

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The most prevalent marker of myeloid engraftment is the time, from nadir after transplantation, when the absolute neutrophil count (ANC) crosses 500/µL [1]. This marker is observed, on average, in the vicinity of 14 days, and is occasionally delayed by up to 1 month [2]. Extensive supportive care is very important during this period to prevent opportunistic infections or other complications before engraftment is complete [3, 4]. To facilitate early prediction, studies have shown new valid criteria for early engraftment confirmation, for example, ANC >100/µL [5]. Though it has been established that monocytes precede granulocytes, platelets, and natural killer cells in engraftment [6], monocytes are not yet used as an engraftment marker, because the number of monocytes, even under normal conditions, is much lower than that of neutrophils.
Some automated hematology analyzers have recently started to offer new parameters, enabled by data fusion software, that make accurate complete blood count (CBC) with differentials (CBC-diff) possible in severe leukopenic samples. Recent studies [7-10] have used these new parameters to diagnose infectious diseases or various clinical conditions. The objective of this study was to verify whether these parameters can be used for early detection of myeloid engraftment and to establish the validity of monocyte-related parameters as an engraftment marker. If these parameters allow for the detection of the first release of neutrophils or monocytes into peripheral blood, confirmation of engraftment may be established earlier than the current standard of ANC increase.
METHODS
1. Study population
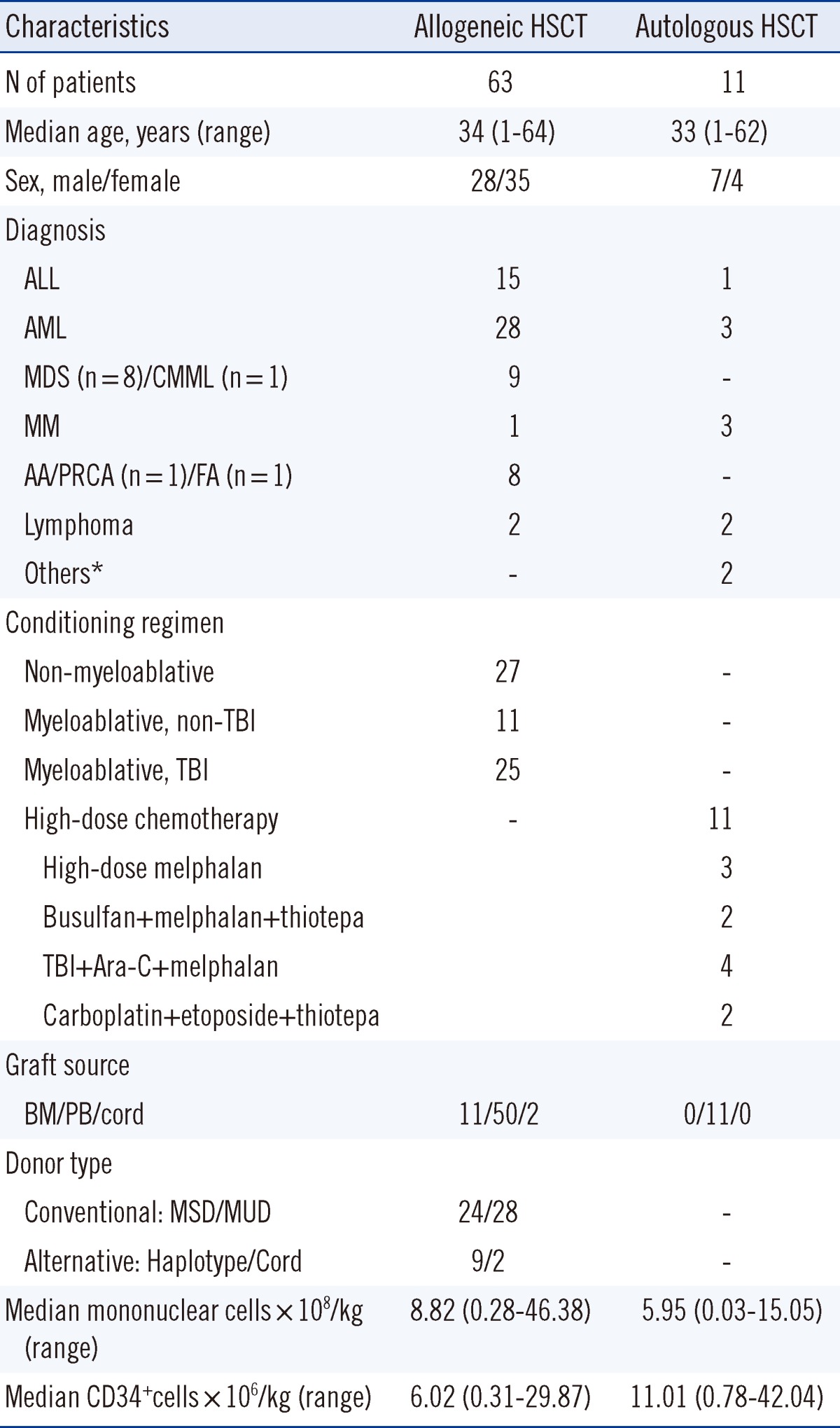
We collected data from 77 patients at Seoul St. Mary's Hospital, Korea, who underwent hematopoietic stem cell transplantation (HSCT) between December 2011 and April 2012. Every workday, data from CBC-diff studies were gathered. Table 1 shows patient characteristics and transplantation-related factors.
Our study population consisted of 3 patients with engraftment failure, and 74 with successful engraftments, among whom 63 patients (83.1%; median age, 34 yr) underwent allogeneic HSCT from sibling, haploidentical family member, unrelated, or cord blood donors. The remaining 11 patients (median age, 33 yr) received high doses of chemotherapy and autologous stem cell reinfusion. The median number of CD34+ cells infused was 6.02×106/kg for allogeneic HSCT and 11.01×106/kg for autologous HSCT. There were 2 cases, in which donor granulocytes were infused. This study was approved by the institutional review board of the Catholic Medical Center.
2. Establishment and analysis of the new markers
We used an automatic hematology analyzer (DxH 800, Beckman Coulter Inc., Miami, FL, USA) to obtain data, including CBC-diff and cell population data, using direct current impedance to measure cell volume (V) for accurate size of all cell types, ratio frequency opacity to characterize conductivity (C) for internal composition of each cell, and a laser beam to measure light scatter (S) for cytoplasmic granularity and nuclear structure. The Coulter VCS technology provides, for each cell type, mean and standard deviation values for volume, conductivity, and 5 light scatter (MALS, UMALS, LMALS, LALS, AL2). We analyzed these 14 parameters each for neutrophils and monocytes. We serially dotted these 28 parameters from the day of HSCT to identify any parameters that conspicuously constituted patterns related to engraftment. The collected data were organized in ascending order of test dates after transplantation. The resulting data helped in visualizing evolving trends of parameter values over time for each patient. These patient data were stored in Excel, and we identified all patients with successful myeloid engraftment using the conventional marker, ANC >500/µL, and marked the dates that engraftments were achieved.
1) Establishing predictive cutoff values for the proposed markers of neutrophilic and monocytic engraftment
Each parameter cutoff value was established as follows: 1) from the engraftment cases, a value that predicted engraftment days earlier than, or at least on the same day as ANC; and 2) the value was not found in the failure cases. After identifying cutoff values, we searched for the earliest engraftment day of each case on which the time from D0 was no less than 5 days and the day's MNV value higher than MNV cutoff value and its mean-conductivity-neutrophils (MNC) value lower than MNC cutoff value for the first time. This process was repeated for all cases.
2) Analysis of the performance of the new engraftment markers in predicting engraftment
We compared the engraftment dates predicted by the new markers with those identified by ANC. Using the sustained engraftment cases, we calculated the average difference in post-transplant days required to reach each new marker for predicting engraftment. Using the engraftment dates obtained from the ANC prediction and the new markers, we then attempted to 1) ascertain if engraftment was identified by using the new markers for all cases, 2) identify the marker that provided the earliest engraftment date for each case, 3) calculate the differences in engraftment prediction dates between markers, and 4) determine whether transplant-related clinical variables would incur differences in engraftment prediction dates.
3. Statistical analysis
We used Student's t-test or ANOVA to test the effect of transplant-related clinical variables on the engraftment day using our new engraftment markers. A P value <0.05 was considered statistically significant. All statistical analysis was performed using SPSS 20.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
1. Established predictive patterns and cutoff values forthe proposed markers of neutrophilic and monocytic engraftment
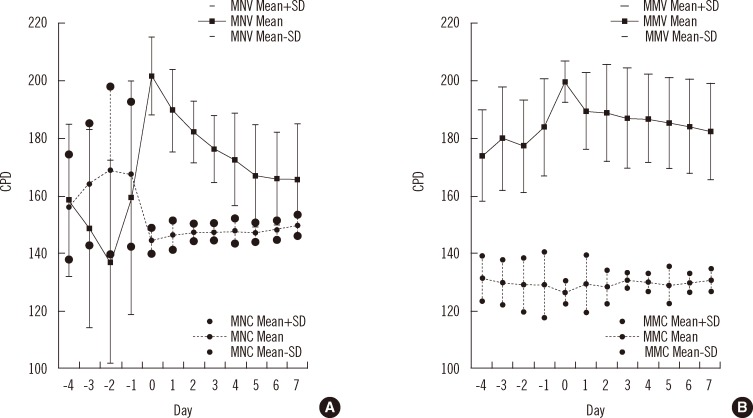
We analyzed the engraftment patterns that showed volume peaks and conductivity notches. We identified 2 combinations of parameters as engraftment markers: a pair of mean-volume-neutrophils (MNV) and MNC as a neutrophilic engraftment marker (NEUTRO) (the pattern of which reveals that MNV peaks simultaneously as MNC notches), and a pair of mean-volume-monocytes (MMV) and mean-conductivity-monocytes (MMC) as a monocytic engraftment marker (MONO), which shows a similar, though not as strong as in NEUTRO, pattern in which MMV peaks as MMC notches (Fig. 1).
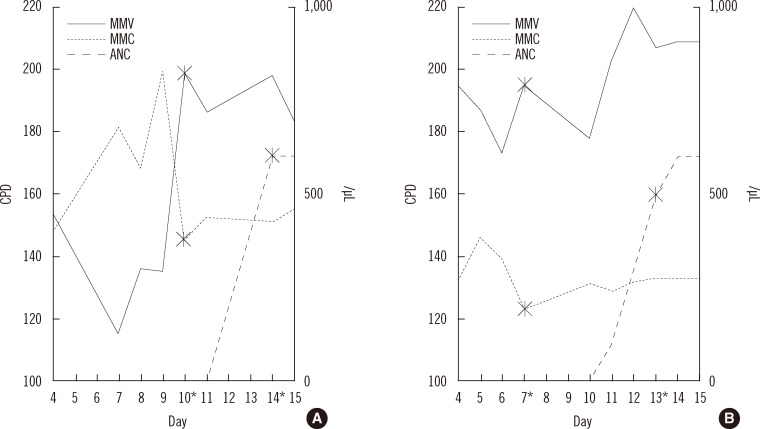
With 2 sets of parameters identified as early predictable markers and their significant engraftment patterns established, we then set the cutoff values as follows: NEUTRO at MNV >185 and MNC <150, and MONO at MMV >190 and MMC <130. Typical cases are shown in Fig. 2.
2. Engraftment days detected by each marker for the study population
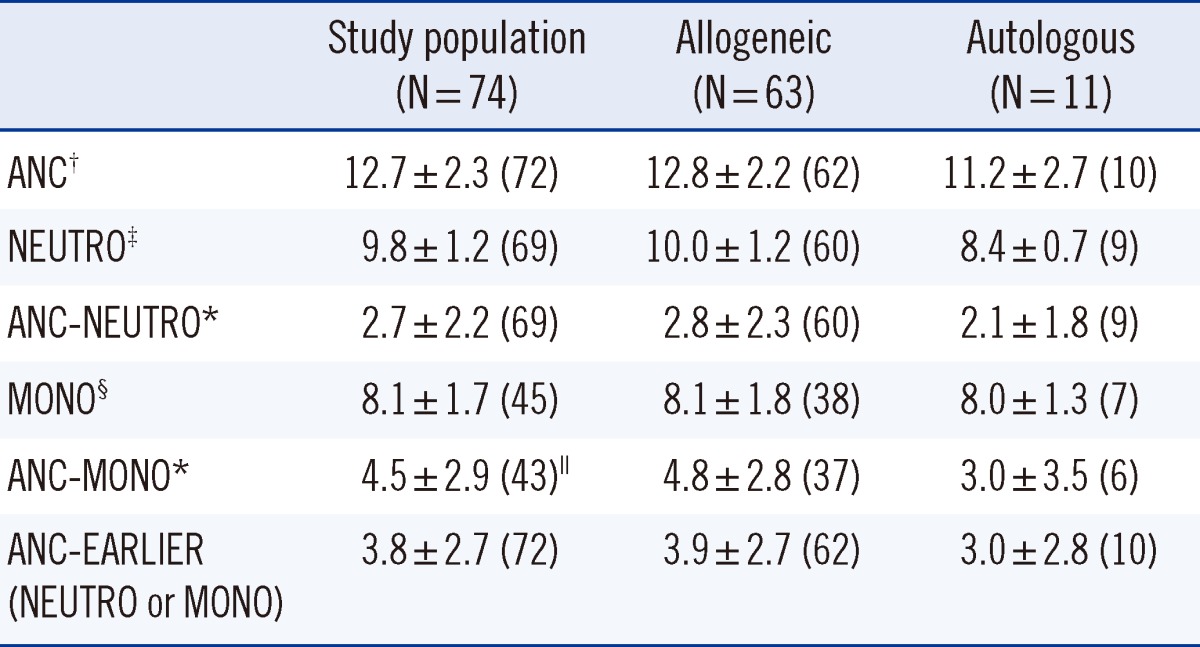
The average number of days before engraftment using ANC was 12.7±2.3. With NEUTRO, engraftment was predicted after 9.8±1.2 days, which antedated ANC by 2.7±2.2 days for successful engraftment cases (P<0.0001). MNV was 202.4±13.7 and MNC 143.9±4.4 on the days of engraftment for the study population. With MONO, the average number of days before engraftment was 8.1±1.7 days, which antedated ANC by 4.5±2.9 days for successful engraftment cases (P<0.0001). MMV was 199.5±7.6, and MMC 126.4±4.0 on the days of engraftment for the study population. None of the cases with engraftment failure reached marker values of NEUTRO or MONO (Table 2).
Engraftment was predicted, on average, 3.8±2.7 days earlier than the conventional ANC prediction in 74 successful engraftment cases by using one or both of the proposed markers: 1) 72 cases (97.3%), in which NEUTRO and/or MONO predicted engraftment earlier than ANC, 2) 1 case, in which the 3 markers predicted engraftment on the same day, and 3) 1 case, in which NEUTRO predicted the same engraftment day as ANC, and MONO failed to predict engraftment.
In the analysis of the 74 successful engraftment cases, NEUTRO showed earlier predictions than ANC in 63 cases (85.1%), and MONO demonstrated earlier predictions than ANC in 43 cases (58.1%). Furthermore, MONO showed earlier predictions than NEUTRO in 27 cases (36.5%); NEUTRO demonstrated earlier prediction than MONO in only 1 case.
In the analysis of the 47 cases for which we were able to collect complete serial data from 5 days after HSCT to ANC engraftment, NEUTRO showed earlier prediction than ANC in 43 cases (91.5%); the only exceptions were the 2 cases of donor granulocyte infusion (DGI) and another 2 cases in which both ANC and NEUTRO coincided. MONO achieved earlier predictions than ANC in 33 cases (70.2%), and MONO showed earlier predictions than NEUTRO in 24 cases (51.1%). NEUTRO showed earlier prediction than MONO in only 1 case. There were 12 cases (25.5%) that never reached the MONO values. On average, NEUTRO provided an earlier prediction by 3.2±2.2 days, and MONO by 4.6±2.9 days, compared with ANC. Engraftment was predicted, on average, 4.2±2.7 days earlier than that by conventional ANC in these 47 cases.
3. Transplant-related variables and engraftment days detected by each marker
The engrafment day predicted by ANC was earlier in autologous HSCT (Auto; 11.2±2.7 days) than in allogeneic HSCT (Allo) (12.8±2.2 days; P=0.0485). The same held true in the case of engraftment prediction by NEUTRO, with engraftment predicted earlier in Auto (8.4±0.7 days; n=9) than in Allo (10.0±1.2 days; n=60; P=0.0004). There was no significant differences between the groups with respect to engraftment prediction by MONO. The values of the marker parameters, MNV, MNC, MMV, and MMC, were 204.0±12.9, 143.0±4.9, 195.7±2.7, and 124.7±6.8, respectively, in Auto; and 202.2±8.0, 144.1±4.3, 200.2±8.0, and 126.7±3.2, respectively, in Allo. The differences in the values between the groups were not significant (Table 2).
Between Auto and Allo, the only significant difference in transplant-related variables was the number of CD34+ cells infused: 11.01±14.33×106/kg in Auto and 6.02±5.70×106/kg in Allo (P=0.0460). There was a weak correlation between the number of CD34+ cells infused and engraftment day predicted using ANC >500/µL (r=-0.304) or NEUTRO (r=-0.333). There were no significant correlations between the new markers and primary diseases, chemotherapy regimen, irradiation intensity, or donor cell types in the study population (P>0.05). There were 2 cases wherein the patients received DGI but did not reach nadir after infusion, steadily maintaining ANC >500/µL levels through the entire recovery period. Neither NEUTRO nor ANC offered assistance in identifying engraftment, whereas MONO predicted successful engraftment in 8 days in both cases.
DISCUSSION
Engraftment after HSCT entails successful stem cell homing and repopulation into the recipient bone marrow, and re-initiation of the hematopoietic process. The neutrophils used as NEUTRO (a combination of MNV and MNC) in this study were of low conductivity, and comparatively larger in volume than the neutrophils observed in normal peripheral blood. MNV may increase owing to infections such as fungemia, but conductivity rarely fluctuates [7-10]. The values of MNV and MNC measured on the engraftment days for all the study cases were 202.4±13.7 and 143.9±4.4, respectively, which show the highest value of MNV and lowest value of MNC, with a narrow standard deviation.
The neutrophils satisfying the marker values are assumed to be the first neutrophils released into the peripheral blood, because they appeared just after the nadir period. Furthermore, the volume of these cells decreased and conductivity increased immediately after they released into the blood, and it is a trend similarly observed in reticulocyte changes in the blood [2, 5]. Similar changes are also observed in monocytes. It is quite interesting that granulocytes also show characteristic morphologic changes just after being released into the peripheral blood from bone marrow, although we cannot recognize these changes under the microscope. An increase in MNV and MMV means that they are larger than mature neutrophils and monocytes. However, their sizes are not visible to the naked eye. Another parameter, conductivity, reflects intracellular components. Therefore, decreased conductivity of the earliest cells means that their intracellular components are slightly different from mature cells.
On average, NEUTRO and MONO enable an earlier engraftment prediction of 4.2±2.7 days earlier than ANC after HSCT. It is valuable to confirm engraftment 4 days earlier. Early predictions of engraftment using MONO were also possible for the cases with DGI. Indeed, as ANC may be continuously high in such cases, regardless of engraftment, MONO may be a more accurate engraftment marker.
We presume that the differences in engraftment days between the Allo and Auto groups stemmed from the fact that there were more infused CD34+ cells (P=0.046) in Auto than in Allo, which is in agreement with previous studies [2, 11-13]. ANC and NEUTRO detected engraftment earlier in Auto than in Allo.
Many different methods for detection of engraftment after HSCT have been reported [14-17]. One of the advantages of the markers put forth by this study is that one can simply use the data from daily CBC without additional work, cost, or time. Because there is currently no available method to calibrate cell population data, it is recommended that each laboratory adjust the parameter values according to the characteristic pattern after HSCT.
In conclusion, for an early prediction of engraftment after HSCT, NEUTRO should be used as a base marker and MONO as a supplementary marker. When jointly used, these new markers provide an engraftment prediction of approximately 4 days earlier than the conventional marker of ANC >500/µL.
 XML Download
XML Download