

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Thyroid cancer is one of the most common malignancies worldwide [1]. Among the numerous genetic alterations that have been identified to play a fundamental role in the tumorigenesis of various thyroid cancers, the c.1799T>A mutation in the BRAF gene is of particular interest. This mutation results in the expression of the BRAF V600E mutant protein, and causes the constitutive activation of a serine/threonine kinase [23]. This serine/threonine kinase is found in up to 80% of papillary thyroid carcinomas (PTCs) and 50% of anaplastic thyroid carcinomas, but not in follicular neoplasms or benign nodules [456]. The advent of molecular diagnostic methods has allowed for easier detection of the BRAF V600E mutation in thyroid fineneedle aspirates (FNAs), in clinical pathology and clinical oncology practices. These molecular methods complement routine cytopathological examinations and are of significant value in identifying diagnostic and prognostic molecular markers and therapeutic targets for thyroid cancer [27891011].
Numerous BRAF assays employing various technologies are presently in use. These technologies encompass conventional Sanger sequencing, pyrosequencing, LightCycler PCR (Roche Diagnostics, Mannheim, Germany) with melting curve analysis, the colorimetric Mutector assay (TrimGen, Sparks, MD, USA), restriction fragment length polymorphisms, the amplification refractory mutation system, and dual-priming oligonucleotide (DPO) PCR [12]. The BRAF V600E mutation might only be present in malignant cells of thyroid FNA cytology specimens; however, these specimens contain a mixture of cell types and are of variable quality [13]. Therefore, a sensitive assay is required to detect the BRAF V600E mutation in FNA specimens [12]. Although conventional Sanger sequencing is the standard method used to detect the BRAF V600E mutation, it is not sensitive enough (approximately 20%) to detect the mutation if it is present at a low frequency in specimens [14]. Other molecular methods with mutation enrichment that have a higher sensitivity than conventional Sanger sequencing, such as DPO PCR and mutant enrichment with 3'-modified oligonucleotide (MEMO) sequencing, have also been developed [121415].
In the present study, we evaluated a new real-time PCR assay using DPO technology, the Anyple BRAF V600E Real-time Detection system (Seegene, Seoul, Korea), and compared the results with those obtained from the Seeplex BRAF V600E ACE Detection system (Seegene), which is based on conventional DPO PCR technology.
METHODS
1. Patients
We collected 258 consecutive FNA specimens from Korean patients (131 women and 127 men; patients' age showed normal distribution with 51.0±11.2 yr, mean±SD) who were found to have malignant or indeterminate thyroid nodules by ultrasonography. After informed consent was granted by each patient, fine-needle aspiration was performed under ultrasonographic guidance by experienced radiologists.
2. Methods
The aspirates were placed onto glass slides and fixed in 95% alcohol for cytological examination. Remaining materials were collected for BRAF V600E mutation analysis. On the basis of cytology, each specimen was classified into one of six categories [16]: benign, follicular lesion of undetermined significance/atypia of undetermined significance (AUS/FLUS), follicular neoplasm (FN)/suspicious for FN (SFN), suspicious for malignancy (SMC), malignant, and nondiagnostic because of unsatisfactory sample quality. For patients who underwent a thyroidectomy, histopathological examination was performed by specialized pathologists.
Genomic DNA was extracted from the aspirated thyroid cells by using a QIAamp DNA Micro Kit (QIAGEN, Chatsworth, CA, USA) according to the manufacturer's instructions. All FNA specimens were tested for the BRAF V600E mutation by using the Seeplex and Anyplex methods. Any conflicting results, including invalid results (n=17), between the two assays were confirmed with MEMO sequencing. [12]. The Seeplex assays were carried out on a GeneAmp 9700 PCR thermal cycler (Applied Biosystems, Foster City, CA, USA) as previously described [17]. The Anyplex assays were performed according to the manufacturer's instructions. In brief, the reaction mixture contained 2 µL of 10× BRAF Oligo Mix including amplification and detection reagents, 3 µL of 8-methoxypsoralen solution to prevent carryover contamination, 10 µL of 2× Anyplex PCR master mix including DNA polymerase, and buffer with deoxynucleoside triphosphates. We added 5 µL of template DNA to each reaction mixture to achieve a final reaction volume of 20 µL. The real-time PCR was performed by using a CFX96 real-time PCR system (Bio-Rad, Hercules, CA, USA). The thermal cycling conditions involved an initial denaturation step at 95℃ for 15 min, followed by 15 amplification cycles (95℃ for 15 sec and 60℃ for 30 sec), and then a further 35 amplification cycles (95℃ for 30 sec and 60℃ for 32 sec). For real-time PCRs, the cycle threshold (Ct) was defined as the cycle at which a significant increase in fluorescence was detected. Specimens and the internal control, with a Ct value <33 were considered positive. Each assay contained a positive and a negative control. MEMO sequencing was carried out as previously described [12].
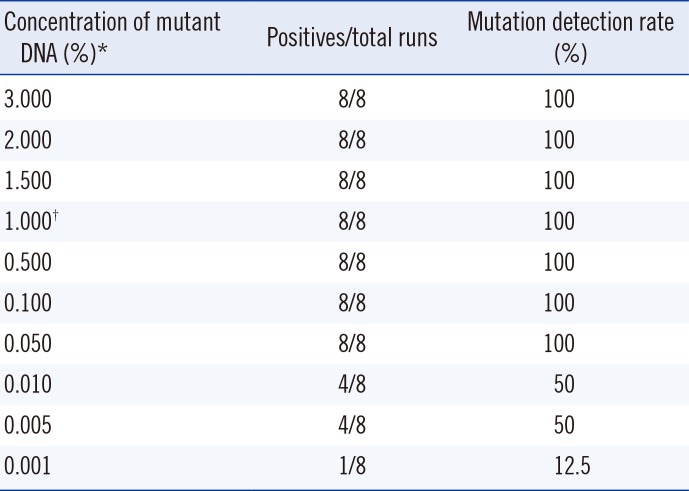
Correlations between cytological and histological findings were determined, and BRAF V600E mutation detection results for the Seeplex and Anyplex assays were compared. To evaluate the limit of detection (LOD) for each assay, mutant DNA (100 ng/µL) obtained from a BRAF V600E-positive cell line (SNU-790) was serially diluted with a V600E-negative cell line (DMPK-M). Eight replicates at eight different concentrations (0.001-3.000%) were tested and, the LOD was determined by probit analysis.
3. Statistical analysis
Statistical analyses were performed by using SPSS 20.0 (SPSS Inc., Chicago, IL, USA) and MedCalc software (MedCalc, Ostend, Belgium). We calculated kappa inter-rater agreement values with 95% confidence intervals (CIs) to compare the detection rates of BRAF V600E mutations between the Seeplex and Anyplex assays. Kappa values were interpreted as follows: 0-0.20 as slight; 0.21-0.40 as fair; 0.41-0.60 as moderate; 0.61-0.80 as substantial; and 0.81-1 as almost perfect agreement [18].
RESULTS
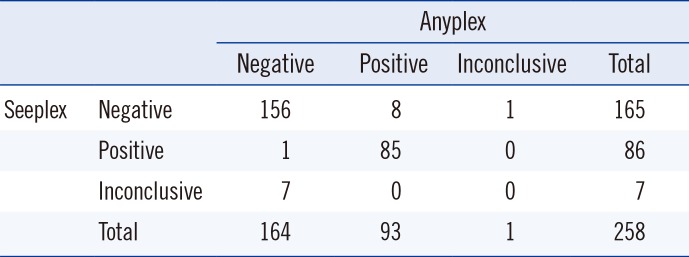
The BRAF V600E mutation was detected in 36.4% (94/258) of FNA specimens by either the Seeplex or Anyplex assay. These included 86 (33.3%) cases as determined by Seeplex and 93 (36.0%) cases by Anyplex (Table 1). The results of the Seeplex and Anyplex assays showed 93.4% (241/258) agreement, with a kappa value of 0.861 (95% CI: 0.798-0.923). We observed more invalid results for the Seeplex (2.7%, n=7) than for the Anyplex (0.4%, n=1) assays.
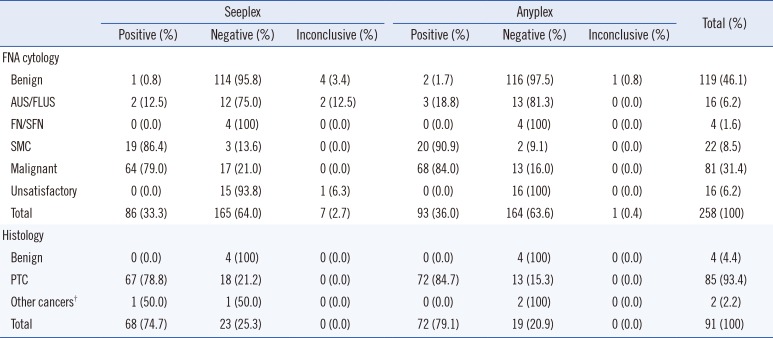
According to our cytology results, 31.4% (81/258) of cases were diagnosed as malignant. These included 80 PTCs and one medullary thyroid cancer (MTC). Of the 81 specimens diagnosed as malignant, the BRAF V600E mutation was detected in 64 (79.0%) and 68 (84.0%) specimens by Seeplex and Anyplex, respectively (Table 2). Among the 22 specimens classified as SMC, the detection rates of the BRAF V600E mutation by Seeplex and Anyplex were 86.4% (19/22) and 90.9% (20/22), respectively.
Thyroidectomies and post-surgical histopathological examinations were performed for 35.3% (91/258) of samples, with four classified as benign, six as AUS/FLUS, 18 as SMC, and 63 as malignant by FNA cytology. These samples included 85 PTCs, four benign thyroid nodules (three benign nodular hyperplasias and one follicular adenoma), and two other thyroid carcinomas (one follicular thyroid carcinoma and one MTC). Of the 85 specimens diagnosed as PTCs, the BRAF V600E mutation was detected in 67 (78.8%) cases by Seeplex and 72 (84.7%) cases by Anyplex assays.
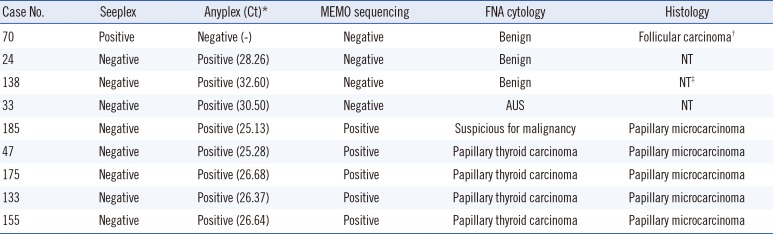
As shown in Table 3, conflicting results were observed in nine cases. For one case, the BRAF V600E mutation was detected by Seeplex only, while for the other eight cases, the mutation was detected by the Anyplex assay only. Of the eight BRAF V600E-positive samples by Anyplex, five were also positive according to MEMO sequencing, cytology results, and post-surgical pathologic findings consistent with PTC. Unfortunately, thyroidectomy was not performed for three cases that were positive by Anyplex but negative by Seeplex and MEMO sequencing. Therefore, confirmatory information for the histopathological findings regarding PTC was not available.
All specimens with invalid results by Seeplex and Anyplex were diagnosed as benign or FLUS on FNA cytological examination, except for one specimen that was BRAF V600E-positive by MEMO sequencing, and yielded unsatisfactory results by FNA cytological examination. Histopathological examinations following thyroidectomy were not performed. No specimens were identified as having the BRAF V600E mutation by MEMO sequencing and Seeplex, but not by Anyplex, confirming the higher sensitivity of the Anyplex assay over the Seeplex assay.
All results were positive at a concentration of 0.05%. The LOD as determined by probit analysis was 0.046% (95% CI: 0.019-0.532) (Table 4).
DISCUSSION
We evaluated the performance of the Anyplex assay in detecting the BRAF V600E mutation using clinical FNA specimens collected from Korean patients with malignant or indeterminate thyroid nodules. In specimens diagnosed as PTC, detection rates for the BRAF V600E mutation were higher with the Anyplex assay than with the Seeplex assay. More specimens diagnosed with PTC contained the BRAF V600E mutation as determined by the Anyplex assay and MEMO sequencing, including conflicting results. Therefore, we concluded that the Anyplex assay was more sensitive than the Seeplex assay.
In the current study, histopathological findings were not used to discriminate between true positives and true negatives for the BRAF V600E mutation, in evaluating the mutation detection sensitivity and specificity between diagnostic methods. Conventional Sanger sequencing is the standard method by which the BRAF V600E mutation is usually detected. However, this method is not sensitive enough to detect the mutation when it occurs at low frequencies in specimens. Therefore, highly sensitive MEMO sequencing has been used to detect the BRAF V600E mutation [12]. We used this as the reference method to analyze samples that provided conflicting results in the Seeplex and Anyplex assays. Our Anyplex results strongly corresponded with the Seeplex results, with a kappa value of 0.861 indicating almost perfect agreement. The clinical sensitivity (detection rate) of the Anyplex assay for BRAF V600E detection was higher than that of the Seeplex assay, for the 81 FNA specimens diagnosed as malignant and the 22 specimens diagnosed as SMC. In addition, among the 85 specimens diagnosed as PTCs on the basis of post-thyroidectomy histopathological findings, detection rates were 78.8% (67/85) by Seeplex and 84.7% (72/85) by Anyplex. The analytical sensitivity test revealed that Anyplex had a higher sensitivity than Seeplex, but a lower sensitivity than MEMO sequencing. These results were comparable with previous studies, which found that DPO real-time PCR and MEMO sequencing were more sensitive than DPO PCR [1219].
In this study, one case that was BRAF V600E-positive by Seeplex, but negative by the Anyplex assay and MEMO sequencing was finally diagnosed as minimally invasive follicular carcinoma on histopathological examination. Considering that only about 1% of follicular carcinomas reportedly contain the BRAF V600E mutation [20], and that analytical sensitivities of the Anyplex assay and MEMO sequencing were higher than that of Seeplex, the BRAF mutation status of this sample was questionable and could be a false positive. In three samples, the BRAF V600E mutation was detected only by Anyplex, not by Seeplex or MEMO sequencing; however, none of these patients underwent thyroidectomy. There were no false positive results from the Anyplex assay when post-thyroidectomy histopathological results were available to be evaluated as references.
The LOD of the Anyplex assay in this study was 0.046%. The LOD claimed by the manufacturer and determined by our comparison test was 1.0%, which was better than that of the Seeplex assay (10.0%), but it was not good as that for MEMO sequencing (0.1%). The reproducibility of the Anyplex assay was verified and found to be close to the LOD claimed by the manufacturer. The analytical sensitivity of the three diagnostic methods was estimated by using the SNU-790 BRAF V600E-positive cell line, which could be considered as a limitation of this study. Another limitation might be that over 66% of the conflicting results could not be solved because surgical histopathological results could not be obtained.
In conclusion, the real-time PCR-based Anyplex method was more sensitive than the Seeplex assay in detecting the BRAF V600E mutation in FNA specimens from thyroid nodules. Anyplex assay could be more useful in diagnosis of PTCs harboring the BRAF V600E mutation.
 XML Download
XML Download