

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare, life-threatening hemolytic disease, affecting only 1-2 persons per million worldwide; in Korea, there are about 300 reported patients [1]. PNH is caused by the absence of glycosylphosphatidylinositol (GPI)-linked proteins, due to phosphatidylinositol glycan A (PIG-A) gene mutation, rendering cells vulnerable to complement attack [2, 3, 4], especially in acidic blood ensued by sleep with shallow respiration [5]. Unlike mutations in normal, healthy individuals, the PIG-A mutation in PNH occurs in an affected multipotent hematopoietic stem cells [6]. With expansion of this mutant clone, PNH is characterized by chronic complement-mediated hemolytic anemia, hemoglobinuria, thrombosis in unusual locations, acquired bone marrow failure, and relatively low risk of myelodysplastic syndrome or leukemia [7, 8].
Traditionally, the Ham test, using acidified serum as proposed in 1937 [9], and the sucrose hemolysis test, incubating blood in hypotonic sucrose solution [10], were used to diagnose PNH, although the sensitivities and specificities of examinations by spectrophotometry are quite low. Over the past several years, evaluation by flow cytometry of GPI-anchored proteins (CD55, CD59) of red blood cells (RBC) and granulocytes has become the gold standard for PNH diagnosis [11, 12, 13]; however, this approach has not been adopted by all laboratories, and hematology specialists are required for opportune diagnosis, which otherwise could be difficult to be established for a prolonged period of up to months or years.
Hence, it is of critical importance to introduce an expedient and facilitated measure for PNH diagnosis. This need is further enforced by the following considerations: the median survival of PNH patients is approximately 10 yr, the 5-yr mortality rate is about 35%, and the treatment with the Food and Drug Administration (FDA)-approved eculizumab (Soliris; Alexion Pharmaceuticals, Inc., Cheshire, CT, USA) for PNH is expected to considerably improve the five-year survival rate for patients, in addition to alleviating symptoms [11, 14, 15, 16, 17].
We aimed to develop a measure by which PNH could be screened using data gathered from routine complete blood count (CBC) tests. Our study was driven by two observations: 1) PNH cells are more damaged than normal cells in acidic conditions, in which complements are activated, and 2) since the reagents used for measuring reticulocytes in a Coulter DxH800 (Beckman Coulter, Miami, FL, USA) are acidic and hypotonic, PNH cells should show different assay data than normal cells. On the basis of the routine parameters and research use only (RUO) parameters from the DxH800, the authors aimed to create a new screening marker for PNH composed of the fewest parameters, but offering the most discriminative power.
Go to : 
METHODS
1. Study population
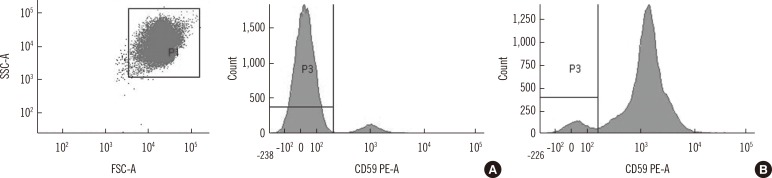
We analyzed 979 CBC data from 963 patients. The CBC data include data from both PNH patients (57 samples from 44 PNH patients) and those receiving CBC exams for anemia, malignancy, infection, or health check-ups at Seoul St. Mary's Hospital, Korea, between December 2012 and July 2014. In the selected population, we followed the standard criteria for the PNH assay. Flow cytometry for CD55 and CD59 on RBCs was performed to quantitate type I (normal expression), type II (partial deficiency), and type III (complete deficiency) PNH clones to a detection level of 1%. PNH clones in granulocytes were detected using fluorescent aerolysin [12] for CD24 and CD15 to a detection level of 0.1%. In addition to the PNH patients, aplastic anemia and myelodysplastic syndrome were also confirmed by flow cytometry to rule out PNH clones.
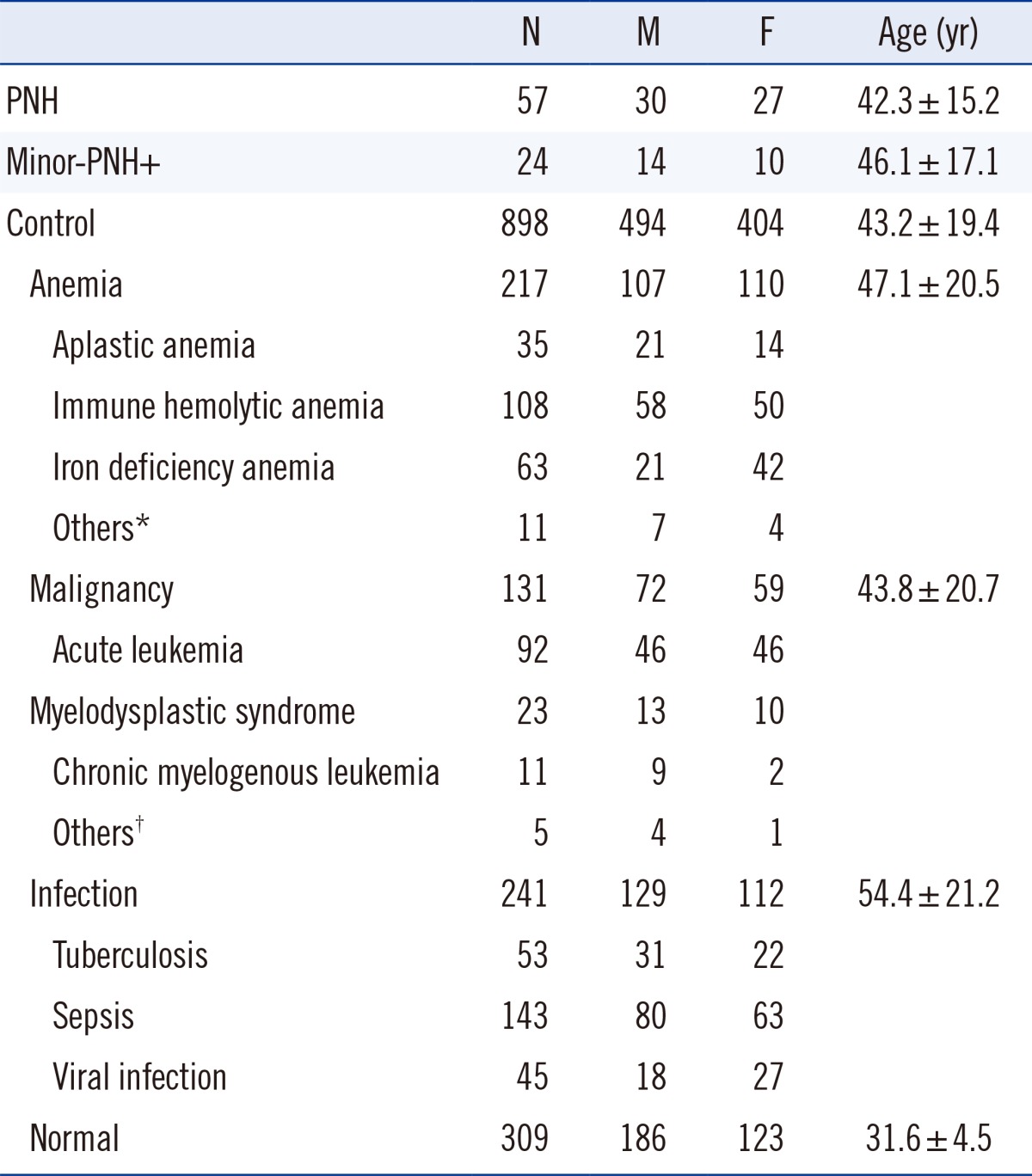
When the PNH-positive clone population was less than 5% of RBC and/or granulocyte counts (Fig. 1), the change of cell population data was expected to be less than 5%. Hence, it was considered that if these samples were treated as the overt cases with more than 5% of PNH clones, noise in the data might occur in establishing the screening marker. To avoid such noise, we classified and analyzed such samples as "PNH minor clone-positive samples" (minor-PNH+). There were 24 minor-PNH+ in the present study population. To ensure minimal sample bias, any two data from the same patient had a minimum test interval of one year between them. Excluding the PNH and minor-PNH+ patients, the remaining study population (control group) was composed of four subgroups: anemia, malignancy, infection, and normal. The specific diseases and the patients' characteristics for each group are shown in Table 1. This study was approved by The Catholic Medical Center institutional review board.
2. Establishment and analysis of the new markers
1) Selecting the parameters
Considering the characteristics of PNH, we examined 43 parameters in total: five basic CBC parameters such as hemoglobin, mean corpuscular volume (MCV), mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration, RBC distribution width; four reticulocyte-related parameters such as reticulocyte number and percent, mean reticulocyte volume (MRV), immature reticulocyte fraction (IRF); and 34 RUO parameters such as low hemoglobin density, microcytic anemia factor, mean sphered cell volume (MSCV), high light scattering reticulocyte, RBC size factor, reticulocyte distribution width (RDWR), and 28 volume/conductivity/light scatter (VCS) parameters [MN-V-RET, SD-V-RET, MN-C-RET, SD-C-RET, MN-AL2-RET, SD-AL2-RET, MN-MALS-RET, SD-MALS-RET, MN-UMALS-RET, SD-UMALS-RET, MN-LMALS-RET, SD-LMALS-RET, MN-LALS-RET, SD-LALS-RET, MN-V-NRET, SD-V-NRET, MN-C-NRET, SD-C-NRET, MN-AL2-NRET, SD-AL2-NRET, MN-MALS-NRET, SD-MALS-NRET, MN-UMALS-NRET, SD-UMALS-NRET, MN-LMALS-NRET, SD-LMALS-NRET, MN-LALS-NRET, and SD-LALS-NRET]. Each parametric data measured was sorted in increasing order of values. We manually tried to identify parameters that exhibited a comparatively distinct demarcation between PNH and non-PNH groups.
2) Establishing cutoff values
The whole samples were divided into two sets: test and validation, to find optimal cutoff values to rule out any interference originating from device conditions, especially from the laser [18]. All sample data were first organized by disease, and each disease group was subsequently sorted in chronological order. Each chronologically-ordered disease group was then divided into two sets: a test set and a validation set. The former included those samples that were placed in odd number positions in the ordered group, whereas the latter included the samples in even number positions. For each identified parameter, a cutoff value was sought that would include the maximum number of PNH patients and the minimum number of non-PNH patients. Establishing cutoff values involved manual sorting of parameter values in Excel in either decreasing or increasing order. A value was considered as a cutoff, if it would mark the most number of PNH samples and the least number of control samples. With the collected cutoff values, we fine-tuned the values to achieve a minimum of 90% sensitivity and specificity. Flow cytometry results were considered as truth values. The marker range set, obtained as described above, was subsequently applied to the validation set to verify its validity.
3. Statistical analysis
We used Student's t-test or ANOVA to test differences in the means of hematologic parameters between groups and Spearman's coefficient of rank sum test to find any correlation between PNH cell counts and each parameter. All statistical analyses including specificity, sensitivity, positive predictive value (PPV), and negative predictive value (NPV) were performed using SPSS 20.0 (SPSS Inc., Chicago, IL, USA). The confidence interval (CI) was set to 95%, and P value less than 0.05 was considered statistically significant.
Go to :
RESULTS
Table 2 shows the mean value of each of five parameters, which exhibits a distinct demarcation between PNH patients and non-PNH patients. A significant difference was found for each of the five parameters between the PNH and control groups (P<0.001). Except for the normal group within the control subgroups, the anemia, malignancy, and infection subgroups all showed a significant difference in the five parameters (P<0.001). In the normal subgroup, only RDWR showed an insignificant difference with the PNH group (P=0.405).

Table 2
Selected parameters in each group (mean ± SD)
P values were provided when compared with PNH group.
Abbreviations: PNH, paroxysmal nocturnal hemoglobinuria; MRV, mean reticulocyte volume; RDWR, reticulocyte distribution width; MSCV, mean sphered cell volume; MN-AL2-NRET, measuring mature RBC volume in the reticulocyte channel by light scattering; IRF, immature reticulocyte fraction.
![]()
When these parameters are applied as a set, the cutoff values that ensured at least 90% specificity and 85% sensitivity are shown below:
Followings are brief explanations for each of the selected parameters: MRV (fL) is the mean volume of all reticulocyte-events; RDWR is the size distribution of reticulocytes expressed as coefficient variation of width; MSCV (fL) is mean sphered cell volume of RBCs derived as a side effect from preparation for reticulocyte measurement; MN-AL2-NRET is mean of RBC volume measured by axial light loss in the reticulocyte channel; and IRF is a percentage of the count of the highest light scatter reticulocytes relative to the total reticulocyte count.
The performance of the new marker in the test set and in the validation set was satisfactory in screening PNH (Table 3).

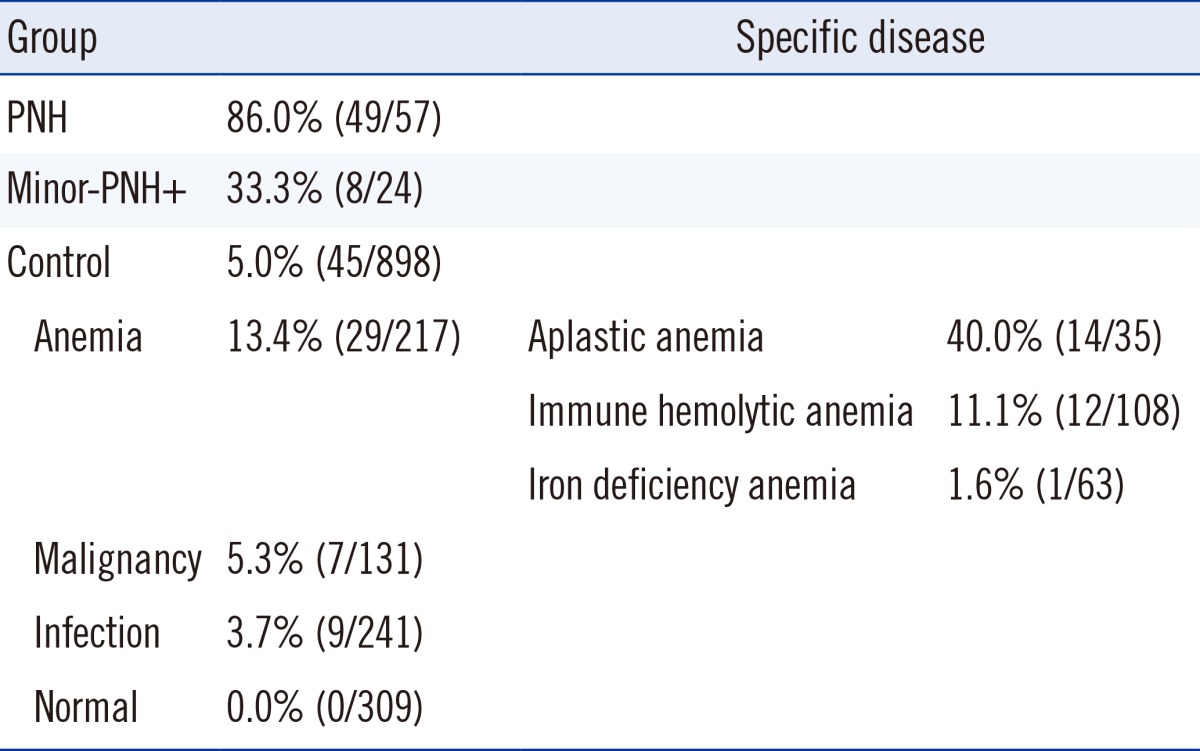
Table 4 shows the positive rates for PNH, control, and minor-PNH+ groups, when the PNH marker, consisting of these five parameters, was applied. Briefly, the PNH group exhibited 86.0% positive rate, the control 5.0%, and minor-PNH+ 33.3%. The anemia subgroup had the highest positive rate (13.4%) of the control groups; within the anemia subgroup, aplastic anemia was the highest (40.0%) compared to immune hemolytic anemia (11.1%) and IDA (1.6%).
When compared between only the PNH group and control group, the PNH marker showed 86.0% sensitivity (95% CI; 73.7-93.3), 95.0% specificity (95% CI; 93.3-96.3), 52.1% PPV (95% CI; 41.6-62.4), and 99.1% NPV (95% CI; 98.1-99.6).
Each parameter generally showed poor correlation to the number of PNH cells found by flow cytometry. Type II erythrocytes were not found in the study samples. Type III erythrocyte count was 37.9±36.6 (mean±SD), Type II granulocyte 0.4±1.2, and Type III granulocyte 52.6±43.2. Among the combinations of each parameter and PNH cell counts, only MN-AL2-NRET and type II granulocyte count showed a moderate correlation (r=0.548, P<0.0001).
Go to :
DISCUSSION
Using the same impedance methods as other CBC analyzers, DxH800 measures such primary CBC data as white blood cell, RBC, platelet count, MCV, RDW, and platelet distribution width; in addition, it uses VCS technology to determine white blood cell differential count and cell population data. VCS technology offers volumetric sizing of cells using direct current; conductivity according to the nuclear characteristics and granularity using alternating current in the radiofrequency range; and five light scatter signals (S; AL2, MALS, UMALS, LMALS, LALS) using a laser, providing comprehensive information regarding cell size, cell surface characteristics, and complexity of nucleus and cytoplasmic granules.
Also, in the reticulocyte channel of the Coulter DxH800, RBCs are processed in acidic hypoosmotic, ghosting solution to measure both reticulocyte-related parameters and RUO parameters [19, 20]. When reagent A (Retic A) containing new methylene blue and sulfuric acid is inserted into RBC, hemoglobin exudes out from the RBC, thus causing it tobecome a ghost cell. After fresh methylene blue staining, slight hypotonic and acidic reagent (Retic Clear, reagent B, pH 1.9) is added to clear the hemoglobin, and the parameters are promptly measured when RBCs are swollen in reagent B. In principle, this assay procedure resembles the Ham test and sugar water test, in that it is deemed PNH-positive when hemolysis is detected in RBCs in acidified serum or hypoosmotic conditions. The observation in which MRV, MSCV, MN-AL2-NRET, and IRF prominently increased in the PNH group in comparison with the control group is due to the characteristic of the PNH cell wherein it gets damaged easily in the reticulocyte channel and swells. On the other hand, there was no difference found with the normal subgroup for RDWR, which implies relative evenness of such characteristic changes in the PNH group. However, it is unknown why there is a higher value of RDWR for the anemia, malignancy, and infection subgroups of the control group than that for the PNH group.
With the established PNH marker, the minor-PNH+ group showed the expected positive rate belonging to the gray zone between the control group and PNH group. Minor-PNH+ does not present with PNH symptoms; however, it occurs either at the inception of mutation or with PNH following eculizumab treatment. Classical flow cytometric analysis for RBC CD55 and CD59 is not optimal in that PNH clone size can be affected by hemolysis or transfusion [21]. The same reason may have been true for our method as well; nevertheless, as a screening test, it is of high quality. To serve as a good quality screening test, satisfactory sensitivity is needed because patients with small PNH clones, such as AA/PNH, MDS/PNH, or subclinical PNH clones, are asymptomatic, while less than 10% of PNH clones rarely require clinical intervention, thus only the expansion of clones can be closely monitored [11].
The sensitivity of the validation set is lower than that of the test set, and if there had been more PNH samples, the sensitivity difference could be expected to be marginal. In attempting to increase sensitivity, the false positive rate increases; this is not a recommendable approach with diseases such as PNH with a very low prevalence. The present results demonstrate a high specificity, with an appropriate level of sensitivity and a high NPV, which helps exclude PNH in negative cases, and in positive cases provides a supplementary clinical means to test cases for potential PNH. It is very important that the new marker identified no patient from the normal group with suspected PNH. This ensures that there is a very low risk of performing flow cytometry for PNH-negative patients when our proposed PNH marker is used.
It was quite intriguing to see that the anemia group, especially aplastic anemia, showed a high positive rate, displaying the PNH disease spectrum. It is known that there is a high incidence of PNH minor clones in aplastic anemia patients. In light of our study, it is considered that aplastic anemia bears a significant resemblance to PNH before any incidence of PNH clones. Studies, including a prospective multicenter study, commonly show linkage between PNH and aplastic anemia and immune-mediated bone marrow failure [11, 12, 21, 22, 23, 24, 25, 26]. These positive cases should be closely followed up, monitoring PNH clone expansion. Relatively quicker and highly probable responses to immunosuppressive therapy can be expected for AA/PNH patients than for aplastic anemia patients with GPI-AP-deficient erythrocytes [27].
In the anemia group, immune hemolytic anemia falls just below aplastic anemia in the order of high false positive rates (11.1%), suggesting common hemolytic cell changes affecting the marker range. A hemolytic period, as a part of the PNH disease process, especially requires distinction from immune hemolytic anemia; therefore, patients with hemolytic anemia should first be screened using the proposed marker and confirmed by flow cytometry for a final diagnosis.
Because of the many co-occurrences of IDA, it is significant that, when comparing separately with IDA group, specificity increased to 98.4%. Thus, the criteria set forth in this study enable differential diagnosis of simple IDA with PNH.
In conclusion, a mere CBC exam can screen PNH with 95% specificity and 86% sensitivity. Furthermore, using five CBC parameters as PNH markers facilitates identification of PNH patients, thus considerably reducing the time required to a final diagnosis by flow cytometry. The limitation of the proposed PNH screening marker in this study lies in that the marker can be applied only to the Coulter DxH800.
Go to :
 XML Download
XML Download