the detection of the C. difficile toxin gene.
The higher sensitivity of NAATs compared with culture implies the need for strict guidelines for C. difficile testing in stool specimens for because of false positive results in asymptomatic or low-risk patients [519]. According to Humphries et al. [20], the severity of CDI was more associated with EIA positivity than positivity in NAATs, although 42% of severe CDI cases were missed in EIA compared with only 2% in NAATs. Performances of various NAATs have shown sensitivities of 77.3-100% and specificities of 93-99% [12345613142122232425]. Thus, sensitivities and specificities of Xpert, Max, IMDx, and Illumigene in our study represented reliable performances compared with those of previous NAATs.
We speculated reasons underlying discrepancies between TC and NAATs and 33 discordant cases among four NAATs. Of 11 TC-negative/NAATs co-positive specimens, three were negative for C. difficile culture and eight were tcdA-tcdB- strains, which could be interpreted as false-negative cases of TC. Although culture was the most sensitive method for detection of toxigenic C. difficile, performance of C. difficile culture depends on several factors associated with media, pretreatment methods (alcohol or heat), and duration of culture [26]. This may explain the NAAT-positive/C. difficile culture-negative cases. Although there are some mixed colonies of toxigenic C. difficile and non-toxigenic C. difficile strains on a primary culture plate, only colonies of non-toxigenic C. difficile can be detected by TC. These may explain the other eight NAAT-positive/C. difficile culture-positive/tcdA-tcdB- cases. Semi-quantitative culture was either grade 2 (four cases) or 3 (four cases), supporting the hypothesis that some non-toxigenic C. difficile colonies may be mixed with toxigenic colonies. If enrichment culture had been performed, the concordance rate between NAATs and TC might have been increased [27]. Another explanation for the discrepancy between NAAT and TC may be the previous antibiotic treatment for CDI. Among 11 TC-negative/NAATs-positive cases, two cases were previously treated with metronidazole for CDI.
Six TC positive/NAATs co-negative specimens were definitely false-negative cases of NAATs, explained by their low yield of colonies on each agar plate (<5 colony-forming unit [CFU] by semi-quantitative culture in each case) or common inhibitors present in stools. In our study, positivity rates of the four NAATs were associated with those of semi-quantitative cultures (Table 3). Positivity rates of Xpert, Max, IMDx, and Illumigene were <80% in grade 1, but increased in grade 2 and maximized in grade 3. In grade 3, most NAATs showed 95-100% detection rates (Chi-square for trend, P<0.05). These results suggest that although NAATs are highly sensitive, their detection rates may partially depend on amount of tcdA or tcdB produced by C. difficile, and false-negative NAAT results may be associated with a small number of toxigenic C. difficile in stools [12428]. There have been few reports on very low colony counts in discrepant cases for evaluation of Max and IMDx and false-negative NAATs results with low quantities of toxigenic C. difficile in culture [1321].
In our study, 33 cases were discordant among four NAATs. As in discrepant cases between TC and NAATs, the presence of common inhibitors in stool and lower bacterial (toxin) load were possible reasons for the discrepancy. Another possible explanation for limited sensitivity of NAATs is the instability (low sensitivity) of products and procedures. Although PCR-ribotyping was not performed in our study, an association between PCR-ribotypes and positivity rates of NAATs among C. difficile isolates was suggested [2930]. In our study, considering TC results, the sensitivity of Xpert/Max was slightly higher than that of IMDx /Illumigene (90.0%/86.3% vs. 84.3%/82.4%), and the specificity of IMDx/Illumigene was slightly higher than that of Xpert/Max (94.4%/93.7% vs. 92.9%/89.3%). According to a previous review article where TC or enriched TC was used as a reference, the pooled sensitivity was 99% (95% CI, 97-100%) for Xpert, demonstrating the highest pooled sensitivity compared with those of other NAATs [4]. In our study, Xpert had the highest sensitivity compared with the other NAATs, although its sensitivity was not >95%.
The rationale for Illumigene is based on tcdA-tcdB+ strains having various deletions at the 3'-end of the tcdA gene, but its 5'-end remains intact in all strains. Thus, targeting the 5'-end of the tcdA gene should be appropriate [11]. However, in our study, the sensitivity of Illumigene was lower than those of the other three NAATs. For 38 tcdA-tcdB+
C. difficile strains, the positivity rate of Illumigene was inferior (78.9%) to those of Max (92.1%), Xpert (89.5%), and IMDx (89.5%). Thus, the LAMP technique showed a risk of missing clinically relevant tcdA-tcdB+
C. difficile strains. Additionally, considering TC results, the sensitivity of Illumigene is reported to be 73-98%, which is a wider range compared with those of Xpert and Max (93.5-100% and 90.5-97.7%, respectively) [4]. Similar to our results, Walkty et al. [22] showed 73.0% sensitivity of Illumigene compared with that of TC. Although the underlying reason for low sensitivity of Illumigene is unclear, organism load, mutations, and polymorphisms in primer- or probe-binding regions are suggested as major factors for lower detection of C. difficile
tcdA variants, causing false-negative results [13]. However, Gyorke et al. [24] suggested that the lower sensitivity of Illumigene might be attributed to additional sample dilution steps in pre-analytical processing and not non-amplification caused by DNA sequence polymorphism.
Current data on Max and the IMDx are limited because these have been recently introduced. A recent premarket evaluation study of IMDx and Max demonstrated sensitivity/specificity of 92.8%/100% for IMDx and 96.9%/95% for Max, although TC was not performed on whole specimens [14]. In other studies, Max was reported to have slightly lower sensitivity compared with Xpert [2125]. In our study, the sensitivity of Max was similar to that of Xpert, but single-positive cases were highest in Max, suggesting that false-positive results may be more likely in Max compared with the other NAATs. A plausible reason for the increased sensitivity of Max may be the extraction process where nucleic acids are concentrated in specimens [14]. IMDx has redundancy built into the primer design to detect variants of tcdB and tcdA genes, especially rare tcdA-tcdB+ strains. Of 87 TC-positive specimens, three were positive for only one of the two targets in IMDx (one for tcdA and two for tcdB). However, the positive target had a cycle threshold (CT) value of ≥40, suggesting that the target discrepancy is most likely a reflection of the detection limit rather than the strain variant. Similar results were also reported by Stellrecht et al. [14].
An advantage of this study was that TC was performed for all specimens, while TC had generally been performed in discrepant cases in other studies. Another advantage was that the evaluation was simultaneously performed in four NAATs using the same set of stool specimens to reduce variables.
In conclusion, commercial NAATs, including Xpert, Max, IMDx, and Illumigene, may be rapid and reliable methods for direct detection of tcdA and/or tcdB in stool specimens compared with TC. Some differences could be observed in sensitivity and detection rates of NAATs, which may partly depend on the number of toxigenic C. difficile in stool specimens.
Go to :
 XML Download
XML Download