

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Disseminated intravascular coagulation (DIC) is a clinicopathological syndrome characterized by intravascular fibrin formation as a result of systemic activation of the coagulation pathway [1]. Intravascular fibrin formation is enhanced by dysfunction of natural anticoagulant systems, such as antithrombin and protein C systems, during the active course of DIC. Since natural anticoagulants can restore dysfunctional anticoagulant systems, recombinant anticoagulant proteins including antithrombin and activated protein C have been investigated for the treatment of DIC [2].
Plasma levels of antithrombin, protein C, and protein S tend to be markedly reduced in patients with severe DIC [3]. Moreover, antithrombin and protein C deficiency are common in DIC patients with poor prognosis [4, 5]. Therefore, plasma levels of natural anticoagulants can be used in the diagnosis and prognosis of DIC. Currently, a scoring system proposed by the subcommittee of International Society of Thrombosis and Haemostasis (ISTH) includes 4 routine laboratory tests: platelet count, prothrombin time (PT), fibrin-related marker level, and fibrinogen [6].
Protein Z is a natural anticoagulant that activates protein Z-dependent protease inhibitor, which in turn inhibits factor X [7]. Although low levels of protein Z are reported in thrombotic conditions [8], to the best of our acknowledge, there is no report on plasma levels of protein Z in DIC.
DIC can occur in various underlying diseases such as sepsis, malignancy, and liver disease [6, 9], and the onset mechanisms of DIC differ depending on the underlying diseases. For example, tissue factor (TF) expressed by tumor cells usually initiates coagulation activation in malignancy, while inflammatory cytokines are the main triggers for coagulation activation in sepsis [10]. Therefore, the diagnostic and prognostic value of laboratory results may differ depending on the underlying diseases [9].
Part 1 of this study investigated the diagnostic values of natural anticoagulants (antithrombin, protein C, protein S, and protein Z) in DIC. Since we found that antithrombin and protein C had higher prognostic value than protein S and protein Z, in part 2, we prospectively assessed the prognostic value of antithrombin and protein C levels according to the underlying diseases in a large study population.
Go to : 
METHODS
1. Study design
Part 1 of the study included 126 patients who were clinically suspected of having DIC. To screen for good prognostic indicators of DIC, 4 candidate anticoagulant proteins, namely antithrombin, protein C, protein S, and protein Z, were assessed.
Then, a larger population study was performed to validate the prognostic values of antithrombin and protein C in part 2 of the study, because these proteins were identified to relate to prognosis in part 1 of the study. The plasma levels and prognostic value of antithrombin and protein C were analyzed in 1,846 patients clinically suspected of having DIC according to the underlying diseases.
This study was approved by the Institutional Review Board of Seoul National University Hospital. We reviewed the test results and medical records to determine whether the patients were clinically consistent with the ones who were diagnosed with DIC. The characteristics of patients, including age, gender, underlying disease, and laboratory test results, are presented in Table 1. We defined overt-DIC using an ISTH Subcommittee cumulative score of 5 or above [6]. For the fibrin-related marker, a D-dimer level of <0.4, 0.4-4.0, and >4.0 µg/mL was considered as no increase, moderate increase, and strong increase, respectively.
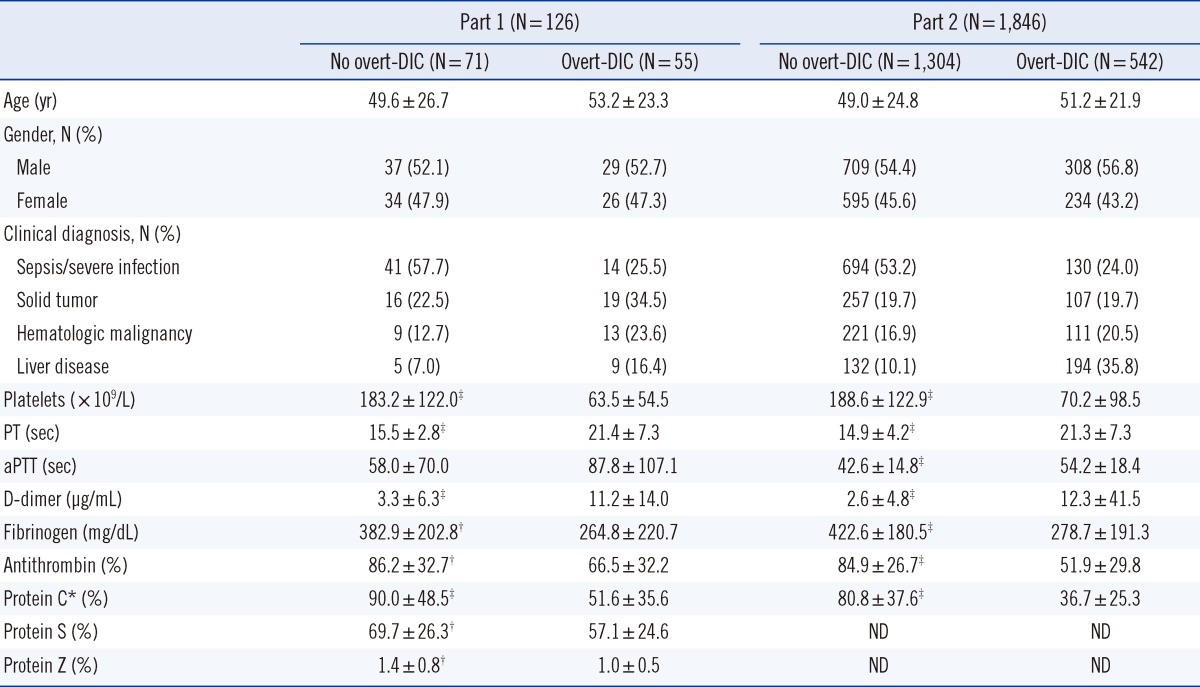
Table 1
Characteristics of the study population
The values are presented as the mean and standard deviation or number of patients and percentage in parentheses.
*Data on Protein C were missing in 2 patients without overt-DIC and in 1 patient with overt-DIC in part 1 of the study; †P<0.05; ‡P<0.001 versus overt-DIC.
Abbreviations: PT, prothrombin time; aPTT, activated partial thromboplastic time; ND, not done; DIC, disseminated intravascular coagulation.
![]()
2. Blood samples and assays
Peripheral blood was collected in commercially available vacutainers: 3.2% sodium citrate tubes (Becton Dickinson, San Jose, CA, USA) for the coagulation test and EDTA tubes (Becton Dickinson) for platelet count. Platelet count was measured on EDTA anticoagulated blood using a XE-2100 system (Sysmex, Kobe, Japan). The PT, activated partial thromboplastin time (aPTT), fibrinogen, and D-dimer levels were assayed on an ACL 3000 (Beckman Coulter Inc., Fullerton, CA, USA). Antithrombin and protein C levels were also determined by chromogenic assay using an ACL 3000 (Beckman Coulter Inc.). The free protein S antigen level was measured using a Free Protein S kit (Instrumentation Laboratory Company, Lexington, MA, USA). Protein Z levels were measured using a commercial ELISA kit (Zymutest Protein Z; Hyphen BioMed, Neuville-sur-Oisa, France) according to the manufacturer's instructions.
3. Statistical analysis
All statistical analyses were carried out using the SPSS 19.0.0 statistical package (SPSS Inc., Chicago, IL, USA). Continuous data of all parameters are given as median values and ranges, and data were compared using the t-test. The relationships between categorical variables were compared by the chi-square test. The area under the ROC curves (AUC) was compared to predict the prognostic power of each variable. Cumulative survival curves were analyzed using Kaplan-Meier survival analysis. The hazard ratios, as measures of the relative risk of the 28-hospital day mortality rate, were estimated with Cox regression analysis, and the 95% confidence interval (CI) was computed. We included age and gender as covariates. The optimal cutoff value was determined with ROC curve analysis using MedCalc 12.3.0.0 (MedCalc Software, Mariakcox, Belgium). Two-sided P values <0.05 were considered statistically significant.
Go to :
RESULTS
1. Diagnostic value screening of antithrombin, protein C, protein S, and protein Z for DIC
In part 1 of the study, overt-DIC was diagnosed in 55 of the 126 patients according to the ISTH diagnostic criteria (Table 1). There was no significant difference in age, gender, or clinical diagnosis between patients with and without overt-DIC. There was a significant difference in platelet count, D-dimer, and fibrinogen, but not in aPTT between patient groups. Plasma levels of the 4 anticoagulants, namely antithrombin, protein C, protein S, and protein Z, were significantly lower in the overt-DIC patients than in patients without overt-DIC. The AUCs (95%CI) were 0.676 (0.586-0.758), 0.744 (0.657-0.818), 0.637 (0.546-0.722), and 0.633 (0.542-0.718) for antithrombin, protein C, protein S, and protein Z, respectively. Among them, the AUCs between protein C and protein Z showed significant difference (P<0.05) (Fig. 1).
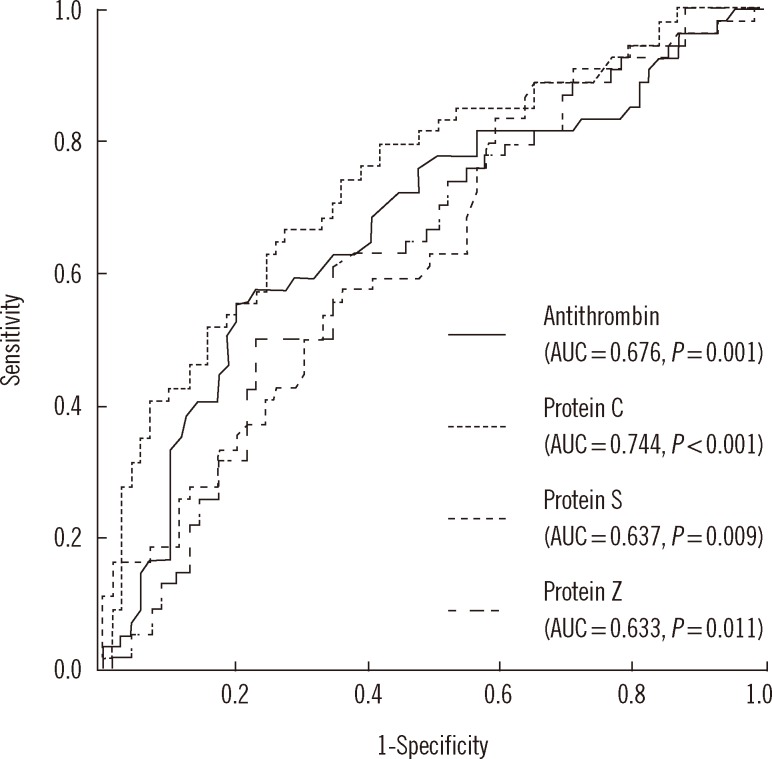 | Fig. 1Receiver operating characteristic curve analyses and calculated values of area under the curves (AUC) for antithrombin, protein C, protein S, and protein Z for prediction of overt-disseminated intravascular coagulation. The AUCs between protein C and protein Z showed significant difference (P<0.05).
|
2. Prognostic value validation of antithrombin and protein C
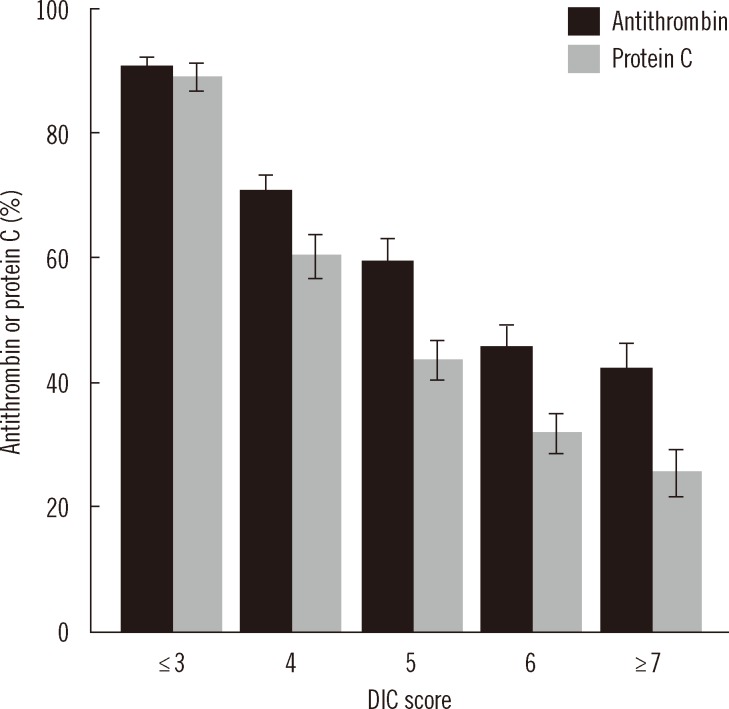
In part 2 of the study, overt-DIC was diagnosed in 542 of the 1,846 patients (Table 1). Antithrombin and protein C levels were also significantly lower in patients with overt-DIC (51.9±29.8, 36.7±25.3) than in patients without overt-DIC (84.9±26.7, 80.8±37.6) (P<0.001). To determine the relation of plasma antithrombin and protein C levels with DIC severity, we analyzed the mean values of antithrombin and protein C according to DIC scores (Fig. 2). As the DIC score increased, both antithrombin and protein C levels gradually decreased (P<0.001). The mean levels of protein C were lower than those of antithrombin in patients with high DIC scores (P<0.001 for score 5, 6, and over 7).
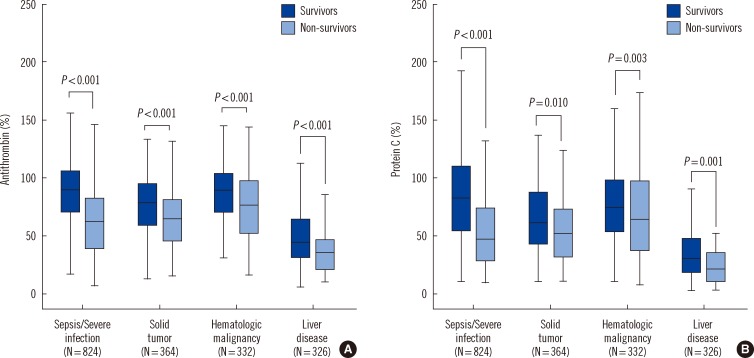
To assess the changes in antithrombin and protein C levels according to the underlying diseases, we divided the patient population into 4 groups on the basis of the underlying disease; sepsis/severe infection (n=824), solid tumor (n=364), hematologic malignancy (n=332), and liver disease (n=326) (Fig. 3). The median levels of both antithrombin and protein C in the complete patient population were lower in non-survivors (59.0, 47.0) than in survivors (80.0, 67.0) (P<0.001). When analyzed separately, antithrombin and protein C levels of non-survivors were markedly lower in the liver disease group (35.5, 21.5) compared to the other underlying diseases (59.0, 47.0 for sepsis/severe infection, 62.0, 52.0 for solid tumor, and 75.0, 64.0 for hematologic malignancy) (P<0.001). Similarly, antithrombin and protein C levels were significantly lower in the liver disease group (43.5, 30.0) than others (90.0, 83.0 for sepsis/severe infection, 76.0, 61.0 for solid tumor, and 89.0, 74.5 for hematologic malignancy) in survivors (P<0.001).
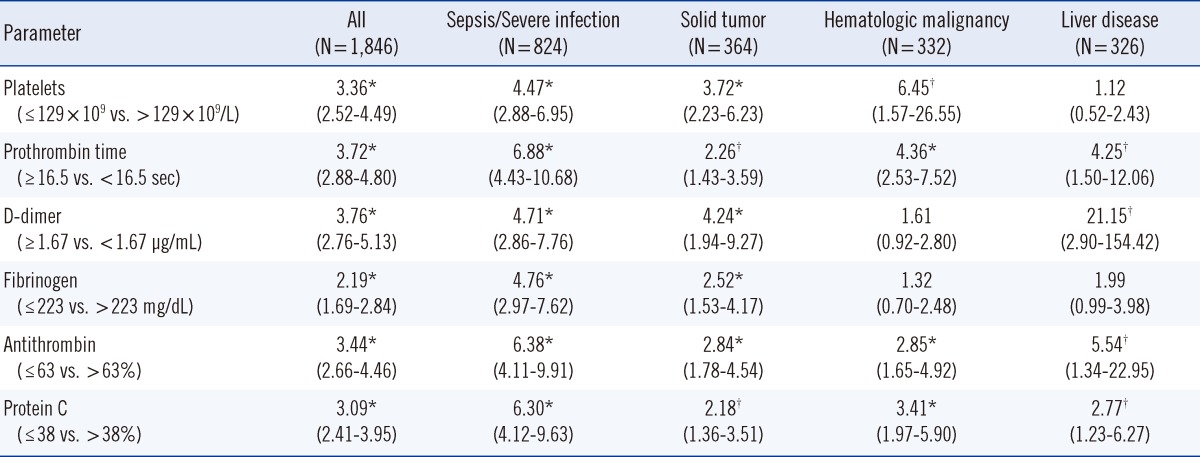
Kaplan-Meier survival analysis was performed to assess the prognostic value of antithrombin and protein C levels (Fig. 4). Cutoff values were set as the values at which the prognostic power to predict 28-day mortality was highest. Patients with low antithrombin levels (≤63%) had a low cumulative survival rate compared to those with high antithrombin levels (>63%) (P<0.001) (Fig. 4A). There was also a significant difference in the cumulative survival rate between patients with low (≤38%) and high protein C levels (>38%) (P<0.001) (Fig. 4B). To validate the prognostic value of antithrombin and protein C in each underlying disease, age- and sex-adjusted Cox regression analyses were performed (Table 2). In all patients, D-dimer showed the highest hazard ratio (3.76; 95% CI, 2.76-5.13), while fibrinogen showed the lowest hazard ratio (2.19; 95% CI, 1.69-2.84). The hazard ratios of antithrombin (3.44; 95% CI, 2.66-4.46) and protein C (3.09; 95% CI, 2.41-3.95) were comparable to that of platelet count (3.36; 95% CI, 2.52-4.49). In the sepsis/severe infection group, PT showed the highest hazard ratio (6.88; 95% CI, 4.43-10.68), while antithrombin (6.38; 95% CI, 4.11-9.91) and protein C (6.30; 95% CI, 4.12-9.63) also showed superior hazard ratios to D-dimer (4.71; 95% CI, 2.86-7.76). In the hematologic malignancy group, the hazard ratio of the platelet count was highest (6.45; 95% CI, 1.57-26.55). In the liver disease group, the hazard ratio of D-dimer was highest (21.15; 95% CI, 2.90-154.42) and that of antithrombin was also high (5.54; 95% CI, 1.34-22.95).
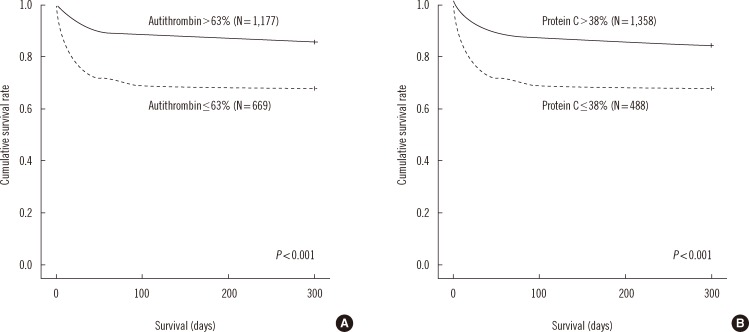 | Fig. 4Kaplan-Meier survival analysis stratified for (A) antithrombin and (B) protein C in all patients. The cutoff values were set as the values at which the prognostic power to predict 28-day mortality was highest.
|
Go to :
DISCUSSION
This study demonstrated that plasma levels of 4 candidate anticoagulant proteins, namely antithrombin, protein C, protein S, and protein Z, were significantly lower in the patients with overt-DIC than in the patients without overt-DIC. Among these factors, protein C showed highest diagnostic value for overt-DIC. Since natural anticoagulants play an essential role in reducing hypercoagulation associated with DIC, plasma levels of anticoagulants should decrease during active DIC. Besides its consumption by the body, degradation of anticoagulants by elastase released from activated neutrophils and impaired liver synthesis may also play a role in reducing plasma anticoagulant levels [11]. The reduced levels of anticoagulants may contribute to fibrin formation, resulting in aggravation of DIC. Many clinical trials on recombinant thrombomodulin and activated protein C have been conducted [2, 12], and our results support the role of anticoagulants in DIC.
Several studies have reported that plasma levels of antithrombin and protein C are significantly lower in patients with poor prognosis [3-5]. However, these results were based on a relatively small number of patients. Our results demonstrate significant prognostic value of antithrombin and protein C in a large population consisting of 1,846 patients. This allowed us to validate and clarify the prognostic value of antithrombin and protein C, suggesting that these proteins may be useful as prognostic markers in clinical practice.
Interestingly, our study showed that the prognostic value of antithrombin and protein C were higher in patients with sepsis and severe infection than in those with other underlying diseases (Table 2). The triggering factor for coagulation activation is known to differ depending on the underlying disorder of DIC. Inflammatory cytokines and bacterial lipopolysaccharide (LPS) mainly trigger the coagulation activation in sepsis [10], while TF expressed by tumor cells initiates coagulation activation in malignancy [13]. In an LPS-induced DIC model, heavy inflammatory responses occurred and more aggravated multi-organ failure was seen compared to TF-induced DIC [10, 14].
Since patients with liver disease have impaired coagulation function due to reduced synthesis of coagulation factors and anticoagulants, accurate diagnosis of overt-DIC can be difficult [15]. The fibrin-related marker, D-dimer, was the best prognostic marker of liver disease of all factors analyzed in our study. Compared to other markers such as platelet count, PT, and fibrinogen levels, the antithrombin level was found to have high prognostic value. Therefore, antithrombin may be a suitable prognostic marker of DIC especially in patients with liver disease.
Protein Z and protein Z-dependent protease inhibitor are a newly characterized anticoagulant system [16]. Both factors play a role in the rapid inactivation of factor Xa. To the best of our knowledge, our study is the first to demonstrate that plasma protein Z levels are significantly lower in patients with overt-DIC compared to patients without overt-DIC. However, the diagnostic value of protein Z for overt-DIC was significantly lower than that of protein C (P<0.05). Considering that protein Z acts with protein Z-dependent protease inhibitor, simultaneous measurement of protein Z-dependent protease inhibitors may be required for accurate evaluation of DIC.
Protein C plays a role in preventing inflammatory responses as well as in inhibiting coagulation activation [17]. The protein C signaling pathway prevents apoptosis of endothelial cells, increases endothelial barrier function, and selectively down-regulates inflammatory genes. Therefore, protein C deficiency in DIC may be predictive of aggravated inflammatory processes as well as coagulopathy. Similarly, antithrombin also inhibits inflammatory processes by downregulating thrombin, which induces various inflammatory responses through stimulation of the nuclear factor kappa-light-chain-enhancer of activated B cells [18]. Hence, antithrombin deficiency in DIC also aggravates the inflammatory response. Taken together, these results indicate that both protein C and antithrombin deficiencies in DIC can promote inflammatory process of DIC through loss of their anti-inflammatory functions.
In summary, protein C exhibit best discriminating power for overt-DIC among 4 candidate anticoagulant proteins. Antithrombin and protein C related with DIC score and showed significant prognostic power, especially in patients with sepsis/severe infection. Antithrombin also showed high prognostic value in patients with liver disease.
In conclusion, since decreased plasma anticoagulant levels reflect florid consumption of physiologic defense systems against DIC-induced hypercoagulation, plasma antithrombin and protein C levels may be powerful prognostic markers of DIC, especially in patients with sepsis and severe infection.
Go to :
 XML Download
XML Download