

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
HLA-identical related donors are only available for approximately 25% of patients that require allogeneic hematopoietic stem-cell transplantation (HSCT). As such, HLA-matched unrelated donors are widely used [1]. The precise impact of HLA mismatching on unrelated HSCT remains unclear, particularly with regards to the relative importance of different HLA loci, as well as the significance of antigenic versus allelic mismatches [2]. Killer cell immunoglobulin-like receptor (KIR) ligand mismatches have been associated with a significant increase in overall survival, as well as better engraftment and a reduced incidence of graft-versus-host disease (GVHD) in patients with AML [3]; however, debates still exist on the impact of KIR ligand mismatch status in the outcome of unrelated HSCT [4, 5]. In addition, these effects vary greatly among different ethnic groups, especially in Japanese patients [6, 7].
The HLA frequency distribution found in Koreans is most similar to that of the Japanese population [8, 9]. However, to the best of our knowledge, the effect of HLA or KIR ligand mismatching and KIR ligand status on the outcome of HSCT from unrelated donors in Korean adult patients has not yet been examined. In this study, we retrospectively assessed the impact of high-resolution donor-recipient mismatching at the HLA-A, -B, -C, -DRB1, and -DQB1 loci, as well as KIR ligand mismatching and KIR ligand status, on the clinical outcome of 154 Korean adult patients treated with unrelated HSCT.
METHODS
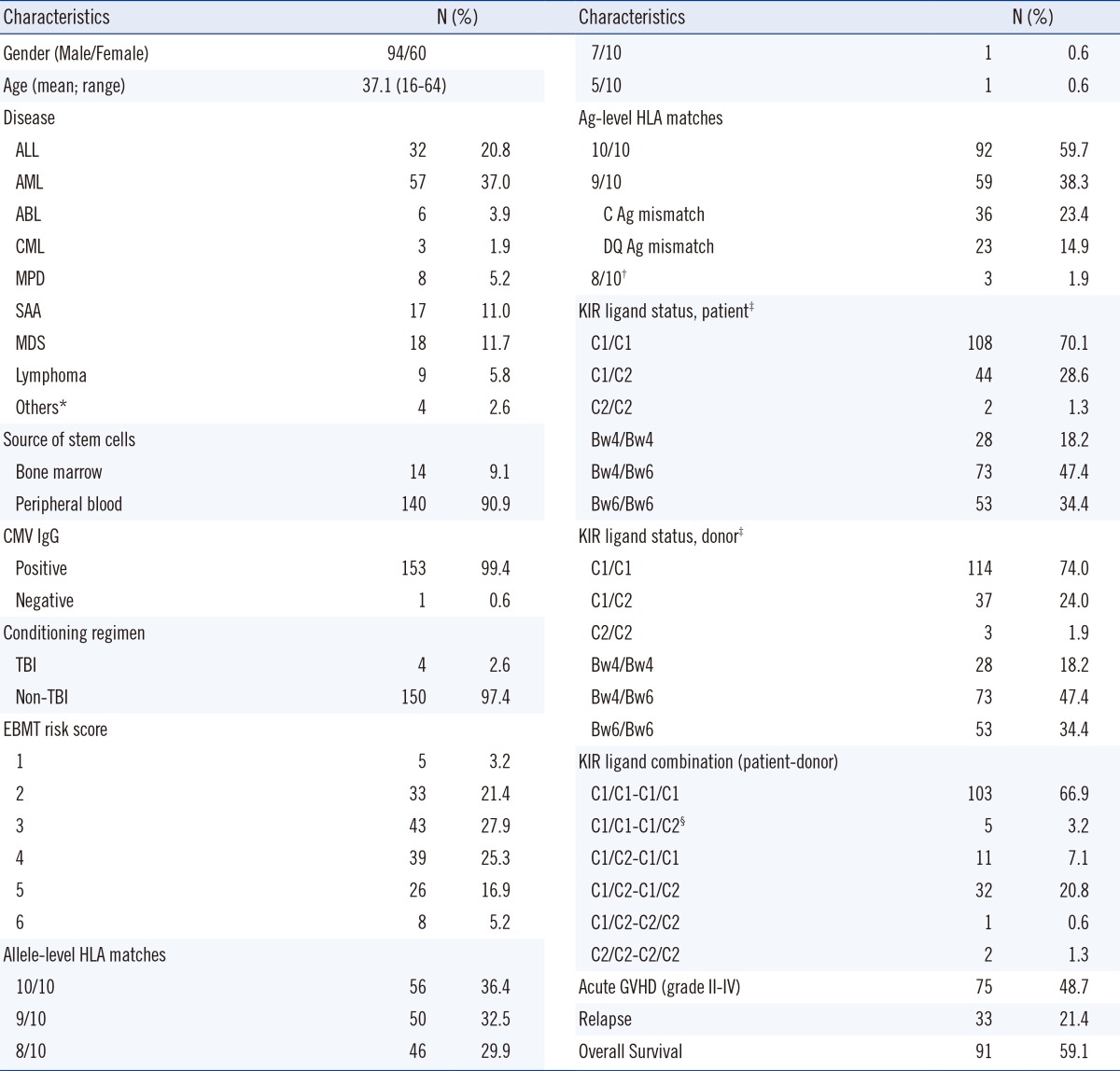
Patients receiving unrelated HSCT between April 2006 and December 2012 in Seoul National University Hospital were included in this study (n=154). Allele SEQR PCR/Sequencing kits for the HLA-A, -B, -C, -DRB1, and -DQB1 alleles were used for sequence-based typing (SBT) at the time of transplantation (all from Atria Genetics, South San Francisco, CA, USA). This study was approved by the institutional review board of Seoul National University Hospital (1309-068-521). Patients were categorized according to their HLA-inhibitory KIR ligand on the basis of their expression of (1) HLA-Bw4 or (2) HLA-Cw groups (C1 or C2) (Table 1) [10]. C1 alleles express Asn80 (such as -Cw1, -Cw3, -Cw7, -Cw8, -Cw12, -Cw12, -Cw14, -Cw16, etc.), whereas C2 alleles express Lys80 (such as -Cw2, -Cw4, -Cw5, -Cw6, -Cw15, -Cw17, -Cw18, etc.) [5]. KIR ligand mismatches were defined by the absence of one donor KIR ligand class I allele in the recipient [11]. For HLA-Cw groups, C1/C1 patients with C1/C2 donors, and C2/C2 patients with C1/C2 donors, were considered KIR ligand mismatches.
High-resolution HLA matching on the HLA-A, -B, -C, -DRB1, and -DQB1 loci, KIR ligand mismatch, and KIR ligand status were analyzed for their associations with the following clinical outcomes: patients' overall survival, event-free survival, relapse of underlying disease, and the occurrence and severity of acute or chronic GVHD [12]. Overall survival was defined as the time from graft infusion to death from any cause at time of analysis (Jun 1, 2014). For event-free survival, death or relapse was considered as events. Clinical characteristics of patients are shown in Table 1. Pre-HSCT patient risk status was classified by the European Group for Blood and Marrow Transplantation (EBMT) scoring system [13]. Antigen-level HLA mismatches were observed only at the HLA-C and -DQB1 loci in our study (Table 1).
Regression analysis was performed to assess the effect of different risk factors on clinical outcome. Categorical variables were analyzed by Chi-square and Fisher's exact tests. The Cox proportional hazard model was applied for multivariate analyses. Survival was analyzed by Kaplan-Meier with log-rank testing. All reported P values are 2-sided, and P value <0.05 was considered statistically significant. All analyses were performed by using SPSS Statistics 21.0 (IBM, Armonk, NY, USA).
RESULTS
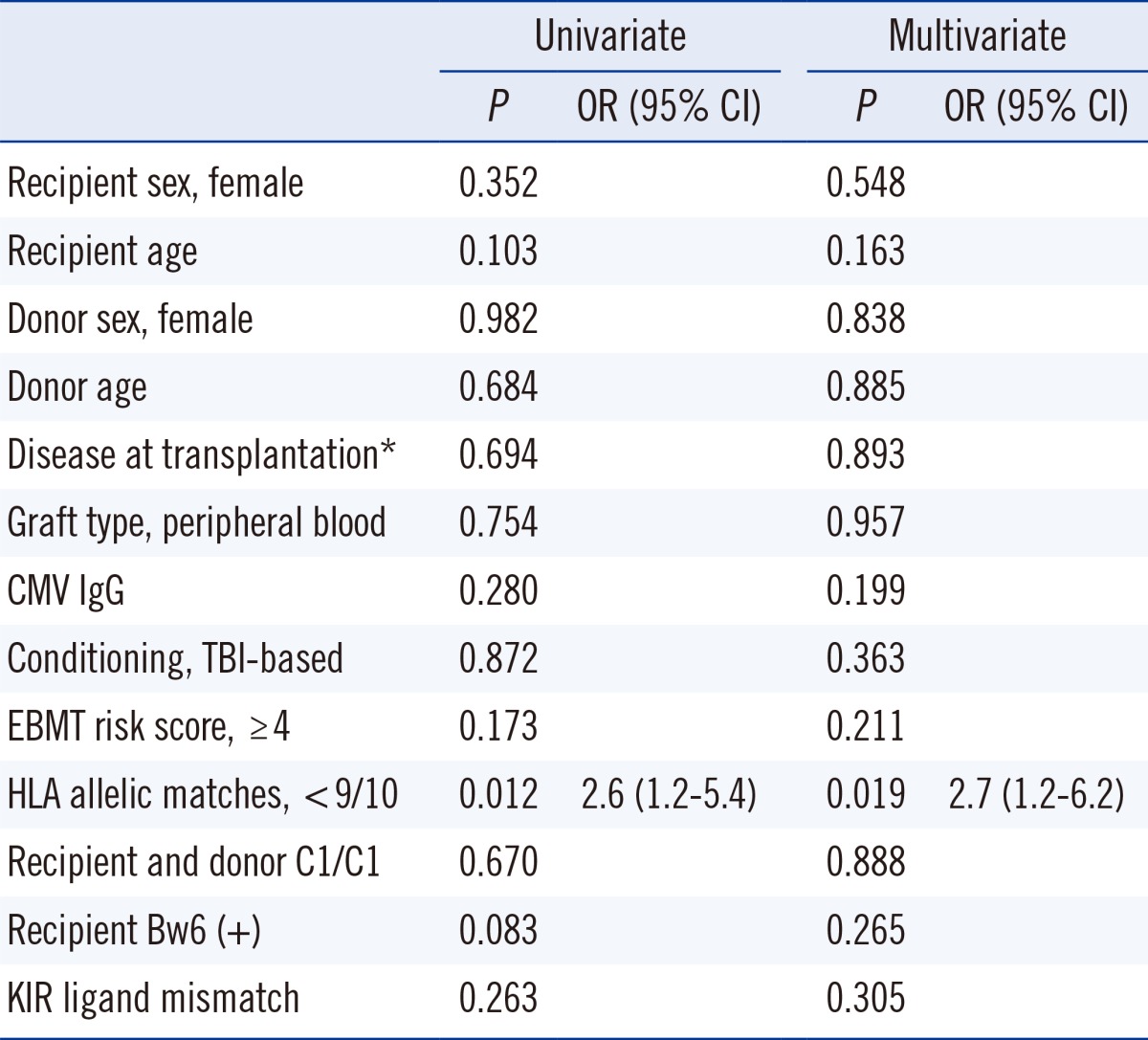
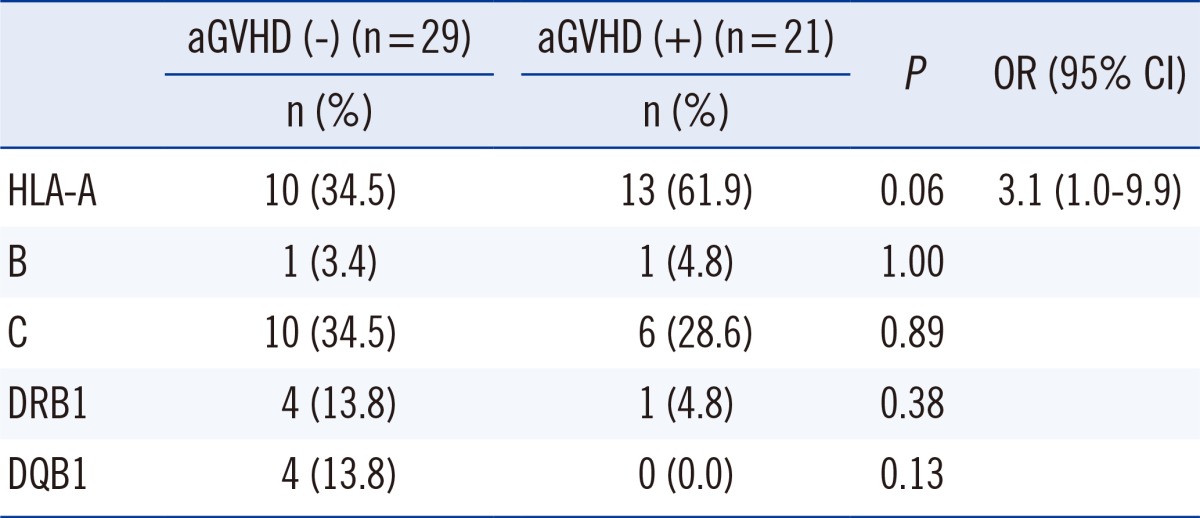
Of the five HLA loci, allelic mismatches of >9/10 alleles was considered a risk factor for severe acute GVHD (Grade II-IV) by univariate analysis (P=0.012, hazard ratio [HR]=2.6), and was also an independent risk factor for severe acute GVHD (Grade II-IV) by multivariate analysis (P=0.019, HR=2.7) (Table 2). The frequency of mismatch at the HLA-A allele was increased in patients with acute GVHD compared to those without (61.9% vs. 34.5%, P=0.06), among one mismatched allele in unrelated HSCT (n=50) (Table 3). In contrast, the frequency of mismatch at other HLA loci (HLA-B, -C, -DRB1, and DQB1) failed to show any significant difference between the two groups.
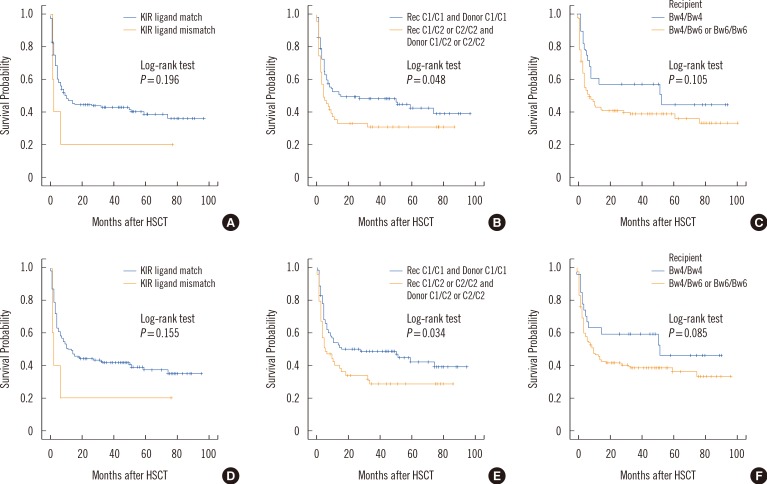
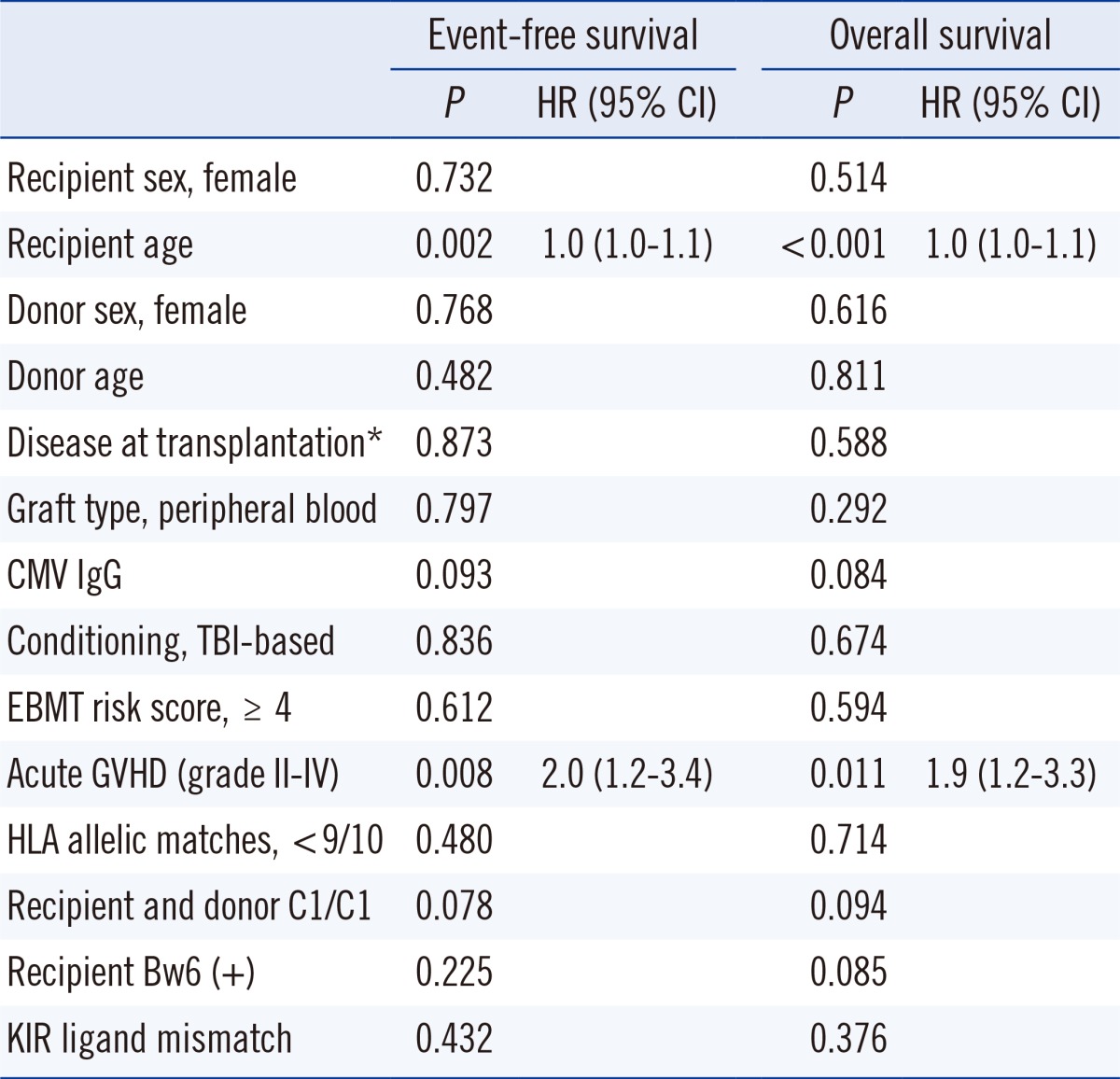
In Cox proportional hazard model, acute GVHD (grade II-IV) was an independent risk factor for event-free survival (P=0.008, HR=2.0) and overall survival (P=0.011, HR=1.9) (Table 4). In our patient population, KIR ligand mismatch occurred in only five HLA-Cw group recipient-donor combinations (all of which were recipient C1/C1 and donor C1/C2; 5/154, 3.2%) (Table 1) and had no effect on clinical outcome (Table 4). For the analysis of KIR ligand status, recipient-donor combinations of both C1/C1 ligands showed an increased tendency for event-free and overall survival than recipient-donor combinations with C2 ligand (recipient C1/C2 or C2/C2 and donor C1/C2 or C2/C2) (P=0.078, P=0.094, respectively) but did not reach statistical significance (Table 4). In Kaplan-Meier survival analysis, C1/C1 recipient-donor combinations showed a significant increase in event-free and overall survival compared to C2 recipient-donor combinations (recipient C1/C2 or C2/C2 and donor C1/C2 or C2/C2) (P=0.048, P=0.034, respectively) (Fig. 1).
DISCUSSION
Previous studies have reported some ethnic variance in the relationship between HLA mismatching and HSCT patient outcome, especially in the Japanese population. Notably, a single HLA-A mismatch was considered to be a significant risk factor for survival (HR=2.27) in the Japanese Marrow Donor Program (JMDP); however, single HLA-C mismatch was a risk factor in non-JMDP transplants (HR=1.68) [6]. In Japanese patients, HLA-A or -B mismatches significantly reduced survival, whereas mismatches at HLA-C or -DRB1/DQB1 did not [14]. In our study, less than nine allelic matches among five HLA loci were significantly associated with acute GVHD (grade II-IV). In addition, the association between HLA-A mismatching with acute GVHD (grade II-IV) is suspicious, since the other loci failed to show any association, somewhat similar to the previous Japanese reports [6, 14]. In a previous study of 1,047 Japanese patients with HLA-A2, a mismatch combination of HLA-A*02:01-*02:06, revealed inferior survival (HR=1.58) [7]. Non-permissive allelic mismatch combinations of A*02:06-A*02:01, A*02:06-A*02:07, A*26:02-A*26:01, and A*26:03-A*26:01 have been reported in Japanese patients [15]. Koreans are genetically most similar to Japanese [8, 9] and show more allelic diversity, particularly in HLA-A*02 and A*26 than Caucasians [8]. This causes higher allele-level mismatch frequencies of A*02 and A*26. In our study, 22 out of 23 HLA-A allelic mismatches were the result of mismatching at HLA-A*02 (n=16) or A*26 (n=6). In Koreans, those mismatches could be associated with acute GVHD and poor clinical outcome in unrelated HSCT and should be confirmed in a larger patient population.
Furthermore, KIR ligand mismatching was not associated with clinical outcome following unrelated HSCT in this study. Results from previous studies on the impact of KIR ligand mismatching in unrelated HSCT were highly variable, and ranged from highly beneficial to detrimental [17, 18, 19, 20, 21, 22, 23, 24]. This was partly due to the differences in the methods used to analyze donor-versus-recipient NK-cell alloreactivity [25]. Differences in patient populations, underlying disease states, conditioning regimens, HLA match status, T-cell depletion, and post-transplant immunosuppressive regimens could also account for these discrepancies [5, 25]. In addition, there were also considerable ethnic differences in KIR gene and ligand frequencies [26]. In Koreans, the frequency of HLA-C2 ligand is much lower than that of Caucasians [8]. In our study, the portion of recipient-donor pairs with KIR ligand mismatch was very small (3.2%, 5/154), which may weaken the statistical power.
For the analysis of KIR ligand status, C1/C1 ligand patient-donor combinations showed an increase in event-free survival when compared to patient-donor combinations with C2 ligand (recipient C1/C2 or C2/C2 and donor C1/C2 or C2/C2). Further studies are needed with a larger patient population to confirm the impact of KIR ligand status on clinical outcome. In Germany, the increase in overall survival for patients with C1/C1 ligand was reported for those with AML/CML, but did not extend to those with ALL/NHL [20]. On the contrary, a study from the International Histocompatibility Working Group (IHWG) identified a lower rate of relapse in C1/C1 patients and to a similar extent in the AML, CML, and ALL subgroups [17]. In our study, the subgroup analyses failed to reach statistical significance (data not shown). The inconsistent results in ALL patients should be further clarified in future.
HLA-Bw4 ligand was not associated with clinical outcome in our study. A study on 264 cases of unrelated HSCT identified increased relapse rate and decreased overall survival in patients with Bw6/Bw6 ligand with donors with KIR3DL1/3DS1 [22]. The basis for the association between C1/C1 or Bw4/Bw4 ligand and better overall survival is unclear. Early reconstitution of KIR repertoires has been reported following HSCT in NK cells with C1-specific KIR2DL2/3 or Bw4-specific KIR3DL1, as compared to NK cells with C2-specific KIR2DL1 [27, 28, 29], and may contribute to the better overall survival by facilitating the surveillance of HLA-C expression on leukemic or virus-infected cells. In addition, the affinities of inhibitory KIRs for their respective HLA-C ligands vary, with KIR2DL1 exhibiting the strongest affinity and inhibitory signals [30]. As NK cell activation depends on a balance between inhibitory and activating signals, another explanation might be that donors with C2 ligand are less effective in activating leukemia-targeting NK cells than C1 ligand donors.
Despite the small number of cases in our study, all patients were treated at one center under uniform HSCT protocols. In conclusion, matches with less than 9 of 10 alleles from HLA-A, -B, -C, -DRB1, and DQB1 loci were associated with acute GVHD (grade II-IV) in Korean adult patients that received unrelated HSCT. The impact of KIR ligand status on clinical outcome was inconclusive and should be studied in a larger patient population.
 XML Download
XML Download