

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor
MDS is a clonal disorder marked by ineffective hematopoiesis, cytopenias, clonal chromosomal abnormalities, and a variable predilection to undergo clonal evolution to AML. Multiple genetic aberrations occur during the clonal evolution of MDS, and in the majority of cases, somatic mutations result from the deletion of all or part of a chromosome [1].
BCR-ABL1 is a hybrid from the ABL1 gene on chromosome 9 and the BCR gene on chromosome 22. The fusion protein encoded from this gene has strong tyrosine kinase activity and is involved in the pathogenesis of several hematologic disorders. BCR-ABL1 genes are categorized into three types, based on differences in the BCR gene's breakpoint, which appear to be related to the disease phenotype. The BCR-ABL1 fusion gene is found in CML and in some cases of acute lymphoblastic leukemia [2]. However, reports on BCR-ABL1-positive MDS cases are extremely rare [3456]. Here, we report an unusual case of MDS progressing to AML with an e1a2 BCR-ABL1 fusion transcript and a complex karyotype, including monosomy 7.
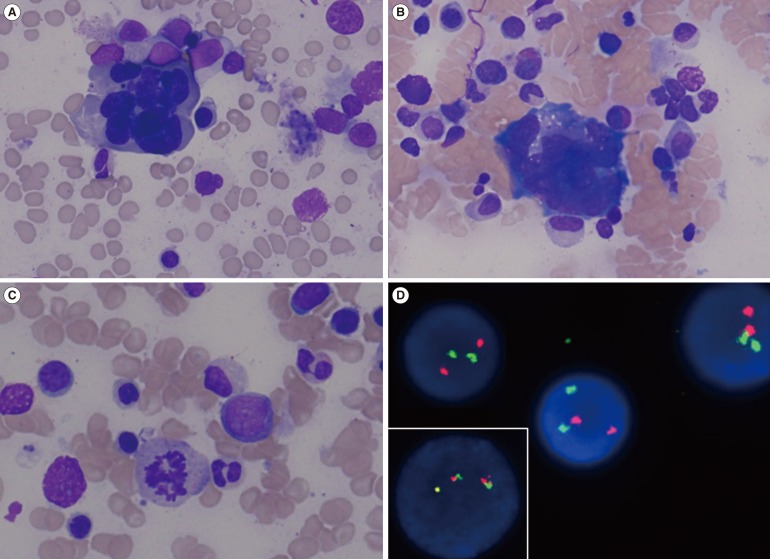
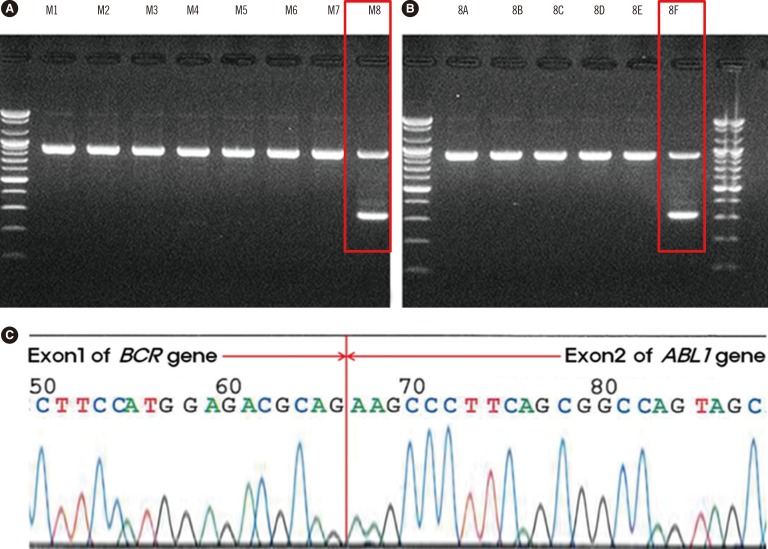
A 65-yr-old man was admitted for evaluation of persistent pancytopenia with 9% blasts in the peripheral blood. He presented with general weakness and breathlessness. Evaluation of the bone marrow (BM) disclosed hypercellularity with mild erythroid hyperplasia, blasts count of 18%, and remarkable dyshematopoiesis (Fig. 1). Immunophenotype analysis of BM cells using flow cytometry showed that the blasts were positive (>20% of cells) for CD13 (45%), CD33 (97%), CD117 (68%), CD34 (97%), and HLA-DR (43%), and negative for other megakaryocytic and lymphoid markers. Multiplex reverse transcriptase polymerase chain reaction (RT-PCR) evaluation of total RNA isolated from BM cells (HemaVision kit; DNA-Diagnostic, Risskov, Denmark) indicated an e1a2 (p190 BCR-ABL1) rearrangement, confirmed on two independent cDNAs and via direct sequencing (Fig. 2). Quantitative RT-PCR analysis (Real-Q BCR-ABL1 quantification kit; BioSewoom, Seoul, Korea) revealed the BCR-ABL1 to ABL1 transcript ratio to be 0.001339977. The fluorescence in situ hybridization signal for BCR-ABL1 rearrangement was found in one interphase cell out of 296 analyzed cells (Fig. 1D). There was no evidence of other molecular abnormalities such as mutations in JAK2 or calreticulin. Conventional cytogenetic analysis revealed a complex abnormality without the Philadelphia (Ph) chromosome: 44,XY,del(5)(q31),-7,del(12)(p12),-14,-16,+mar [cp20]. The final diagnosis was MDS subtype refractory anemia with excess blasts-2 (RAEB-2). The patient died before undergoing a follow-up BM examination owing to lung cancer, which was found shortly after the MDS diagnosis.
BCR-ABL1-positive de novo MDS is a very rare disease, and when it manifests with excess blasts, as in this case, it may be confused with the accelerated phase of CML. However, several features of this case differentiate it from CML. First, our patient did not have organomegalies, such as splenomegaly, or any related symptoms, which are common in CML. Second, our patient did not display basophilia in the peripheral blood or BM, which is common in CML. Third, BM examination showed severe dyshematopoietic features without findings of myeloproliferative neoplasms. Fourth, monosomy 7 and del(5)(q31) identified using chromosomal analysis are typical aberrations of MDS.
It is common that BCR-ABL1-negative MDS changes to BCR-ABL1-positive MDS after disease progression [3456]. In the case of BCR-ABL1-positive MDS, most patients show excess blasts on the verge of transformation to AML [678], which implies that the appearance of BCR-ABL1-positive clones is likely to be closely associated with leukemogenesis and triggers MDS to transform into AML.
Jacobsen et al. [9] proposed three possible explanations for the acquisition of the late-appearing Ph chromosome: 1) it may have been present on initial presentation; however, the techniques used were inadequate to detect the BCR rearrangement; 2) it may represent further evidence of multistep pathogenesis; and 3) the presence of the Ph chromosome in some cells may represent the development of a new clone of cells in leukemic relapse. In this case, we presume that the third explanation may be fitting. The BCR-ABL1-positive clone was most likely detected on emergence because the BCR-ABL1 copy number and BCR-ABL1 to ABL1 transcript ratio during quantitative RT-PCR analysis were found to be very low. Moreover, a typical Ph chromosome was not found in 20 metaphase cells by conventional cytogenetic analysis. To the best of our knowledge, this is the first report of de novo MDS RAEB-2 with the cryptic e1a2 subtype of BCR-ABL1 rearrangement and complex chromosomal abnormality in Korea. Currently, there is no established treatment method that is distinguished from the usual MDS treatment. In the future, a more systematic study of this disease is needed with respect to serial biologic monitoring, therapy, and outcome.
 XML Download
XML Download