

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Hemophagocytic lymphohistiocytosis (HLH) can be divided into primary (genetic or familial) and secondary (acquired or reactive) forms. Abnormal immunophenotyping and downregulation of CD5 or CD7 in T cells have been well characterized in Epstein-Barr virus (EBV)-associated HLH [1, 2]. A few studies have also reported abnormal immunophenotyping of T cells in patients with familial HLH (FHL) [1, 3]. Here, we report a case of FHL with immunophenotypically abnormal T cells and monoclonal T cells confirmed by a T-cell receptor (TCR) gene rearrangement test.
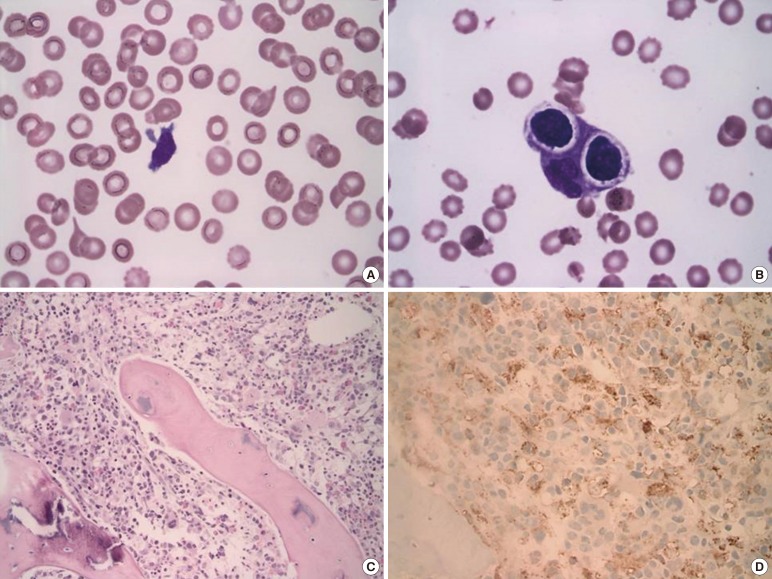
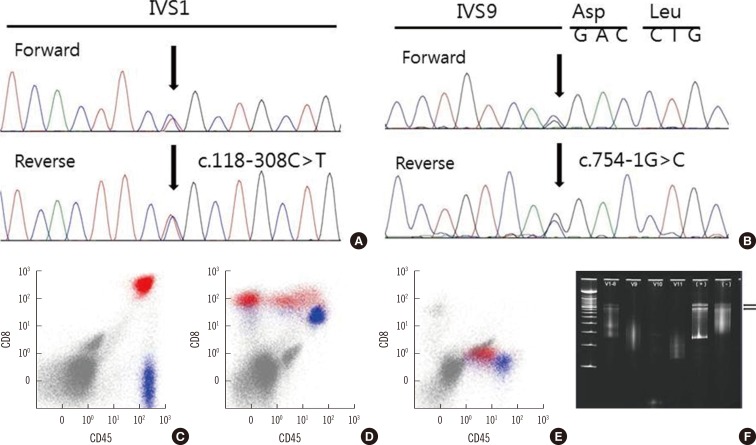
A 2-month-old infant was referred to our hospital for further evaluation and treatment of persistent fever and thrombocytopenia. Hepatosplenomegaly and petechiae were observed on physical examination. The total leukocyte count was 1.64×109/L, consisting of 65% lymphocytes, with 1% atypical lymphoid cells. The Hb level was 9.1 g/dL, and the platelet count was 20×109/L. Blood chemistry results were as follows: 570 IU/L AST, 454 IU/L ALT, 657 IU/L lactate dehydrogenase (LDH), 11.4 mg/dL total bilirubin, and 147 mg/dL fibrinogen. The prothrombin time (PT) and activated partial thromboplastin time (aPTT) was 15.3 sec (reference range; 12.6-14.9 sec) and 40.3 sec (reference range; 29.1-41.9 sec), respectively. A serological test to detect any underlying viral infection showed (+, positive; -, negative): anti-CMV IgG (+), anti-CMV IgM (-), anti-EB-VCA IgG (+), anti-EB-VCA IgM (-), EBV-EA (-), and anti-EB-NA IgG (+). The results of a chromosome study were normal (46,XY). Atypical lymphocytes were observed on peripheral blood smear (Fig. 1A). Hemophagocytic histiocytes were observed on bone marrow biopsy (Fig. 1B, C, and D). EBV was not detected by in situ hybridization. We performed mutation analysis of the FHL-related genes UNC13D and PRF1 using DNA isolated from peripheral blood. Sequencing analysis revealed compound heterozygous mutations in UNC13D [c.118-308 C>T (;)754-1G>C] (Fig. 2A and B). These mutations are frequently observed in Korean FHL patients [4]. Immunophenotyping using bone marrow aspirate revealed an abnormal population of CD8+ T cells with downregulated levels of CD5 or CD7 (14.61% of total events; Fig. 2C, D, and E). A TCR gene rearrangement study using paraffin-embedded tissue revealed T cell monoclonality [5] (Fig. 2F). The patient was treated with HLH-2004 chemotherapy and allogenic bone marrow transplantation. Bone marrow studies were performed before and after allogenic bone marrow transplantation. Hemophagocytic histiocytes were not observed in the follow-up bone marrow study. The patient remained in remission (follow-up time: 12 months after diagnosis). A familial study for UNC13D gene mutation was not performed.
Abnormal immunophenotype of CD8+ T cells with downregulation of CD5 is a common finding in HLH associated with viruses, especially EBV-associated HLH [1, 6, 7]. McCall et al. [1] reported that 6 of 9 cases (76%) of EBV-associated HLH had expansion of CD8+ T cell populations with variable downregulation of CD5, CD7, and/or CD3, whereas 1 of 8 cases (13%) of non-EBV-associated HLH showed downregulation of CD7 expression [1]. There are few reports on abnormal immunophenotype of T cells in FHL [1, 3, 8]. Karandikar et al. [3] reported a case of FHL associated with a perforin gene mutation that showed CD8+ T cells with loss of CD5 expression. Wada et al. [8] also reported a case of FHL associated with a perforin gene mutation that showed CD8+ T cells with loss of CD5 expression. Downregulation of CD5, CD7, CD3 and aberrant expression of HLA-DR is a common finding in both FHL and EBV-associated HLH or other acquired HLH [1, 3]. In this case, downregulation of CD5 and CD7 was found, as reported previously [1, 3]. The cause of downregulation of CD5 expression in acquired HLH or FHL remains unclear. Some authors have suggested a link between CD5 downregulation in T cells and monoclonal proliferation [6].
Our case also showed monoclonality in the TCR gene rearrangement study. Monoclonality in the TCR gene rearrangement study is also a common finding in EBV-associated HLH [9]. Monoclonal T cell proliferation in FHL has also been reported [10]. Moreover, the study also reported clonal changes in T cell populations after treatment (monoclonal to polyclonal) [10]. These results might help shed light on the pathogenesis underlying clonal proliferation of T cells and downregulation of CD5 in HLH.
To the best of our knowledge, this is the first report on FHL with an abnormal immunophenotype and T cell monoclonality in Korea. Further studies are needed to characterize the immunophenotypic features and clonality of T cells in FHL and their diagnostic or clinical significance.
 XML Download
XML Download