This article has been
cited by other articles in ScienceCentral.
Abstract
We compared the activities of tedizolid to those of linezolid and other commonly used antimicrobial agents against gram-positive cocci recovered from patients with skin and skin structure infections (SSSIs) and hospital-acquired pneumonia (HAP) in Korean hospitals. Gram-positive isolates were collected from 356 patients with SSSIs and 144 patients with HAP at eight hospitals in Korea from 2011 to 2014. SSSIs included impetigo, cellulitis, erysipelas, furuncles, abscesses, and infected burns. Antimicrobial susceptibility was tested by using the CLSI agar dilution method. All of the gram-positive isolates were inhibited by ≤1 µg/mL tedizolid. The minimum inhibitory concentration [MIC]90 of tedizolid was 0.5 µg/mL for methicillin-resistant Staphylococcus aureus, which was 4-fold lower than that of linezolid. Tedizolid may become a useful option for the treatment of SSSIs and HAP caused by gram-positive bacteria.
Keywords: Tedizolid, Skin, Soft tissue, Infection, Pneumonia, Gram-positive bacteria
Skin and skin structure infections (SSSIs) are common problems in both inpatients and outpatients. The vast majority of SSSIs are caused by gram-positive organisms that are normal flora on the skin of human beings. Staphylococci and streptococci cause majority of gram-positive infections [
1]. A recent increase in staphylococcal infections caused by methicillin-resistant
Staphylococcus aureus (MRSA) has resulted in a significant increase of cases of MRSA pneumonia in the health care setting, especially in the chronically ill population [
2]. Vancomycin has been the cornerstone of treatment for MRSA infections. However, recently, vancomycin-resistant
S. aureus and linezolid-resistant
Staphylococcus strains have emerged [
345]. These strains pose significant challenges to the clinical treatment of infections caused by these organisms. Tedizolid offers broad
in vitro activity against gram-positive pathogens, including MRSA and strains resistant to vancomycin or linezolid, and has greater potency than other drugs of its class [
67]. It was specifically designed to be active against linezolid-resistant
S. aureus, including strains containing the multidrug-resistant
cfr gene [
8].
Tedizolid phosphate was recently approved by the U.S. Food and Drug Administration to treat patients with acute bacterial SSSI caused by
S. aureus, various
Streptococcus species, and
Enterococcus. In addition, planned studies will investigate the potential role of tedizolid in the treatment of community-acquired bacterial pneumonia and hospital-acquired pneumonia (HAP) [
9]. We published a previous report focusing on the activity of tedizolid against collections of clinical isolates in a single institution, but it was not characterized by infection type [
10]. Therefore, the present study aimed to compare the activities of tedizolid to those of linezolid and other commonly used antimicrobial agents against gram-positive cocci recovered from patients with SSSIs and HAP in Korean hospitals.
Non-duplicated aerobic and anaerobic gram-positive isolates were collected from clinical specimens of 356 patients with SSSIs and 144 patients with HAP at eight hospitals in Seoul and Gyeonggi province, Korea from 2011 to 2014. SSSIs included impetigo, cellulitis, erysipelas, furuncles, abscesses, and infected burns [
111]. HAP was defined as pneumonia that occurred 48 hr or more after admission.
Species were identified by using conventional methods or the Vitek 2 system (bioMérieux, Marcy l'Etolile, France). Antimicrobial susceptibility was tested by using the CLSI agar dilution method [
1213]. Mueller-Hinton agar was used as a growth medium (Becton Dickinson, Cockeysville, MD, USA) for testing
Staphylococcus spp. and
Enterococcus spp.: Mueller-Hinton agar supplemented with 5% sheep blood for
Streptococcus spp.; Brucella agar (Becton Dickinson) supplemented with 5 µg/mL hemin, 1 µg/mL vitamin K1; and 5% laked sheep blood for anaerobic bacteria. Tedizolid and linezolid (Dong-A ST, Seoul, Korea); erythromycin, tetracycline, oxacillin and penicillin G (Sigma Chemical, St. Louis, MO, USA); piperacillin and tazobactam (Yuhan, Seoul, Korea); clindamycin (Korea Upjohn, Seoul, Korea); levofloxacin (Daiichi Pharmaceutical, Tokyo, Japan); cefotetan (Daiichi Pharmaceutical); ampicillin and gentamicin (Chong Kun Dang, Seoul, Korea); cefoxitin and imipenem (Merck Sharp & Dohme, Rahway, NJ, USA); meropenem (Sumitomo, Tokyo, Japan); metronidazole (ChoongWae, Seoul, Korea); trimethoprim and sulfamethoxazole (Dong Wha, Seoul, Korea); vancomycin (Daewoong, Seoul, Korea); and teicoplanin (Sanofi Aventis, Bridgewater, NJ, USA) were used as antimicrobial powders. American type culture collection strains of
S. aureus (ATCC29213),
E. faecalis (ATCC 29212),
S. pneumoniae (ATCC 49619),
Bacteroides fragilis (ATCC 25285), and
B. thetaiotaomicron (ATCC 29741) were used as reference strains. The non-meningeal breakpoints of penicillin G and cefotaxime were used for
S. pneumoniae. This study used the breakpoints of tedizolid suggested by the US Food and Drug Administration [
14].
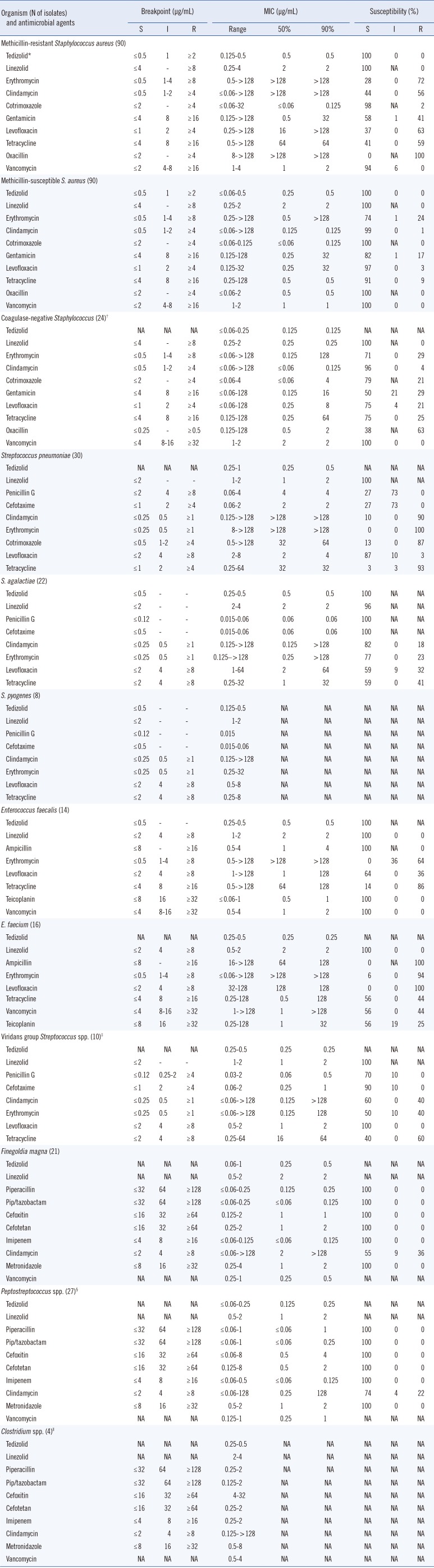
All of the aerobic and anaerobic gram-positive isolates in patients with SSSIs were inhibited by ≤1 µg/mL tedizolid (
Table 1). The most potent drugs against MRSA were tedizolid (minimum inhibitory concentration [MIC]
90=0.5 µg/mL), linezolid (MIC
90=2 µg/mL), and vancomycin (MIC
90=2 µg/mL). The MIC range of tedizolid was 0.125 to 0.5 µg/mL for MRSA, while that of linezolid was 0.25 to 4 µg/mL. The MIC
90s of tedizolid were 0.5 µg/mL for both MRSA and methicillin-susceptible
S. aureus (MSSA) and ≤0.125 µg/mL for coagulase-negative staphylococci, which were 2- to 4-fold lower than those of linezolid. These MIC values were similar to those described in previous reports [
1015]. The MICs of tedizolid were 0.25 µg/mL for all three vancomycin-intermediate
S. aureus isolates.
The MIC ranges of tedizolid were 0.25 to 0.5 µg/mL for Enterococcus, while those of linezolid were 0.5 to 2 µg/mL. Tedizolid inhibited all vancomycin-resistant Enterococcus at 0.5 µg/mL. When the meningeal breakpoint was applied, most of the pneumococcal isolates tested were not susceptible to penicillin G or cefotaxime. However, the MIC range of tedizolid was 0.25 to 1 µg/mL, and the MIC90 (0.5 µg/mL) was 4-fold lower than that of linezolid. Tedizolid inhibited all the isolates of viridans Streptococcus spp. and β-hemolytic streptococci such as S. pyogenes and S. agalactiae at 0.5 µg/mL.
Tedizolid had excellent activity against gram-positive anaerobes recovered from SSSIs (
Table 1). The MIC ranges of tedizolid were 0.06 to 1 µg/mL for
Finegoldia magna and ≤0.06 to 0.25 µg/mL for the other
Peptostreptococcus spp. The MIC
90 values for these organisms were 0.5 and 0.25 µg/mL, respectively, which were 4-8 fold lower than those of linezolid. All the
Clostridium spp. isolates were inhibited by tedizolid at 0.5 µg/mL.
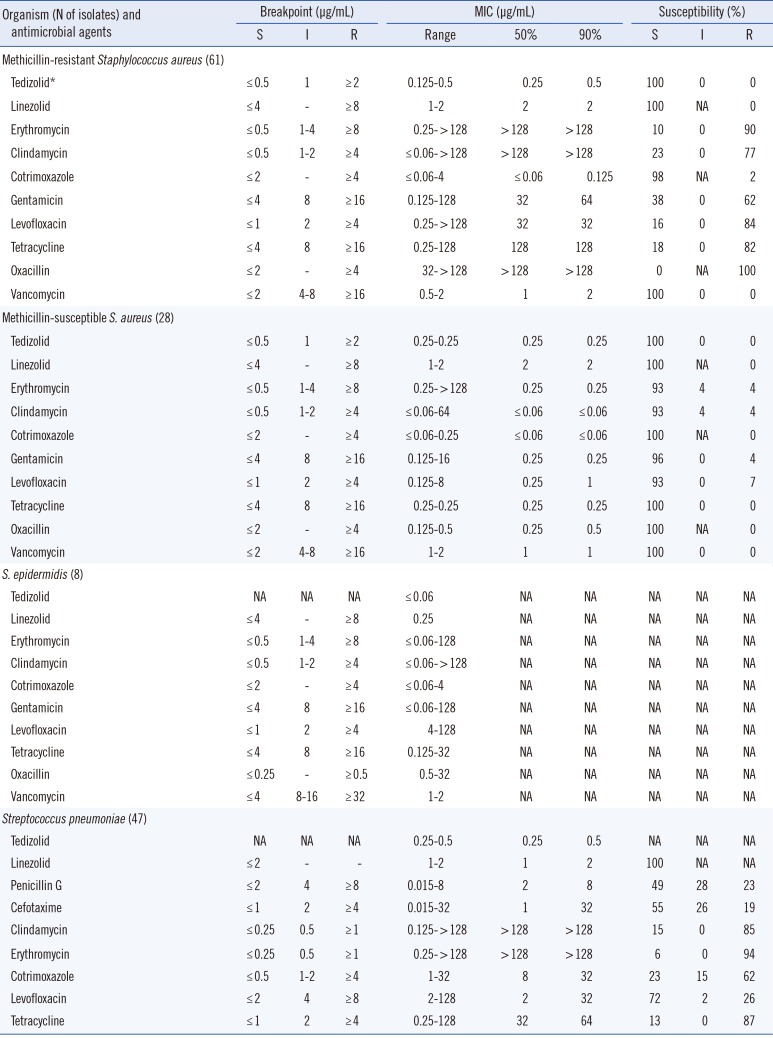
All the gram-positive isolates in patients with HAP were inhibited by ≤0.5 µg/mL tedizolid (
Table 2). The MIC ranges of tedizolid were 0.125 to 0.5 µg/mL for MRSA and 0.25 µg/mL for MSSA. The MIC
90 values of tedizolid were 0.25, 0.5, and 0.5 µg/mL for MSSA, MRSA, and pneumococci, respectively, which were 4- to 8-fold lower than those of linezolid.
In summary, the MIC values of tedizolid in this study were not significantly different according to type of infection. All organisms tested were susceptible to tedizolid, nevertheless the breakpoint of tedizolid is 4- or 8-fold lower than that of linezolid. Tedizolid is a potent agent with high in vitro activity against common aerobic and anaerobic gram-positive pathogens in SSSIs and HAP. Tedizolid may become a useful option for the treatment of SSSIs and HAP.
Table 1
Comparative in vitro activities of tedizolid and other antimicrobial agents against bacteria recovered from patients with skin and skin structure infections
|
Organism (N of isolates) and antimicrobial agents |
Breakpoint (µg/mL) |
MIC (µg/mL) |
Susceptibility (%) |
|
S |
I |
R |
Range |
50% |
90% |
S |
I |
R |
|
Methicillin-resistant Staphylococcus aureus (90) |
|
|
|
|
|
|
|
|
|
|
Tedizolid*
|
≤ 0.5 |
1 |
≥2 |
0.125-0.5 |
0.5 |
0.5 |
100 |
0 |
0 |
|
Linezolid |
≤4 |
- |
≥8 |
0.25-4 |
2 |
2 |
100 |
NA |
0 |
|
Erythromycin |
≤ 0.5 |
1-4 |
≥8 |
0.5- > 128 |
> 128 |
> 128 |
28 |
0 |
72 |
|
Clindamycin |
≤ 0.5 |
1-2 |
≥4 |
≤ 0.06- > 128 |
> 128 |
> 128 |
44 |
0 |
56 |
|
Cotrimoxazole |
≤2 |
- |
≥4 |
≤ 0.06-32 |
≤ 0.06 |
0.125 |
98 |
NA |
2 |
|
Gentamicin |
≤4 |
8 |
≥ 16 |
0.125- > 128 |
0.5 |
32 |
58 |
1 |
41 |
|
Levofloxacin |
≤1 |
2 |
≥4 |
0.25- > 128 |
16 |
> 128 |
37 |
0 |
63 |
|
Tetracycline |
≤4 |
8 |
≥ 16 |
0.5- > 128 |
64 |
64 |
41 |
0 |
59 |
|
Oxacillin |
≤2 |
- |
≥4 |
8- > 128 |
> 128 |
> 128 |
0 |
NA |
100 |
|
Vancomycin |
≤2 |
4-8 |
≥ 16 |
1-4 |
1 |
2 |
94 |
6 |
0 |
|
Methicillin-susceptible S. aureus (90) |
|
|
|
|
|
|
|
|
|
|
Tedizolid |
≤ 0.5 |
1 |
≥2 |
≤ 0.06-0.5 |
0.25 |
0.5 |
100 |
0 |
0 |
|
Linezolid |
≤4 |
- |
≥8 |
0.25-2 |
2 |
2 |
100 |
NA |
0 |
|
Erythromycin |
≤ 0.5 |
1-4 |
≥8 |
0.25- > 128 |
0.5 |
> 128 |
74 |
1 |
24 |
|
Clindamycin |
≤ 0.5 |
1-2 |
≥4 |
≤ 0.06- > 128 |
0.125 |
0.125 |
99 |
0 |
1 |
|
Cotrimoxazole |
≤2 |
- |
≥4 |
≤ 0.06-0.125 |
≤ 0.06 |
0.125 |
100 |
NA |
0 |
|
Gentamicin |
≤4 |
8 |
≥ 16 |
0.125-128 |
0.25 |
32 |
82 |
1 |
17 |
|
Levofloxacin |
≤1 |
2 |
≥4 |
0.125-32 |
0.25 |
32 |
97 |
0 |
3 |
|
Tetracycline |
≤4 |
8 |
≥ 16 |
0.25-128 |
0.5 |
0.5 |
91 |
0 |
9 |
|
Oxacillin |
≤2 |
- |
≥4 |
≤ 0.06-2 |
0.5 |
0.5 |
100 |
NA |
0 |
|
Vancomycin |
≤2 |
4-8 |
≥ 16 |
1-2 |
1 |
1 |
100 |
0 |
0 |
|
Coagulase-negative Staphylococcus (24)†
|
|
|
|
|
|
|
|
|
|
|
Tedizolid |
NA |
NA |
NA |
≤ 0.06-0.25 |
0.125 |
0.125 |
NA |
NA |
NA |
|
Linezolid |
≤4 |
- |
≥8 |
0.25-2 |
0.25 |
0.25 |
100 |
NA |
0 |
|
Erythromycin |
≤ 0.5 |
1-4 |
≥8 |
≤ 0.06- > 128 |
0.125 |
128 |
71 |
0 |
29 |
|
Clindamycin |
≤ 0.5 |
1-2 |
≥4 |
≤ 0.06- > 128 |
≤ 0.06 |
0.125 |
96 |
0 |
4 |
|
Cotrimoxazole |
≤2 |
- |
≥4 |
≤ 0.06-4 |
≤ 0.06 |
4 |
79 |
NA |
21 |
|
Gentamicin |
≤4 |
8 |
≥ 16 |
≤ 0.06-128 |
0.125 |
16 |
50 |
21 |
29 |
|
Levofloxacin |
≤1 |
2 |
≥4 |
≤ 0.06-128 |
0.25 |
8 |
75 |
4 |
21 |
|
Tetracycline |
≤4 |
8 |
≥ 16 |
0.125-128 |
0.25 |
64 |
75 |
0 |
25 |
|
Oxacillin |
≤ 0.25 |
- |
≥ 0.5 |
0.125-128 |
0.5 |
2 |
38 |
NA |
63 |
|
Vancomycin |
≤4 |
8-16 |
≥ 32 |
1-2 |
2 |
2 |
100 |
0 |
0 |
|
Streptococcus pneumoniae (30) |
|
|
|
|
|
|
|
|
|
|
Tedizolid |
NA |
NA |
NA |
0.25-1 |
0.25 |
0.5 |
NA |
NA |
NA |
|
Linezolid |
≤2 |
- |
- |
1-2 |
1 |
2 |
100 |
NA |
NA |
|
Penicillin G |
≤2 |
4 |
≥8 |
0.06-4 |
4 |
4 |
27 |
73 |
0 |
|
Cefotaxime |
≤1 |
2 |
≥4 |
0.06-2 |
2 |
2 |
27 |
73 |
0 |
|
Clindamycin |
≤ 0.25 |
0.5 |
≥1 |
0.125- > 128 |
> 128 |
> 128 |
10 |
0 |
90 |
|
Erythromycin |
≤ 0.25 |
0.5 |
≥1 |
8- > 128 |
> 128 |
> 128 |
0 |
0 |
100 |
|
Cotrimoxazole |
≤ 0.5 |
1-2 |
≥4 |
0.5- > 128 |
32 |
64 |
13 |
0 |
87 |
|
Levofloxacin |
≤2 |
4 |
≥8 |
2-8 |
2 |
4 |
87 |
10 |
3 |
|
Tetracycline |
≤1 |
2 |
≥4 |
0.25-64 |
32 |
32 |
3 |
3 |
93 |
|
S. agalactiae (22) |
|
|
|
|
|
|
|
|
|
|
Tedizolid |
≤ 0.5 |
- |
- |
0.25-0.5 |
0.5 |
0.5 |
100 |
NA |
NA |
|
Linezolid |
≤2 |
- |
- |
2-4 |
2 |
2 |
96 |
NA |
NA |
|
Penicillin G |
≤ 0.12 |
- |
- |
0.015-0.06 |
0.06 |
0.06 |
100 |
NA |
NA |
|
Cefotaxime |
≤ 0.5 |
- |
- |
0.015-0.06 |
0.06 |
0.06 |
100 |
NA |
NA |
|
Clindamycin |
≤ 0.25 |
0.5 |
≥1 |
0.125- > 128 |
0.125 |
> 128 |
82 |
0 |
18 |
|
Erythromycin |
≤ 0.25 |
0.5 |
≥1 |
0.125- > 128 |
0.25 |
> 128 |
77 |
0 |
23 |
|
Levofloxacin |
≤2 |
4 |
≥8 |
1-64 |
2 |
64 |
59 |
9 |
32 |
|
Tetracycline |
≤2 |
4 |
≥8 |
0.25-32 |
1 |
32 |
59 |
0 |
41 |
|
S. pyogenes (8) |
|
|
|
|
|
|
|
|
|
|
Tedizolid |
≤ 0.5 |
- |
- |
0.125-0.5 |
NA |
NA |
NA |
NA |
NA |
|
Linezolid |
≤2 |
- |
- |
1-2 |
NA |
NA |
NA |
NA |
NA |
|
Penicillin G |
≤ 0.12 |
- |
- |
0.015 |
NA |
NA |
NA |
NA |
NA |
|
Cefotaxime |
≤ 0.5 |
- |
- |
0.015-0.06 |
NA |
NA |
NA |
NA |
NA |
|
Clindamycin |
≤ 0.25 |
0.5 |
≥1 |
0.125- > 128 |
NA |
NA |
NA |
NA |
NA |
|
Erythromycin |
≤ 0.25 |
0.5 |
≥1 |
0.25-32 |
NA |
NA |
NA |
NA |
NA |
|
Levofloxacin |
≤2 |
4 |
≥8 |
0.5-8 |
NA |
NA |
NA |
NA |
NA |
|
Tetracycline |
≤2 |
4 |
≥8 |
0.25-8 |
NA |
NA |
NA |
NA |
NA |
|
Enterococcus faecalis (14) |
|
|
|
|
|
|
|
|
|
|
Tedizolid |
≤ 0.5 |
- |
- |
0.25-0.5 |
0.5 |
0.5 |
100 |
NA |
NA |
|
Linezolid |
≤2 |
4 |
≥8 |
1-2 |
2 |
2 |
100 |
0 |
0 |
|
Ampicillin |
≤8 |
- |
≥ 16 |
0.5-4 |
1 |
4 |
100 |
NA |
0 |
|
Erythromycin |
≤ 0.5 |
1-4 |
≥8 |
0.5- > 128 |
> 128 |
> 128 |
0 |
36 |
64 |
|
Levofloxacin |
≤2 |
4 |
≥8 |
1- > 128 |
1 |
128 |
64 |
0 |
36 |
|
Tetracycline |
≤4 |
8 |
≥ 16 |
0.5- > 128 |
64 |
128 |
14 |
0 |
86 |
|
Teicoplanin |
≤8 |
16 |
≥ 32 |
≤ 0.06-1 |
0.5 |
1 |
100 |
0 |
0 |
|
Vancomycin |
≤4 |
8-16 |
≥ 32 |
0.5-4 |
1 |
2 |
100 |
0 |
0 |
|
E. faecium (16) |
|
|
|
|
|
|
|
|
|
|
Tedizolid |
NA |
NA |
NA |
0.25-0.5 |
0.25 |
0.25 |
NA |
NA |
NA |
|
Linezolid |
≤2 |
4 |
≥8 |
0.5-2 |
2 |
2 |
100 |
0 |
0 |
|
Ampicillin |
≤8 |
- |
≥ 16 |
16- > 128 |
64 |
128 |
0 |
NA |
100 |
|
Erythromycin |
≤ 0.5 |
1-4 |
≥8 |
≤ 0.06- > 128 |
> 128 |
> 128 |
6 |
0 |
94 |
|
Levofloxacin |
≤2 |
4 |
≥8 |
32-128 |
128 |
128 |
0 |
0 |
100 |
|
Tetracycline |
≤4 |
8 |
≥ 16 |
0.25-128 |
0.5 |
128 |
56 |
0 |
44 |
|
Vancomycin |
≤4 |
8-16 |
≥ 32 |
1- > 128 |
1 |
> 128 |
56 |
0 |
44 |
|
Teicoplanin |
≤8 |
16 |
≥ 32 |
0.25-128 |
1 |
32 |
56 |
19 |
25 |
|
Viridans group Streptococcus spp. (10)‡
|
|
|
|
|
|
|
|
|
|
|
Tedizolid |
NA |
NA |
NA |
0.25-0.5 |
0.25 |
0.25 |
NA |
NA |
NA |
|
Linezolid |
≤2 |
- |
- |
1-2 |
1 |
2 |
100 |
NA |
NA |
|
Penicillin G |
≤ 0.12 |
0.25-2 |
≥4 |
0.03-2 |
0.06 |
0.5 |
70 |
10 |
0 |
|
Cefotaxime |
≤1 |
2 |
≥4 |
0.06-2 |
0.25 |
1 |
90 |
10 |
0 |
|
Clindamycin |
≤ 0.25 |
0.5 |
≥1 |
≤ 0.06- > 128 |
0.125 |
> 128 |
60 |
0 |
40 |
|
Erythromycin |
≤ 0.25 |
0.5 |
≥1 |
≤ 0.06- > 128 |
0.125 |
128 |
50 |
10 |
40 |
|
Levofloxacin |
≤2 |
4 |
≥8 |
0.5-2 |
1 |
2 |
100 |
0 |
0 |
|
Tetracycline |
≤2 |
4 |
≥8 |
0.25-64 |
16 |
64 |
40 |
0 |
60 |
|
Finegoldia magna (21) |
|
|
|
|
|
|
|
|
|
|
Tedizolid |
NA |
NA |
NA |
0.06-1 |
0.25 |
0.5 |
NA |
NA |
NA |
|
Linezolid |
NA |
NA |
NA |
0.5-2 |
2 |
2 |
NA |
NA |
NA |
|
Piperacillin |
≤ 32 |
64 |
≥ 128 |
≤ 0.06-0.25 |
0.125 |
0.25 |
100 |
0 |
0 |
|
Pip/tazobactam |
≤ 32 |
64 |
≥ 128 |
≤ 0.06-0.25 |
≤ 0.06 |
0.125 |
100 |
0 |
0 |
|
Cefoxitin |
≤ 16 |
32 |
≥ 64 |
0.125-2 |
1 |
1 |
100 |
0 |
0 |
|
Cefotetan |
≤ 16 |
32 |
≥ 64 |
0.25-2 |
1 |
2 |
100 |
0 |
0 |
|
Imipenem |
≤4 |
8 |
≥ 16 |
≤ 0.06-0.125 |
≤ 0.06 |
0.125 |
100 |
0 |
0 |
|
Clindamycin |
≤2 |
4 |
≥8 |
≤ 0.06- > 128 |
2 |
> 128 |
55 |
9 |
36 |
|
Metronidazole |
≤8 |
16 |
≥ 32 |
0.25-4 |
1 |
2 |
100 |
0 |
0 |
|
Vancomycin |
NA |
NA |
NA |
0.25-1 |
0.25 |
0.5 |
NA |
NA |
NA |
|
Peptostreptococcus spp. (27)§
|
|
|
|
|
|
|
|
|
|
|
Tedizolid |
NA |
NA |
NA |
≤ 0.06-0.25 |
0.125 |
0.25 |
NA |
NA |
NA |
|
Linezolid |
NA |
NA |
NA |
0.5-2 |
1 |
2 |
NA |
NA |
NA |
|
Piperacillin |
≤ 32 |
64 |
≥ 128 |
≤ 0.06-1 |
≤ 0.06 |
1 |
100 |
0 |
0 |
|
Pip/tazobactam |
≤ 32 |
64 |
≥ 128 |
≤ 0.06-1 |
≤ 0.06 |
0.25 |
100 |
0 |
0 |
|
Cefoxitin |
≤ 16 |
32 |
≥ 64 |
≤ 0.06-8 |
0.5 |
4 |
100 |
0 |
0 |
|
Cefotetan |
≤ 16 |
32 |
≥ 64 |
0.125-8 |
0.5 |
2 |
100 |
0 |
0 |
|
Imipenem |
≤4 |
8 |
≥ 16 |
≤ 0.06-0.5 |
≤ 0.06 |
0.125 |
100 |
0 |
0 |
|
Clindamycin |
≤2 |
4 |
≥8 |
≤ 0.06-128 |
0.25 |
128 |
74 |
4 |
22 |
|
Metronidazole |
≤8 |
16 |
≥ 32 |
0.5-2 |
1 |
2 |
100 |
0 |
0 |
|
Vancomycin |
NA |
NA |
NA |
0.125-1 |
0.25 |
1 |
NA |
NA |
NA |
|
Clostridium spp. (4)∥
|
|
|
|
|
|
|
|
|
|
|
Tedizolid |
NA |
NA |
NA |
0.25-0.5 |
NA |
NA |
NA |
NA |
NA |
|
Linezolid |
NA |
NA |
NA |
2-4 |
NA |
NA |
NA |
NA |
NA |
|
Piperacillin |
≤ 32 |
64 |
≥ 128 |
0.25-2 |
NA |
NA |
NA |
NA |
NA |
|
Pip/tazobactam |
≤ 32 |
64 |
≥ 128 |
0.125-2 |
NA |
NA |
NA |
NA |
NA |
|
Cefoxitin |
≤ 16 |
32 |
≥ 64 |
4-32 |
NA |
NA |
NA |
NA |
NA |
|
Cefotetan |
≤ 16 |
32 |
≥ 64 |
0.25-2 |
NA |
NA |
NA |
NA |
NA |
|
Imipenem |
≤4 |
8 |
≥ 16 |
0.25-2 |
NA |
NA |
NA |
NA |
NA |
|
Clindamycin |
≤2 |
4 |
≥8 |
0.125- > 128 |
NA |
NA |
NA |
NA |
NA |
|
Metronidazole |
≤8 |
16 |
≥ 32 |
0.5-8 |
NA |
NA |
NA |
NA |
NA |
|
Vancomycin |
NA |
NA |
NA |
0.5-4 |
NA |
NA |
NA |
NA |
NA |
Table 2
Comparative in vitro activities of tedizolid and other antimicrobial agents against bacteria recovered from patients with hospital-acquired pneumonia
|
Organism (N of isolates) and antimicrobial agents |
Breakpoint (µg/mL) |
MIC (µg/mL) |
Susceptibility (%) |
|
S |
I |
R |
Range |
50% |
90% |
S |
I |
R |
|
Methicillin-resistant Staphylococcus aureus (61) |
|
|
|
|
|
|
|
|
|
|
Tedizolid*
|
≤0.5 |
1 |
≥2 |
0.125-0.5 |
0.25 |
0.5 |
100 |
0 |
0 |
|
Linezolid |
≤4 |
- |
≥8 |
1-2 |
2 |
2 |
100 |
NA |
0 |
|
Erythromycin |
≤0.5 |
1-4 |
≥8 |
0.25- > 128 |
> 128 |
> 128 |
10 |
0 |
90 |
|
Clindamycin |
≤0.5 |
1-2 |
≥4 |
≤0.06- > 128 |
> 128 |
> 128 |
23 |
0 |
77 |
|
Cotrimoxazole |
≤2 |
- |
≥4 |
≤0.06-4 |
≤0.06 |
0.125 |
98 |
NA |
2 |
|
Gentamicin |
≤4 |
8 |
≥16 |
0.125-128 |
32 |
64 |
38 |
0 |
62 |
|
Levofloxacin |
≤1 |
2 |
≥4 |
0.25- > 128 |
32 |
32 |
16 |
0 |
84 |
|
Tetracycline |
≤4 |
8 |
≥16 |
0.25-128 |
128 |
128 |
18 |
0 |
82 |
|
Oxacillin |
≤2 |
- |
≥4 |
32- > 128 |
> 128 |
> 128 |
0 |
NA |
100 |
|
Vancomycin |
≤2 |
4-8 |
≥16 |
0.5-2 |
1 |
2 |
100 |
0 |
0 |
|
Methicillin-susceptible S. aureus (28) |
|
|
|
|
|
|
|
|
|
|
Tedizolid |
≤0.5 |
1 |
≥2 |
0.25-0.25 |
0.25 |
0.25 |
100 |
0 |
0 |
|
Linezolid |
≤4 |
- |
≥8 |
1-2 |
2 |
2 |
100 |
NA |
0 |
|
Erythromycin |
≤0.5 |
1-4 |
≥8 |
0.25- > 128 |
0.25 |
0.25 |
93 |
4 |
4 |
|
Clindamycin |
≤0.5 |
1-2 |
≥4 |
≤0.06-64 |
≤0.06 |
≤0.06 |
93 |
4 |
4 |
|
Cotrimoxazole |
≤2 |
- |
≥4 |
≤0.06-0.25 |
≤0.06 |
≤0.06 |
100 |
NA |
0 |
|
Gentamicin |
≤4 |
8 |
≥16 |
0.125-16 |
0.25 |
0.25 |
96 |
0 |
4 |
|
Levofloxacin |
≤1 |
2 |
≥4 |
0.125-8 |
0.25 |
1 |
93 |
0 |
7 |
|
Tetracycline |
≤4 |
8 |
≥16 |
0.25-0.25 |
0.25 |
0.25 |
100 |
0 |
0 |
|
Oxacillin |
≤2 |
- |
≥4 |
0.125-0.5 |
0.25 |
0.5 |
100 |
NA |
0 |
|
Vancomycin |
≤2 |
4-8 |
≥16 |
1-2 |
1 |
1 |
100 |
0 |
0 |
|
S. epidermidis (8) |
|
|
|
|
|
|
|
|
|
|
Tedizolid |
NA |
NA |
NA |
≤0.06 |
NA |
NA |
NA |
NA |
NA |
|
Linezolid |
≤4 |
- |
≥8 |
0.25 |
NA |
NA |
NA |
NA |
NA |
|
Erythromycin |
≤0.5 |
1-4 |
≥8 |
≤0.06-128 |
NA |
NA |
NA |
NA |
NA |
|
Clindamycin |
≤0.5 |
1-2 |
≥4 |
≤0.06- > 128 |
NA |
NA |
NA |
NA |
NA |
|
Cotrimoxazole |
≤2 |
- |
≥4 |
≤0.06-4 |
NA |
NA |
NA |
NA |
NA |
|
Gentamicin |
≤4 |
8 |
≥16 |
≤0.06-128 |
NA |
NA |
NA |
NA |
NA |
|
Levofloxacin |
≤1 |
2 |
≥4 |
4-128 |
NA |
NA |
NA |
NA |
NA |
|
Tetracycline |
≤4 |
8 |
≥16 |
0.125-32 |
NA |
NA |
NA |
NA |
NA |
|
Oxacillin |
≤0.25 |
- |
≥0.5 |
0.5-32 |
NA |
NA |
NA |
NA |
NA |
|
Vancomycin |
≤4 |
8-16 |
≥32 |
1-2 |
NA |
NA |
NA |
NA |
NA |
|
Streptococcus pneumoniae (47) |
|
|
|
|
|
|
|
|
|
|
Tedizolid |
NA |
NA |
NA |
0.25-0.5 |
0.25 |
0.5 |
NA |
NA |
NA |
|
Linezolid |
≤2 |
- |
- |
1-2 |
1 |
2 |
100 |
NA |
NA |
|
Penicillin G |
≤2 |
4 |
≥8 |
0.015-8 |
2 |
8 |
49 |
28 |
23 |
|
Cefotaxime |
≤1 |
2 |
≥4 |
0.015-32 |
1 |
32 |
55 |
26 |
19 |
|
Clindamycin |
≤0.25 |
0.5 |
≥1 |
0.125- > 128 |
> 128 |
> 128 |
15 |
0 |
85 |
|
Erythromycin |
≤0.25 |
0.5 |
≥1 |
0.25- > 128 |
> 128 |
> 128 |
6 |
0 |
94 |
|
Cotrimoxazole |
≤0.5 |
1-2 |
≥4 |
1-32 |
8 |
32 |
23 |
15 |
62 |
|
Levofloxacin |
≤2 |
4 |
≥8 |
2-128 |
2 |
32 |
72 |
2 |
26 |
|
Tetracycline |
≤1 |
2 |
≥4 |
0.25-128 |
32 |
64 |
13 |
0 |
87 |


 PDF
PDF ePub
ePub Citation
Citation Print
Print


 XML Download
XML Download