

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Clinical genetic testing plays an important role in evaluating patients with developmental delay (DD), mental retardation (MR), and autism spectrum disorders (ASD) with unknown etiology. DD indicates deficits in learning and adaptive functioning at the expected age. MR, often referred to as "intellectual disability", is a disorder with intellectual and adaptive deficits and can be diagnosed after the age of five years [1]. MR and DD affect 1-3% of general population [2]. ASD encompasses a group of disorders like autism, Asperger's syndrome, and pervasive developmental disorder. ASD shows features like impairment in social communication and interactions, and repetitive and restrictive behaviors [1]. The frequency of occurrence of ASD is approximately 1% of general population [1]. Genetic causes, including known genetic syndromes and chromosomal abnormalities, comprise the main etiology of these disorders. Approximately 17.4-47.1% of DD/MR and 10% of ASD can be explained by genetic causes [34].
The National Health Insurance system of the Republic of Korea only permits multiplex ligation-dependent probe amplification (MLPA) tests for four microdeletion syndromes (Prader-Willi/Angelman syndrome, DiGeorge syndrome, Miller-Dieker syndrome, and Williams syndrome), conventional cytogenetics, and FISH. Thus, the medical institutions in Korea cannot perform other diagnostic genetic tests. Conventional cytogenetics allows for detection of numerical and structural chromosomal abnormalities present in the entire genome, but has a limited resolution of 5-10 megabases (Mb). Thus, submicroscopic aberrations cannot be detected, and interpretation of the test results remains subjective. FISH and MLPA can detect specific cytogenetic aberrations with a higher sensitivity than conventional cytogenetics; however, they cannot cover entire regions of chromosomes. Thus, it takes substantial effort to detect abnormalities involving multiple regions, and the diagnostic yield is decreased when the clinical spectrum of the disease is variable. DD, MR, and ASD are difficult to define disease categories clinically owing to overlapping symptoms and comorbidities.
Chromosomal microarray (CMA) is now recommended worldwide as the first-tier clinical diagnostic test for patients with DD, MR, and ASD of unknown causes [5]. CMA detects copy number variations (CNVs) in the entire genome with a much higher resolution than conventional cytogenetics. Before the CMA test was adopted as a routine clinical diagnostic test, conventional cytogenetics and single gene tests such as fragile-X syndrome testing were done as initial tests for unexplained DD, MR, and ASD. However, the diagnostic yields of conventional cytogenetics and fragile-X syndrome testing in patients with DD/MR is below 3% and 1.2%, respectively [56]. CMA detects pathogenic CNVs with an average diagnostic yield of 12.2% in 33 previous studies involving 21,698 patients with neurodevelopmental disorders or multiple congenital anomalies [5].
We evaluated the utility of CMA as a routine clinical diagnostic test in the Korean population. In addition, we aimed to report a few interesting clinical cases confirmed by CMA test. We used Affymetrix single nucleotide polymorphism (SNP) array with an average resolution of 100 kb. The SNP array has been validated in a previous study indicating that it has sufficient resolution to detect single gene deletions [7]. Although CMA detects genomic imbalance with higher diagnostic yield than conventional cytogenetics, it cannot detect balanced rearrangements and low-level mosaicism [8]. Thus, we selected clinically affected individuals with normal karyotype.
Go to : 
METHODS
1. Patients
Genetic tests were requested by physicians from pediatrics, rehabilitation, neurology, and psychiatric departments for unexplained DD, MR, and ASD with or without dysmorphism or seizures. Written informed consent approved by institutional review board was obtained from patients or patients' parents for genetic analysis.
Conventional G-banded karyotype analysis from peripheral blood was performed as a part of initial screening tests, and 96 patients with normal karyotypes were included in this study. As we retrospectively performed CMA using the blood samples collected during MLPA studies, parental samples could not be obtained and were therefore, not available for analysis.
From March 2012 to April 2014, 96 patients with normal karyotype (67 males and 29 females, Table 1) were referred for further genetic testing. The median age at diagnosis was three years (range: 7 months-22 yr). Thirty four patients were ASD, 54 patients were DD and/or MR, and 8 patients were ASD combined with DD and/or MR (Table 1).
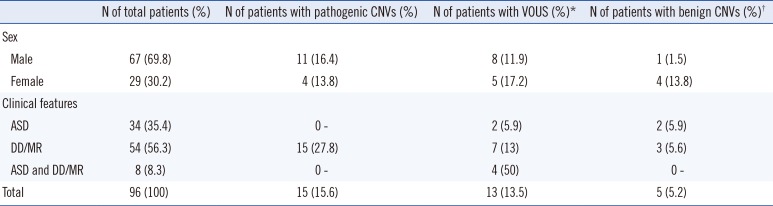
Table 1
Number of patients with copy number variations according to demographic and clinical features
![]()
2. DNA preparation
EDTA whole blood was used to extract DNA by using the Easy-DNA kit (Invitrogen Corporation, Carlsbad, CA, USA). The concentration and quality of genomic DNA was analyzed by Nanodrop ND-1000 (Thermo Scientific, Wilmington, DE, USA).
3. MLPA
Microdeletion syndromes were screened by using SALSA MLPA P245 Microdeletion Syndromes probemix (MRC-Holland, Amsterdam, The Netherlands) according to the manufacturer's instructions. The P245 probemix contains 49 different MLPA probes with amplification product sizes between 130 and 486 nucleotides. The probes target 40 causative genes implicated in 23 known microdeletion/microduplication syndromes. DNA was denatured at 98℃ for five minutes and hybridized with the probe set overnight at 60℃. Ligation reaction with ligase-65 enzyme was performed at 54℃ for 15 min, followed by five minutes at 98℃ for heat inactivation of the enzyme. PCR was performed with the specific SALSA PCR primers for 35 cycles (95℃ for 30 sec; 60℃ for 30 sec; 72℃ for one minute) by using the GeneAmp PCR System (Applied Biosystems, Foster City, CA, USA). MLPA fragment analysis data were generated by using the Applied Biosystems 3,500×L Genetic Analyzer (Applied Biosystems). The data were analyzed by using the GeneMarker software (SoftGenetics, State College, PA, USA). For confirmatory analysis of abnormal results found with the P245 screening probemix, an MLPA test with P372, P373, or P374 syndrome-specific probemix, or a P339 SHANK3 probemix (MRC-Holland) was performed by using the same protocol. Pathogenic CNVs detected by CMA that were smaller than 1 Mb were confirmed by using a P343 or P181 probemix.
4. Chromosomal microarray
CMA was performed with a CytoScan 750K array (Affymetrix, Santa Clara, CA, USA) according to the manufacturer's recommendations. The platform is composed of 550,000 non-polymorphic CNV probes and more than 200,000 SNP probes with an average resolution of 100 kb. The data were analyzed by using Chromosome Analysis Suite v2.1 Software (Affymetrix) and Nexus Copy Number v.7.5 Software (BioDiscovery, El Segundo, CA, USA). The February 2009 human reference sequence (GRCh37/Hg19) was used for genomic assembly.
5. Interpretation of detected CNVs
Detected CNVs were classified as pathogenic, benign, or variant of uncertain clinical significance (VOUS) in accordance with the recommended guidelines from the International Standard Cytogenomic Array and the American College of Medical Genetics [5910]. The data were interpreted by using information available in scientific literature, public databases and other general information about pathogenic or benign CNVs (size, content of Online Mendelian Inheritance in Man [OMIM] morbid genes or dosage sensitive genes, and type of dosage imbalance: duplication or deletion) [511]. Genomic map from the UCSC Genome Browser (http://genome.ucsc.edu/cgi-bin/hgGateway) was used to map the locations of CNVs and gene distribution. The Database of Genomic Variants (DGV, http://dgv.tcag.ca/dgv/app/home) provided catalogs of structural variations found in healthy controls. The dbVar (http://www.ncbi.nlm.nih.gov/dbvar/) database was also used to get information about CNVs from both normal and diseased populations. We also used the DatabasE of Chromosomal Imbalance and Phenotype in Humans using Ensembl Resources (DECIPHER, https://decipher.sanger.ac.uk/) as a reference for known microdeletion and microduplication syndromes, and the OMIM (http://omim.org/) for disease-causing genes, their functions and inheritance patterns.
Besides excluding pathogenic CNVs overlapping with known genomic imbalance syndromes and benign CNVs reported as normal variant in healthy controls, VOUS should meet at least one of the three criteria: the CNV is not a common polymorphism, OMIM genes in the CNV interval are not known for dosage sensitivity, and are not associated with patient's phenotypes.
Go to :
RESULTS
1. Results of MLPA and CMA
We identified 42 CNVs in 33/96 (34.4%) patients. Among these, 17 CNVs were classified as pathogenic (40.5%), 15 as VOUS (35.7%), and 10 as benign (23.8%). One or more pathogenic CNVs were reported in 15 patients (Table 1). Therefore the diagnostic yield of CMA was 15.6% (15/96) in our study. VOUS, excluding cases with pathogenic CNVs, were reported in 13/96 patients (13.5%). One or more benign CNVs, excluding cases with pathogenic CNVs and VOUS, were reported in five patients (5.2%).
Most of the 15 CNVs of unknown significance were not a common polymorphism, except a 2.3 kb-sized duplication at 8p23.2 found in three patients (Table 2, Case 20, 21, and 22). The duplicated region, which includes CSMD1 (MIM 608397) gene, was also found in normal controls [12]. CSMD1 was shown to be interrupted by duplication in a patient with speech delay and autism in a previous study [13].
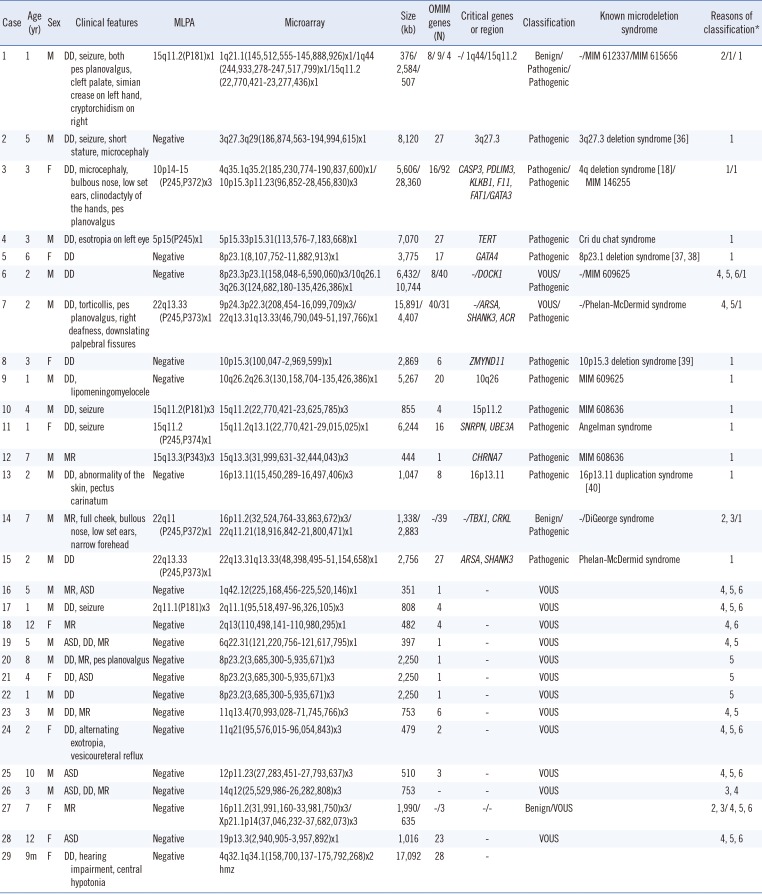
Table 2
Summary of clinical features and genetic test results of patients with copy number variants or loss of heterozygosity
| Case | Age (yr) | Sex | Clinical features | MLPA | Microarray | Size (kb) | OMIM genes (N) | Critical genes or region | Classification | Known microdeletion syndrome | Reasons of classification* |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1 | M | DD, seizure, both pes planovalgus, cleft palate, simian crease on left hand, cryptorchidism on right | 15q11.2(P181)x1 | 1q21.1(145,512,555-145,888,926)x1/1q44 | 376/2,584/507 | 8/ 9/ 4 | -/ 1q44/15q11.2 | Benign/Pathogenic/Pathogenic | -/MIM 612337/MIM 615656 | 2/1/ 1 |
| (244,933,278-247,517,799)x1/15q11.2 | |||||||||||
| (22,770,421-23,277,436)x1 | |||||||||||
| 2 | 5 | M | DD, seizure, short stature, microcephaly | Negative | 3q27.3q29(186,874,563-194,994,615)x1 | 8,120 | 27 | 3q27.3 | Pathogenic | 3q27.3 deletion syndrome [36] | 1 |
| 3 | 3 | F | DD, microcephaly, bulbous nose, low set ears, clinodactyly of the hands, pes planovalgus | 10p14-15 (P245,P372)x3 | 4q35.1q35.2(185,230,774-190,837,600)x1/ | 5,606/28,360 | 16/92 | CASP3, PDLIM3, KLKB1, F11, FAT1/GATA3 | Pathogenic/Pathogenic | 4q deletion syndrome [18]/MIM 146255 | 1/1 |
| 10p15.3p11.23(96,852-28,456,830)x3 | |||||||||||
| 4 | 3 | M | DD, esotropia on left eye | 5p15(P245)x1 | 5p15.33p15.31(113,576-7,183,668)x1 | 7,070 | 27 | TERT | Pathogenic | Cri du chat syndrome | 1 |
| 5 | 6 | F | DD | Negative | 8p23.1(8,107,752-11,882,913)x1 | 3,775 | 17 | GATA4 | Pathogenic | 8p23.1 deletion syndrome [3738] | 1 |
| 6 | 2 | M | DD | Negative | 8p23.3p23.1(158,048-6,590,060)x3/10q26.1 | 6,432/10,744 | 8/40 | -/DOCK1 | VOUS/Pathogenic | -/MIM 609625 | 4, 5, 6/1 |
| 3q26.3(124,682,180-135,426,386)x1 | |||||||||||
| 7 | 2 | M | DD, torticollis, pes planovalgus, right deafness, downslating palpebral fissures | 22q13.33 (P245,P373)x1 | 9p24.3p22.3(208,454-16,099,709)x3/ | 15,891/4,407 | 40/31 | -/ARSA, SHANK3, ACR | VOUS/Pathogenic | -/Phelan-McDermid syndrome | 4, 5/1 |
| 22q13.31q13.33(46,790,049-51,197,766)x1 | |||||||||||
| 8 | 3 | F | DD | Negative | 10p15.3(100,047-2,969,599)x1 | 2,869 | 6 | ZMYND11 | Pathogenic | 10p15.3 deletion syndrome [39] | 1 |
| 9 | 1 | M | DD, lipomeningomyelocele | Negative | 10q26.2q26.3(130,158,704-135,426,386)x1 | 5,267 | 20 | 10q26 | Pathogenic | MIM 609625 | 1 |
| 10 | 4 | M | DD, seizure | 15q11.2(P181)x3 | 15q11.2(22,770,421-23,625,785)x3 | 855 | 4 | 15p11.2 | Pathogenic | MIM 608636 | 1 |
| 11 | 1 | F | DD, seizure | 15q11.2(P245,P374)x1 | 15q11.2q13.1(22,770,421-29,015,025)x1 | 6,244 | 16 | SNRPN, UBE3A | Pathogenic | Angelman syndrome | 1 |
| 12 | 7 | M | MR | 15q13.3(P343)x3 | 15q13.3(31,999,631-32,444,043)x3 | 444 | 1 | CHRNA7 | Pathogenic | MIM 608636 | 1 |
| 13 | 2 | M | DD, abnormality of the skin, pectus carinatum | Negative | 16p13.11(15,450,289-16,497,406)x3 | 1,047 | 8 | 16p13.11 | Pathogenic | 16p13.11 duplication syndrome [40] | 1 |
| 14 | 7 | M | MR, full cheek, bullous nose, low set ears, narrow forehead | 22q11(P245,P372)x1 | 16p11.2(32,524,764-33,863,672)x3/ | 1,338/2,883 | -/39 | -/TBX1, CRKL | Benign/Pathogenic | -/DiGeorge syndrome | 2, 3/1 |
| 22q11.21(18,916,842-21,800,471)x1 | |||||||||||
| 15 | 2 | M | DD | 22q13.33(P245,P373)x1 | 22q13.31q13.33(48,398,495-51,154,658)x1 | 2,756 | 27 | ARSA, SHANK3 | Pathogenic | Phelan-McDermid syndrome | 1 |
| 16 | 5 | M | MR, ASD | Negative | 1q42.12(225,168,456-225,520,146)x1 | 351 | 1 | - | VOUS | 4, 5, 6 | |
| 17 | 1 | M | DD, seizure | 2q11.1(P181)x3 | 2q11.1(95,518,497-96,326,105)x3 | 808 | 4 | VOUS | 4, 5, 6 | ||
| 18 | 12 | F | MR | Negative | 2q13(110,498,141-110,980,295)x1 | 482 | 4 | - | VOUS | 4, 6 | |
| 19 | 5 | M | ASD, DD, MR | Negative | 6q22.31(121,220,756-121,617,795)x1 | 397 | 1 | - | VOUS | 4, 5 | |
| 20 | 8 | M | DD, MR, pes planovalgus | Negative | 8p23.2(3,685,300-5,935,671)x3 | 2,250 | 1 | - | VOUS | 5 | |
| 21 | 4 | F | DD, ASD | Negative | 8p23.2(3,685,300-5,935,671)x3 | 2,250 | 1 | - | VOUS | 5 | |
| 22 | 1 | M | DD | Negative | 8p23.2(3,685,300-5,935,671)x3 | 2,250 | 1 | - | VOUS | 5 | |
| 23 | 3 | M | DD, MR | Negative | 11q13.4(70,993,028-71,745,766)x3 | 753 | 6 | - | VOUS | 4, 5 | |
| 24 | 2 | F | DD, alternating exotropia, vesicoureteral reflux | Negative | 11q21(95,576,015-96,054,843)x3 | 479 | 2 | - | VOUS | 4, 5, 6 | |
| 25 | 10 | M | ASD | Negative | 12p11.23(27,283,451-27,793,637)x3 | 510 | 3 | - | VOUS | 4, 5, 6 | |
| 26 | 3 | M | ASD, DD, MR | Negative | 14q12(25,529,986-26,282,808)x3 | 753 | - | - | VOUS | 3, 4 | |
| 27 | 7 | F | MR | Negative | 16p11.2(31,991,160-33,981,750)x3/ | 1,990/635 | -/3 | -/- | Benign/VOUS | 2, 3/ 4, 5, 6 | |
| Xp21.1p14(37,046,232-37,682,073)x3 | |||||||||||
| 28 | 12 | F | ASD | Negative | 19p13.3(2,940,905-3,957,892)x1 | 1,016 | 23 | - | VOUS | 4, 5, 6 | |
| 29 | 9m | F | DD, hearing impairment, central hypotonia | Negative | 4q32.1q34.1(158,700,137-175,792,268)x2 | 17,092 | 28 | - | |||
| hmz |
*1.Overlapping with a known genomic imbalance syndrome; 2. In the category of genomic imbalance in healthy individuals as per public database; 3. No OMIM genes in the CNV interval; 4. CNV is not a common polymorphism; 5. OMIM genes in the CNV interval are not known for dosage sensitivity; 6. OMIM genes in the CNV interval are not associated with patient's phenotype.
Abbreviations: MLPA, multiplex ligation-dependent probe amplification; VOUS, variant of uncertain clinical significance; ASD, autism spectrum disorder; DD, developmental delay; MR, mental retardation; m, months.
![]()
One patient showed a deletion in 2q13 (Case 18), which included four OMIM genes (RGPD6, RGPD5, MALL, and NPHP1). The four genes are not known to have any relation with this patient's phenotype, but homozygous deletion of NPHP1 (MIM 607100) is known to be associated with nephronophthisis [14]. TBC1D32 gene (MIM 615867) was deleted in one patient (Case 19). TBC1D32 has been reported to be mutated in a patient with multiple congenital anomalies [15]. A duplication at 11q13.4 in a patient (Case 23) includes six OMIM genes (DHCR7, NADSYN1, KRTAP5-9, FAM86C1, IL18BP, and NUMA1). Mutation of DHCR7 gene is associated with Smith-Lemli-Opitz syndrome (SLOS, MIM 270400), which is an autosomal recessive multiple congenital anomaly and intellectual disability syndrome [16]. Thus far, the only reported DHCR7 mutations associated with SLOS are point mutations or multiple exonic deletions [1617]. Thus, it is difficult to interpret the significance of duplication in our patient. A 753 kb-sized duplication at 14q12 in a patient (Case 26) contains no OMIM gene, so the CNV is likely to have a benign nature. However, we interpreted it as VOUS because the duplicated region was not reported in databases for control population [9].
Pathogenic CNVs were identified in 27.8% patients with DD and/or MR (Table 1). No pathogenic CNVs were seen in patients with ASD and ASD combined with DD and/or MR in our study. The size range of the pathogenic CNVs was 444 kb to 28.4 Mb. Most of the pathogenic CNVs (94.1%) were above 500 kb (Table 3). Six CNVs between 5-10 Mb and three CNVs above 10 Mb were not detected by conventional cytogenetics. All benign CNVs were below 5 Mb (Table 3).
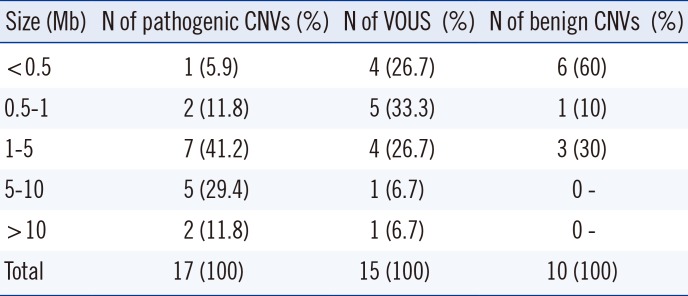
Table 3
Size distribution of pathogenic CNVs found in patients
![]()
MLPA microdeletion syndrome screening probemix for 23 chromosomal disorders detected six patients with known microdeletion or microduplication syndromes with a diagnostic yield of 6.3%. There were one patient with Angelman syndrome and one with DiGeorge syndrome. Therefore, the diagnostic yield of four microdeletion syndromes designated by National Health Insurance system in Korea was 2.1%.
2. Clinical case reports
1) Hypoparathyroidism, sensorineural deafness, and renal dysplasia syndrome
A 3-yr-old female (Table 2, Case 3) was referred for evaluation of developmental delay. G-banded karyotype was normal, while CMA revealed a 5.6 Mb deletion at 4q35.1q35.2 region and a 28.4 Mb duplication at 10p15.3p11.2 region.
Chromosome 4q deletion is known to be associated with intellectual disability, ASD, and craniofacial dysmorphism [18]. The critical region for ASD phenotype, containing MTNR1A, FAT1, and F11 at 4q35.2 [18], is identical to that in our patient. Duplication of GATA3 gene at 10p14 can cause hypoparathyroidism, sensorineural deafness, and renal dysplasia syndrome (HDR syndrome, MIM 146255) [19]. DD and facial dysmorphism have also been described in a HDR syndrome patient [19]. A previous study reported unbalanced cryptic translocation der(4)(4;10)(q35;p15), similar to our case [20]. Parental study revealed that the genomic imbalance was originated from unbalanced segregation of maternal balanced reciprocal translocation t(4;10)(q35;p15) [20]. Both patients showed learning disabilities, facial dysmorphisms, and immunodeficiency [20]. Our patient's karyotype was initially interpreted as normal, however, after CMA results, a more detailed karyotype analysis revealed der(4)(4;10)(q35;p15), as previously described [20].
There were three patients with cryptic unbalanced translocations involving two chromosomes in our study (Case 3, 6, and 7), suggesting inheritance from parental balanced translocation. In these cases, other family members were given genetic evaluation and proper counseling about the disorders and the recurrence risk in family [9].
2) Patient with a region of homozygosity on chromosome 4
A 9-month-old female (Table 2, Case 29) was evaluated for delayed development due to central hypotonia. CMA showed no CNV, but there was one 17.1-Mb region of homozygosity (ROH) on chromosome 4.
SNP-based array, unlike array-based CGH, can identify copy-number changes as well as ROH, which indicates uniparental disomy (UPD) or identity by descent (IBD) [21]. When the ROHs exist on multiple chromosomes, they usually suggest IBD, i.e. inheritance from a common ancestor [22]. In contrast, UPD is suspected when the large ROH is on a single chromosome [22]. ROH may have pathogenic implications in two ways: if there are imprinted genes within the region, or if it leads to homozygosity for deleterious alleles involved in autosomal recessive disorders [23]. In our case, 28 OMIM genes map to this 17.1 Mb ROH on chromosome 4. Previous reports included chromosome 4 UPD in a patient with mental disorder [23] and an interstitial deletion at 4q32q34, a region that overlaps with our case, in a patient with DD and dysmorphism [24]. However, multiple ROHs can be detected in a normal population. Therefore, caution should be exercised when reporting and interpreting ROH [22]. A parental study and genetic counseling should be recommended in this instance.
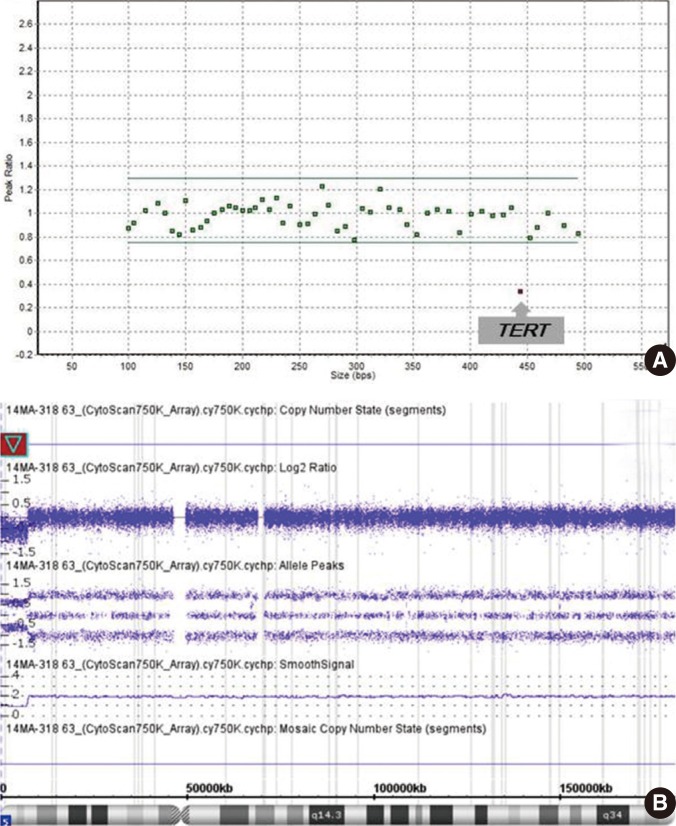
3) Cri du chat syndrome
A 3-yr-old male (Table 2, Case 4) visited the psychiatric department for speech delay. He also had esotropia in his left eye and was diagnosed as having DD. MLPA with P245 probemix revealed deletion in only one probe site on exon 3 of TERT gene (Fig. 1A), which is known to be involved in the phenotype of cri du chat syndrome (MIM 123450). CMA showed a deletion at 5p15.33p15.31(113,576-7,183,668) (Fig. 1B), confirming the MLPA result. A decreased signal for only one probe in MLPA experiment can indicate a false-positive result owing to polymorphism in the probe ligation site [25]. Therefore, confirmation of MLPA finding by another method is essential in such cases [25]. The region involved in the cri du chat syndrome is known to be variable in size, and it can be a terminal or an interstitial deletion [26]; so confirmative tests like CMA can be of help.
Go to :
DISCUSSION
We conducted CMA analysis in 96 unexplained DD, MR, and ASD patients with normal karyotype as assessed by conventional cytogenetics. The diagnostic yield of CMA was 15.6%, which is higher than the average rate from previous reports including chromosomal aneuploidies (12.2%) [5]. Our finding supports the necessity of implementing CMA as a routine diagnostic test in the Korean population. Moreover, first-tier use of CMA for clinical genetic evaluation of unexplained DD, MR, and ASD in the Korean population could be beneficial for patients, considering the cost-effectiveness of CMA compared with current conventional cytogenetics and MLPA or FISH test strategy [272829]. Owing to the significantly higher diagnostic yield of CMA (CMA 15.6% vs. MLPA for the four microdeletion syndromes 2.1%), an additional 13.5% of patients with genetic etiology can be diagnosed through initial CMA testing and can save much time, cost, and effort from additional diagnostic tests.
Although we found no pathogenic CNV in patients with ASD and ASD combined with DD/MR, the possibility of later onset of symptoms of autistic features in these patients has to be considered, with regard to the previous findings about high frequency of pathogenic CNVs in ASD patients [13031].
It is known that the size of CNV is of limited importance in interpretation of pathogenicity [9]. The size distribution of pathogenic CNVs varied a lot in this study. Pathogenic CNVs greater than 5 Mb were missed by conventional cytogenetics in six cases (Cases 2, 3, 4, 6, 9, and 11). One patient (Case 3) had a terminal deletion on chromosome 4 and a terminal duplication on chromosome 10. Initially, the karyotype of the patient was interpreted as normal; however, after referring to the CMA results, a reanalysis of the karyotype revealed der(4)(4;10)(q35;p15). Case 11 with Angelman syndrome had a 6 Mb-sized deletion downstream of the centromere. Four of these six cases (Cases 2, 4, 6, and 9) involved a terminal deletion. Although 5-6 Mb is usually considered to be the detection limit of conventional G-banded karyotyping, some cases, such as chromosome abnormalities involving terminal or near-centromere regions, can be missed [11].
Among our cases, two patients (2/96, 2.1%) were diagnosed as having Phelan-McDermid syndrome (MIM 606232). These two patients had deletions in 22q13 region, involving ARSA and SHANK3 loci (Cases 7 and 15). Haploinsufficiency of the SHANK3 product is known to have a causative role in neurologic symptoms in Phelan-McDermid syndrome [32]. Deletions, translocations, or point mutations involving SHANK3 locus have been reported as pathogenic in ASD/DD [323334]. Higher frequency of CNVs involving SHANK3 was reported in Chinese patients (1.7%), compared with 20 studies of European, American, and Australian populations (0.24%) [34]. The prevalence of imbalance involving SHANK3 in our study (2.1%) was also higher than that reported in a previous study of Caucasian population (0.24%) [34], suggesting higher frequency of Phelan-McDermid syndrome in DD/MR/ASD patients among East Asians.
The result of a parental study [5] is one of the most useful evidences of clinical significance of CNVs found in a patient. The interpretation of VOUS can be helped from the information whether it is inherited from a healthy parent or if it occurred de novo in the proband [5]. The absence of parental analysis is a limitation of our study. Although we could not validate VOUS with a parental study and only included patients with normal karyotype, the detection rate of pathogenic CNVs in our study was higher than that in previous reports [5]. Parental studies will help not only the interpretation of clinical significance of CNVs, but also the genetic counseling and evaluation of recurrence risk of the genetic abnormality in families, when CMA is available as a routine diagnostic test in future in Korea.
One major obstacle in implementing CMA as a routine diagnostic test is the current introduction system for medical technology in Korea [35]. All new diagnostic tests, including genetic tests, must go through a unified regulatory process. It is possible to apply to New Health Technology Assessment of Health Insurance Review & Assessment Service for a new medical device after getting permission from Ministry of Food and Drug Safety in Korea. Rapidly changing technology in clinical genomic testing requires a flexible system for assessing newly introduced medical procedures and health technology.
Go to :
 XML Download
XML Download