

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A genome-wide single nucleotide polymorphism array (SNP-A) assay can detect not only the copy number alterations but also the copy-neutral loss of heterozygosity (CN-LOH) on a chromosomal segment with high sensitivity, as demonstrated in MDS/MPN and NK (normal karyotype) AML [1,2,3,4,5]. However, no study has evaluated SNP-A assay in NK ALL, except for one that reported detection of copy number alterations and CN-LOH by SNP-A in 62% of NK ALL patients as well as smaller deletions compared with those in other leukemia subtypes [6]. In addition, the clinical relevance of unstable genotype (subtle changes in the size of detected alterations at relapse) has not been evaluated. We report three patients with NK ALL who harbored genomic alterations, as detected by a high-resolution SNP-A assay at both diagnosis and relapse. We also assessed the clinical relevance of slight changes in the size of affected genetic lesions at relapse with the maintenance of normal cytogenetics.
CASE REPORT
1. Case 1
A 38-yr-old man was diagnosed as having NK ALL on the basis of the results of negative HemaVision (DNA Technology; Aarhus, Denmark) and metaphase cytogenetics (MC) analysis. He was diagnosed as having B-cell ALL with NK and achieved complete remission (CR) at 10 weeks of treatment. He experienced relapse at 8 weeks after CR and, at relapse, his karyotype was maintained as normal and HemaVision results were also negative.
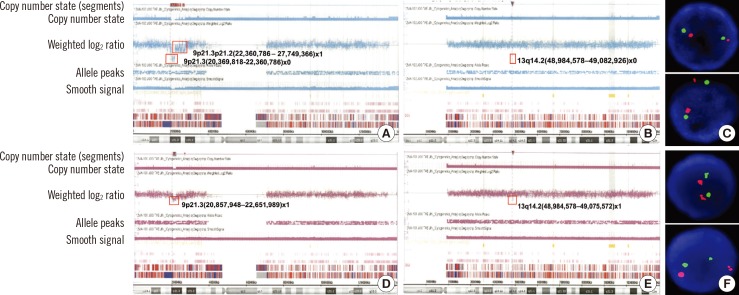
A genome-wide SNP-A assay was performed by using the Affymetrix Cytogenetics 2.7M Array (Affymetrix; Santa Clara, CA, USA) with bone marrow samples obtained both at diagnosis and relapse. At diagnosis, SNP-A analysis revealed homozygous deletions of 9p21.3 (associated with CDKN2A) and 13q14.2 (associated with RB1) and heterozygous deletions of 6p22.2, 8q22.1, 9p21.3p21.2, 14q11.2, 18q22.2, and 19p13.2 (Fig. 1A, B). FISH analysis for the detection of RB1 deletions showed nuc ish (RB1,13q14)×2[200] (Fig. 1C). An identical assay performed at relapse showed loss of heterozygous deletions in 6 affected lesions along with subtle size changes in deleted lesions of 9p21.3 (1,944-1,752 kb) and 13q14.2 (96-89 kb), indicating the persistence of CDKN2A and RB1 deletion at relapse (Fig. 1D, E). FISH analysis for the detection of RB1 deletions also showed nuc ish (RB1,13q14)×2[200] (Fig. 1F).
2. Case 2
A 57-yr-old woman was diagnosed as having NK ALL on the basis of the results of HemaVision (negative) and MC analysis. SNP-A analysis at diagnosis revealed heterozygous interstitial deletions of 3q13, 4q23q24, 5q15q21.3, 5q21.3q22.1, 5q22.3q23.1, 5q34, 6q16.3q21, 7q11.23, and 13q14.2q14.3, including RB1 (Fig. 2A). She achieved CR after 4 weeks of treatment but experienced relapse at 6 months after CR. At relapse, her karyotype was normal and HemaVision results were also negative. Results of SNP-A analysis at relapse showed heterozygous deletions of 3q13, 4q23q24, 5q15q21.3, 5q21.3q22.1, 5q22.3q23.1, 5q34, 6q16.3q21, 7q11.23, and 13q14.2q14.3, including RB1 (Fig. 2B), which is similar to those at diagnosis. However, the deleted genomic lesions of 3q13, 4q23q24, 5q15q21.3, 5q21.3q22.1, 5q34, and 13q14.2q14.3 at relapse were slightly different from those at diagnosis.
3. Case 3
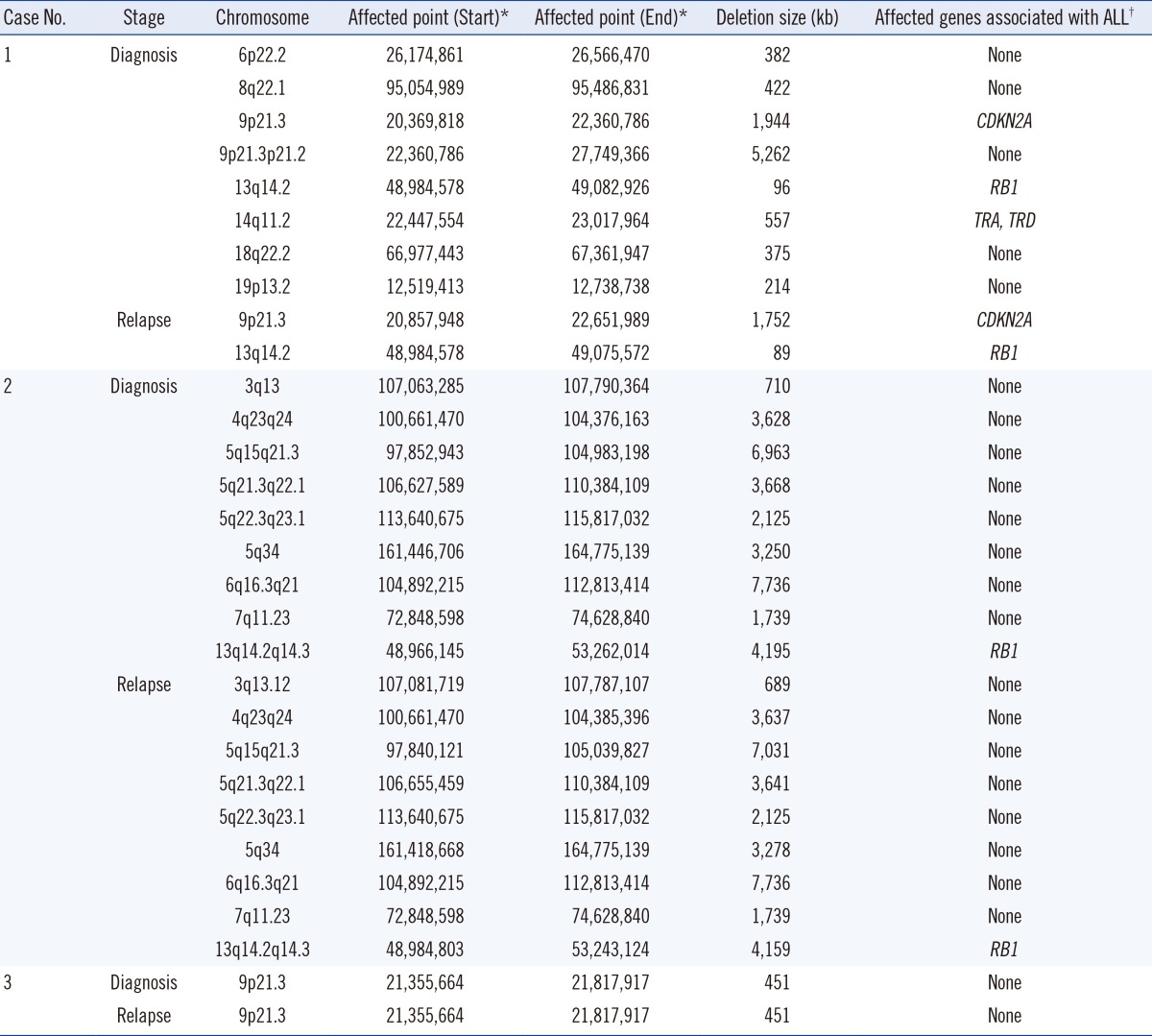
A 58-yr-old man was diagnosed as having NK ALL as per the results of HemaVision (negative) and MC analysis. He achieved CR after 4 weeks of chemotherapy but experienced relapse at follow-up 32 months after remission. At relapse, the HemaVision results were also negative. However, SNP-A analysis demonstrated an interstitial 451 kb deletion of 9p21.3, which includes interferon α-1/13 (IFNA13) and micro-RNA 31 (MIR31) in a mosaic pattern, at both diagnosis and relapse (Fig. 2C). Demographic findings of the deleted genetic lesions and the affected genes associated with ALL in the three cases are represented in Table 1.
DISCUSSION
In Case 1, SNP-A analysis could detect the presence of interstitial microdeletion including both RB1 and CDKN2A, which is not otherwise detectable by MC or FISH analysis. Because the deletions of CDKN2A and RB1 are associated with poor prognosis in ALL [7, 8], this may suggest that SNP-A assay can provide prognostic information in NK ALL. The SNP-A assay could detect subtle size changes in the affected lesions (microscopic clonal evolution) and recovery of small-sized interstitial deletions at relapse, which are also not detectable by MC. Thus, the SNP-A assay is more advantageous in detecting microscopic clonal evolution than other methods. In addition, in Case 2, SNP-A assay could detect subtle changes in the size of the affected genetic lesions at relapse (unstable genotype). We may speculate that unstable genotype may indicate microscopic clonal evolution at relapse. The early relapse in Case 2 patient supports this speculation.
The association between ALL and the loss of IFNA13 and MIR31 is unclear. However, as abnormal 9p is an adverse prognostic factor for B-ALL [9], the interstitial deletion of 9p21.3 detected by SNP-A analysis may contribute to poor prognosis, as demonstrated by early relapse in Case 3.
Our report has some limitations. First, the SNP-A assay at relapse in Case 2 did not show any additional abnormalities and slight size changes in the detected genetic lesions as evidence of clonal evolution have not been demonstrated. Therefore, the presence of unstable genotype should be regarded only as a phenomenon suggesting various events, including clonal evolution. Second, we could neither perform SNP-A analysis using samples with CR or fibroblasts, which is important for the discrimination of acquired somatic events from germline aberrations, nor confirm whether all genetic abnormalities detected in our cases were somatic. Third, we could not perform FISH analysis in RB1 in Case 2 as well as detailed evaluations of the discrepancies between the results of FISH and SNP-A analysis. The discrepancy in the results of FISH and SNP-A analysis regarding the RB1 gene in Case 1 may be explained from different detection sensitivity of both methods. However, more comprehensive analysis is required for comprehending this discrepancy.
In conclusion, our case report demonstrates that a SNP-A assay can allow sensitive detection of cryptic changes affecting clinically important genes. A SNP-A assay may be more advantageous than other methods in detecting unstable genotype at relapse, which may be associated with microscopic clonal evolution and poor prognosis in ALL.

 XML Download
XML Download