

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor
Down syndrome (DS) patients exhibit a 50-fold increase in acute leukemia incidence during the first five years of life, compared with those without DS. Trisomy 21, with or without other cytogenetic abnormalities, is reported in ~3% of AML and MDS cases; however, tetrasomy 21 and pentasomy 21 are unusual [1, 2]. Isodicentric chromosome 21 is a rare but recurrent cytogenetic abnormality in acute leukemia patients [3]; however, pentasomy 21q with two isochromosome 21s is very rare and has not yet been reported in pediatric DS patients with acute megakaryoblastic leukemia (AMKL).
Here, we report a first case of 19-month-old girl diagnosed as having DS, who was later diagnosed as having AMKL with pentasomy 21. The patient was admitted at 14 months of age, because bicytopenia was detected during a routine visit. Complete blood count (CBC) revealed the followings: Hb 8.6 g/dL; white blood cell (WBC) count, 4.6×109/L; and platelet count, 27×109/L. Peripheral blood smear showed anisopoikilocytosis with some elliptocytes and dacrocytes. DS was diagnosed at birth, and the patient's kayotype was 46,XX,+21c,der(21;21)(q10;q10)c. Although an attempted bone marrow aspiration resulted in a "dry tap," a needle biopsy specimen showed moderate fibrosis and megakaryocytic hyperplasia (4.9/high power field) with dysmegakaryocytic features. She was diagnosed as having transient myeloproliferative disorder, received one unit of packed red blood cells, and was subsequently discharged.
Five months later, a follow-up CBC revealed leukoerythroblastic reaction, and a physical examination revealed hepatosplenomegaly. Bone marrow study revealed persistent megakaryocytic hyperplasia and grade 3 fibrosis (Fig. 1). Cytogenetic analysis revealed a 49,XX,+11,+19,+21c,der(21;21)(q10;q10)c,+der (21;21)[19]/46,XX,+21c,der(21;21)c[9] karyotype, per the International System for Human Cytogenetic Nomenclature (ISCN) 2013. FISH confirmed pentasomy 21 (Fig. 2). JAK2 mutation and BCR/ABL fusion were not detected. She received conservative therapy, and one month later, the disease progressed such that the peripheral blood presented 15% blasts. The patient was transferred to another hospital where she was diagnosed as having DS-associated AML. The blast count was 30% on the bone marrow aspirate, and the immunophenotype of the neoplastic cells was characteristic of megakaryoblasts: CD13+, CD33+, CD34+, CD64w+, CD117+, CD41w+, CD7+, HLA-DR+, MPO-, and nTdT-. GATA1 mutation was not detected; however, an additional trisomy 11-associated MLL gain was detected by FISH. Calreticulin gene mutation test was not performed. The patient underwent cytarabine plus daunorubicin induction chemotherapy but failed to respond to the treatment and expired six months later.
 | Fig. 1(A) Bone marrow needle biopsy specimen, showing grade 3 fibrosis (H&E stain, ×100). (B) Reticulin staining showing grade 3 fibrosis (Reticulin stain, ×200).
|
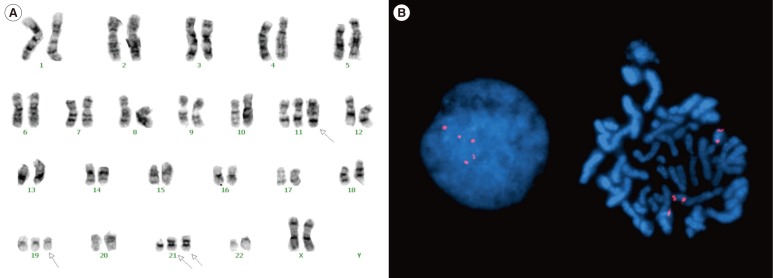 | Fig. 2Patient with Down syndrome exhibiting primary myelofibrosis with pentasomy 21. (A) Karyogram (Karyotype: 49,XX,+11,+19, +21c,der(21;21)(q10;q10)c, +der(21;21)[19]/46,XX,+21c,der(21;21)(q10;q10)c[9]. Arrows indicate abnormal chromosomes of 11, 19, and 21. (B) FISH analysis with a locus-specific probe for 21q22.13-q22.2, revealing pentasomy 21.
|
We identified pentasomy 21 with two isochromosome 21s in DS-associated transient abnormal myeloproliferative disorder, which was later transformed into AMKL. Transient myeloproliferative disorder occurs in ~10% of newborns with DS, and non-transient AML develops one to three years later in ~20-30% of such cases [4]. Fifty percent of cases of DS-associated acute leukemia are usually AMKL. In -70% of AMKL cases preceded by a pre-leukemic phase, which is characterized by thrombocytopenia and dysplastic changes, and often accompanied by marrow fibrosis, the disease may last several months or even years [5]. The present patient showed a similar disease course, transforming eventually into AMKL a few months later. Trisomy 19 that was observed in this patient might be due to some unknown role played by the leukemic transformation, as the most common abnormality in AMKL [6], and in the AKT2, cyclin E, and MLL2 genes in the 19q12 region, which have been implicated in solid tumors and are under investigation in hematologic malignancies [7].
Genes on chromosome 21 play an important role in leukemogenesis [8]. One gene --RUNX1(AML1) at 21q22-- plays a crucial role in hematopoiesis during embryonic development, and is frequently involved in chromosomal rearrangements observed in various myeloid malignancies [9]. Isochromosome 21q, formed as idic(21)(p10;p10), could result in an increased gene copy number on the entire long arm of chromosome 21 [10]. Furthermore, the duplication of idic(21)(p10;p10) gave rise to pentasomy 21q and to amplification of oncogenes at 21q, such as RUNX, ETS, and ERG, which may be involved in the development of leukemia. Moreover, the MLL gene gain due to trisomy 11, might be associated with the poor prognosis in this particular patient. To date, 16 cases of pentasomy 21 with two isochromosomes have been reported in hematologic malignancies, but the clinical features common to these cases are unknown [3].
This case shows us that hematologic surveillance of peripheral blood is needed in DS newborns, and close follow-up as well as optimal molecular and cytogenetic studies should be performed in cases with abnormal peripheral blood findings. Clarification of the mechanism underlying myelofibrosis and leukemogenesis in pentasomy 21q with two isochromosomes, in myeloid leukemia associated with DS, requires further studies.
 XML Download
XML Download