

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Blood stream infections (BSIs) are associated with high rates of morbidity and mortality ranging from 20% to 70% worldwide [1, 2, 3, 4]. BSIs are the 10th leading cause of death in the United States, accounting for 6% of all deaths [5]. An estimated 135,000 patients die each year of sepsis-associated complications in Europe [6]. Blood culture systems, which detect viable microorganisms in blood, are the current gold standard for BSI diagnosis. Patients with sepsis, defined as a clinical infection resulting in a systemic inflammatory response, account for only about one third of the total positive cultures [7]. Although blood cultures are currently performed with continuous-monitoring blood culture systems (CMBCSs), several factors such as poor timing of collection, insufficient blood volumes, and the presence of antibiotics in the samples reduce the sensitivity of blood cultures [7, 8]. The main limitation of utilizing blood culture method is the vast amount of time required, as treating patients with empirical therapies before the blood culture analysis is complete may not serve to cure the illness. Kumar et al. [9] reported that the mean survival rate decreased by 7.6% every hour that effective antibiotic therapy was delayed following the onset of sepsis-related hypotension.
Recently, several PCR-based commercial assays that target a panel of clinically relevant bacterial and fungal bloodstream pathogens have been developed. Two types of commercial PCR-based assays are most common. The first type is designed for culture-positive samples. Examples of this type of assay are the peptide nucleic acid fluorescence in situ hybridization-based assay (AdvanDx, Woburn, MA, USA) [10], Hyplex Blood Screen (BAG, Lich, Germany) [11], and Prove-it Sepsis (Mobidiag, Helsinki, Finland) [12]. The second type is designed for direct blood samples. Examples of this type of assay are SepsiTest (Molzym, Bremen, Germany) [13] and Vyoo (SIRS-Lab, Jena, Germany) [14]. The PCR-based reverse blot hybridization assay (PCR-REBA, REBA Sepsis-ID; M&D, Wonju, Korea) was developed to rapidly detect bacterial and fungal pathogens and antimicrobial resistance genes in blood culture samples [15]. It uses pan-probes to distinguish gram-positive bacteria (GPB), gram-negative bacteria (GNB), and fungi. In addition, it uses probes for antibiotic resistance genes (i.e., the mecA gene of methicillin-resistant Staphylococcus spp. and the vanA and vanB genes of vancomycin-resistant enterococci).
The aim of this study was to evaluate the REBA Sepsis-ID test for rapid and accurate detection of pathogens and antimicrobial resistance genes in blood.
METHODS
This study was approved by the Institutional Review Board (CR312055) of Yonsei University Severance Hospital.
1. Collection of blood culture bottles
Three-hundred positive blood culture (PBC) and 1,100 negative blood culture (NBC) samples from patients with a delta neutrophil index (DNI) greater than 2.7% [16] were consecutively collected at Wonju Severance Christian Hospital from March to July in 2013. To avoid the redundancy of enrolled samples, only one blood culture sample per patient was allowed. The enrolled blood culture samples were simultaneously tested with the PCR-REBA and conventional microbiological tests. The overall positive rate of blood culture in this study period was 7.46% (1,640/21,979).
The PBC samples were eligible for enrollment if they had been flagged positive by BACTEC FX (Becton Dickinson, Sparks, MD, USA) or BacT/ALERT 3D (bioMérieux, Durham, NC, USA) with a positive Gram stain. The PBC bottles were then removed from the CMBCS and a 1,000 µL aliquot of the culture-broth mixture was aseptically collected by using a syringe and needle. The aliquot was then divided into halves. The first half (500 µL) was used to perform a Gram stain and subcultured on sheep blood agar and MacConkey agar, which were incubated at 35℃ for 24-48 hr in 5% CO2, and the second half (500 µL) was kept at -20℃ for subsequent DNA extraction.
NBC samples were used if culture results were negative for five days of incubation in CMBCSs. After the blood culture bottles were removed from the CMBCS, 500 µL of blood suspension was collected and kept at -20℃ for subsequent DNA extraction. All the NBC bottles were incubated at 35℃ until PCR results were obtained. For the NBC samples with a positive real-time PCR result, 1,000 µL of blood suspension was used to inoculate routine subculture media (sheep blood agar, chocolate agar, and Sabouraud dextrose agar), and incubated at 35℃ under 5% CO2 for five days. For slow-growing bacteria, another 1,000 µL of blood suspension was used to inoculate special subculture media (plating count agar media [Becton Dickinson] [17] and Reasoner's 2A agar media [Becton Dickinson] [18]), which was incubated at 20℃ low temperature incubator. Additionally, the remaining blood suspension was used to inoculate Luria-Bertani [19] and brain heart infusion broths (Becton Dickinson), which were incubated at 37℃ incubator. Colonies isolated from the special subculture media and NBC samples that were positive by real-time PCR were confirmed by bacterial 16S rRNA and fungal 18S to 5.8S internal transcribed sequence analysis. The amplicons were sequenced by Xenotech Company (Daejeon, Korea). The conventional identification test and antimicrobial susceptibility test were done by using the MicroScan system (Siemens Healthcare Diagnostics, Sacramento, CA, USA).
2. DNA preparation
To prepare DNA templates from the 300 PBC and 1,100 NBC samples, DNA was extracted by using the following procedure. A 200 µL aliquot of the blood was mixed with 1,000 µL of erythrocyte lysis buffer (ELB) (Sigma, St. Louis, MO, USA) at room temperature for 10 min to disrupt erythrocytes. The supernatant was then removed after centrifugation at 13,000 g for 5 min. The pellet was washed with 1,000 µL of ELB to completely remove the erythrocytes and centrifuged under the same conditions. One hundred microliters of ELB was added to the pellet, which was then frozen and thawed twice. One hundred microliters of DNA extraction solution (M&D) was added to the mixture, and it was boiled for 15 min. After centrifugation at 13,000 g for 10 min, the supernatant was used as a DNA template for PCR.
3. PCR amplification
Conventional PCR amplification was performed according to the manufacturer's instructions to evaluate the PBC samples. TaqMan real-time PCR assays were carried out by using Real-GP (gram-positive), -GN (gram-negative), and -CAN (Candida) real-time PCR kits (M&D) according to the following procedure to evaluate the NBC samples. The reaction mixture contained 10 µL of real-time PCR mixture, 5 µL of primer and probe mixture, 0.04 µL of 50× ROX reference dye, 5 µL of sample DNA, and sterile distilled water to give a final volume of 20 µL. The thermal cycling conditions were: 10 min at 94℃, followed by 40 cycles of 30 sec at 94℃ and 30 sec at 60℃. Each TaqMan real-time PCR assay included a positive control and an internal control, which was used to control for the effect of PCR inhibitors in the reaction. The cycle threshold (CT) values resulting from reactions in the master mix with and without specimen were compared. The bacterial load was quantified by determining the CT, the number of PCR cycles required for the fluorescence to exceed a value significantly higher than the background fluorescence. All reactions were performed by using an ABI 7500 FAST instrument (Applied Biosystems, Foster City, CA, USA). The CT value was analyzed by using 7500 Software version 2.0.4 (Applied Biosystems). Fifteen PBC samples were evaluated by using real-time PCR TaqMan assay as a pilot study before evaluating the NBC samples. The CT values resulting from this pilot study ranged from 11 to 20.94 cycles. The real-time PCR assay was defined as positive if the CT value was below 30.0.
4. PCR-reverse blot hybridization assay
The REBA Sepsis-ID test was performed according to the standard protocol provided by the manufacturer [15]. The membrane used in the REBA Sepsis-ID test contained DNA probes for GPB, including Staphylococcus aureus, Staphylococcus spp., Streptococcus pneumoniae, Streptococcus spp., Enterococcus spp., and Mycobacterium spp.; DNA probes for GNB including Escherichia coli, Klebsiella pneumoniae, Citrobacter freundii, Salmonella spp., Shigella spp., Haemophilus influenzae, Pseudomonas aeruginosa, and Acinetobacter baumannii; DNA probes for Candida species including C. albicans, C. tropicalis, C. glabrata, C. parapsilosis, and C. krusei; and DNA probes for antimicrobial resistance genes including mecA, vanA, and vanB. Indicator lines on the REBA strips were evaluated by using a template provided with the kit. A universal control band was used to evaluate the intensity of faint bands (only the bands with color intensity equal to or greater than that of the control band were considered positive). The results indicated by band patterns on the developed strips specific for each species and resistance gene were compared to the conventional microbiologic results.
5. 16S rRNA sequence analysis
All the isolates and PCR amplicons with discrepant results between the REBA Sepsis-ID test and conventional methods were subjected to 16S rRNA sequence analysis. The REBA Sepsis-ID test, bacterial 16S rRNA, and fungal 18S to 5.8S internal transcribed sequence analysis were performed on these samples. The results were compared with those of blood cultures.
RESULTS
1. Positive blood culture samples -monomicrobial bacteremia
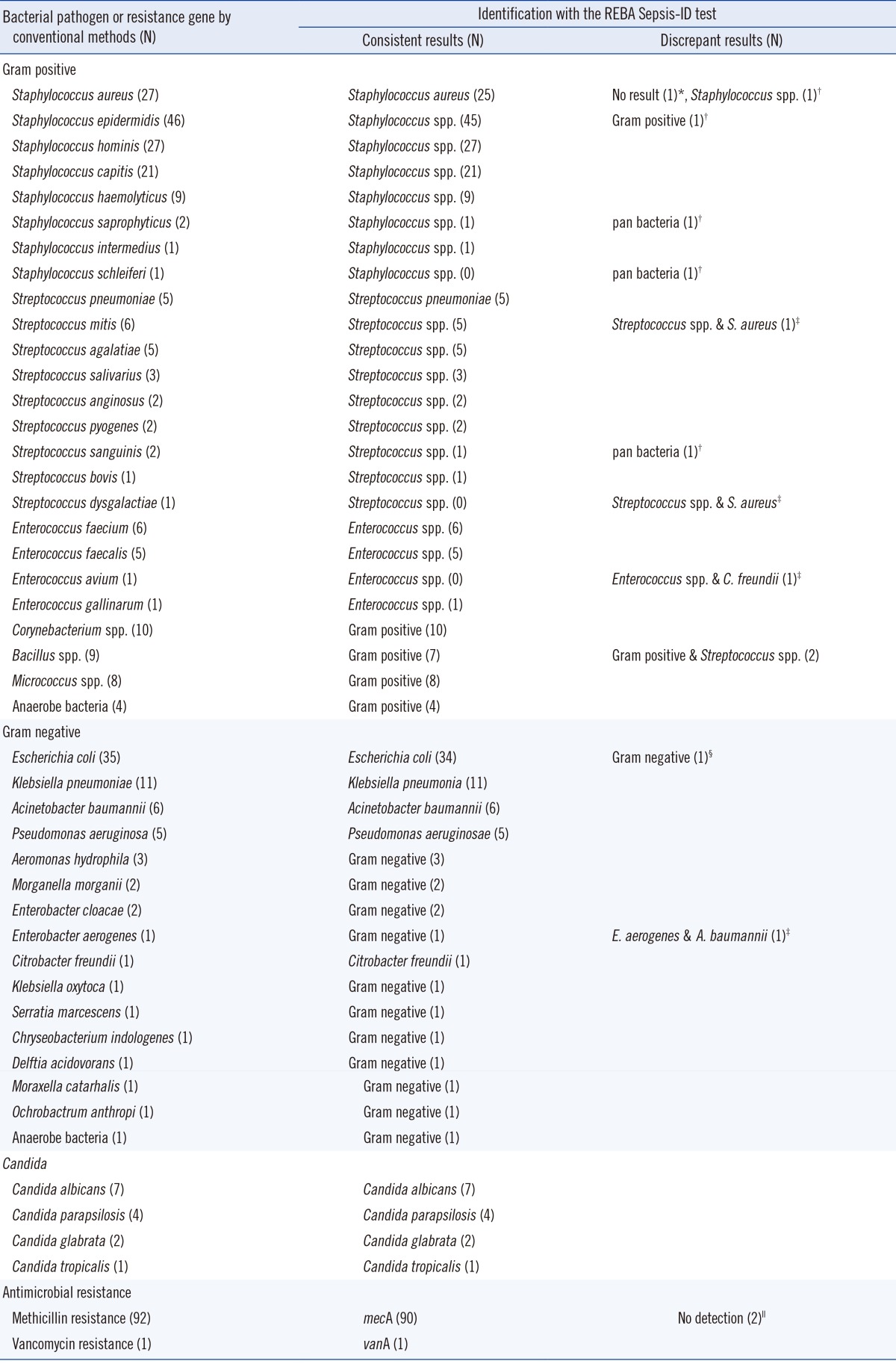
Two hundred eighty-eight of 300 PBC samples contained a single organism as determined by the culture method. Of the monomicrobial PBC samples, 69.8% (201/288) contained GPB including S. aureus, coagulase-negative Staphylococcus (CoNS), S. pneumoniae, Streptococcus spp., Enterococcus spp., and anaerobic GPB. An additional 25.3% (73/288) contained GNB including E. coli, K. pneumoniae, A. baumannii, P. aeruginosa, C. freundii, and anaerobic GNB. A total of 4.9% (14/288) contained Candida spp. including C. albicans, C. parapsilosis, C. glabrata, and C. tropicalis (Table 1). Two of 27 S. aureus and three of 103 CoNS isolates gave discrepant results between the culture method and the REBA Sepsis-ID test. One S. aureus case was not identified by PCR amplification, and another S. aureus case was not identified as the species level. Three CoNS cases were identified at the pan-GP or pan-bacteria level by the REBA Sepsis-ID test. All five S. pneumoniae isolates were correctly identified. Three of 22 Streptococcus spp. showed discrepant results between culture and the REBA Sepsis-ID test. The presence of both Streptococcus spp. and S. aureus was indicated in two of these discrepant samples by the REBA Sepsis-ID test. Subsequent 16S rRNA sequence analysis confirmed the presence of two isolates in each sample. Twelve of 13 Enterococcus spp. were concordant. One sample resulted in two bands corresponding to Enterococcus spp. and C. freundii by the REBA Sepsis-ID test despite only Enterococcus avium being isolated. Subsequent 16S rRNA sequence analyses confirmed the presence of E. avium and C. freundii in the blood culture sample. The other 27 GPB including 10 Corynebacterium spp., 9 Bacillus spp., 8 Micrococcus spp., and 4 anaerobic GPB were not included in the REBA probes. PCR products from all but two samples hybridized with the pan-GP probes. The agreement rate between the culture method and the REBA Sepsis-ID test for GPB and GNB was 94.5% (190/201) and 97.3% (71/73), respectively. Three GPB monomicrobial samples were revealed to have more than one isolate by the REBA Sepsis-ID test. E. coli was isolated from one GNB monomicrobial sample, but the PCR product hybridized only with the pan-GN probe. In the only other GNB monomicrobial sample, Enterobacter aerogenes was isolated, and the PCR product hybridized with both of the pan-GN and A. baumannii probes. This sample was confirmed to contain both of E. aerogenes and A. baumannii by 16S rRNA sequence analysis. All 14 Candida species were identified by the REBA Sepsis-ID test.
2. Positive blood culture samples -polymicrobial bacteremia
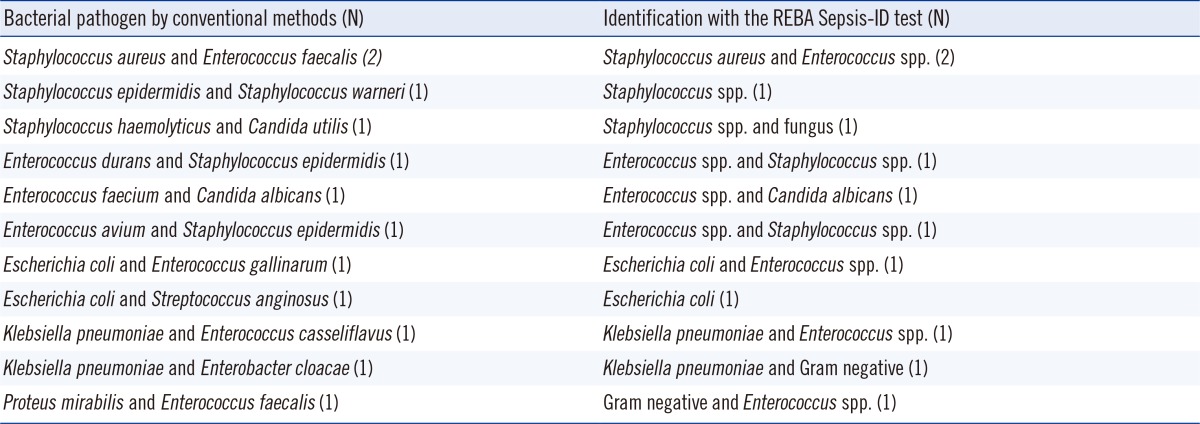
Of the 12 polymicrobial PBC samples, the agreement rate between the culture method and the REBA Sepsis-ID test was 91.7% (11/12). E. coli plus Streptococcus anginosus isolated by the culture method in one case was identified to be only E. coli by the REBA Sepsis-ID test (Table 2).
3. Negative blood culture samples
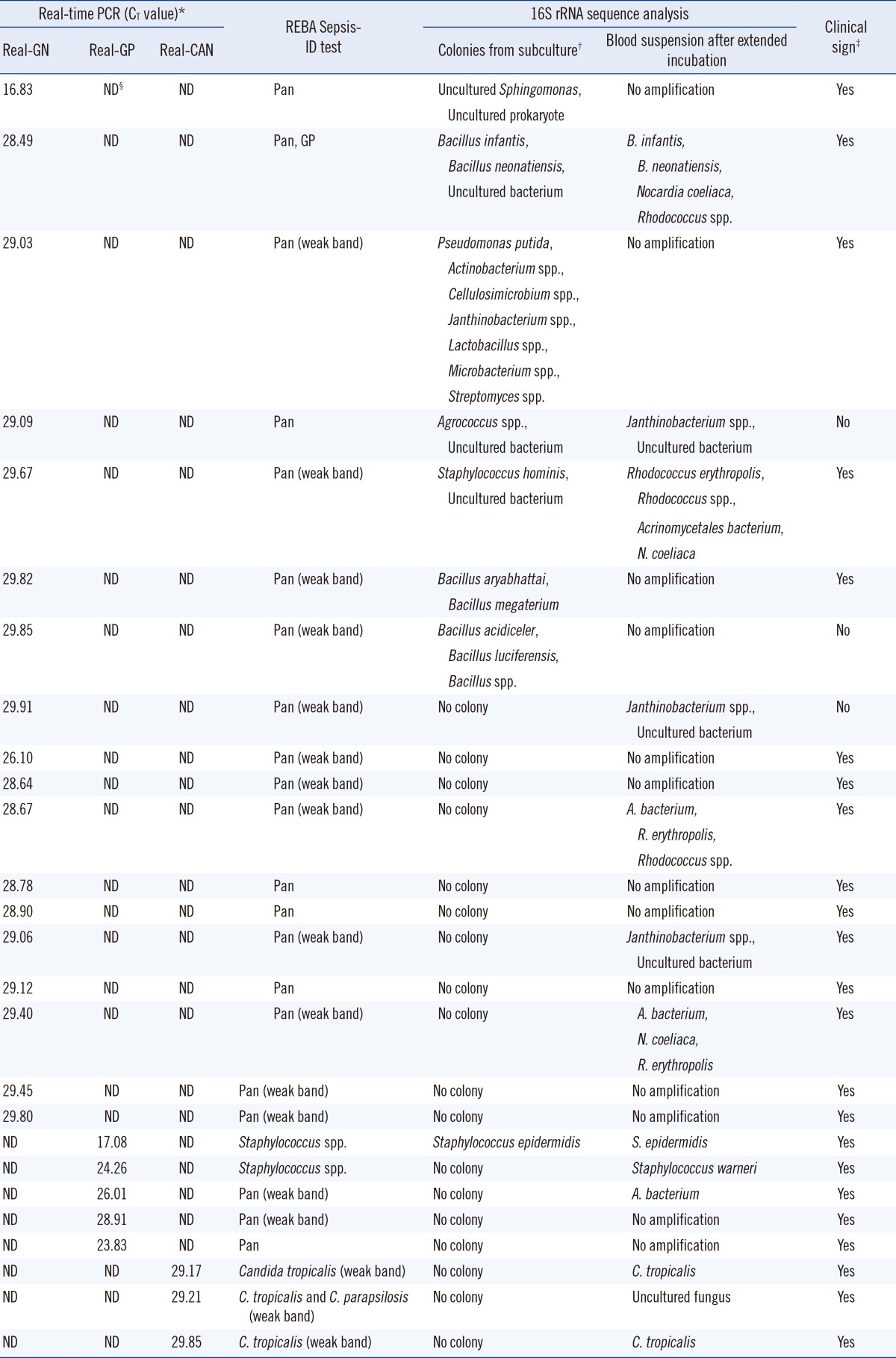
Among the NBC samples, 97.6% (1,074/1,100) had CT values above 30.0. The remaining 2.4% (26/1,100) NBC samples had CT values below 30.0, including four with values less than 25.0, one between 26.0 and 27.0, and 21 between 28.0 and 30.0. Of these samples, 69.2% (18/26) were Real-GN positive, 19.2% (5/26) were Real-GP positive, and 11.5% (3/26) were Real-CAN positive by TaqMan real-time PCR assay (Table 3). Most Real-GP, and Real-GN positive cases produced PCR products that weakly hybridized to the pan-bacteria probe. Isolates from two Real-CAN positive cases were identified as containing C. tropicalis and one was identified as containing C. tropicalis plus C. parapsilosis by the REBA Sepsis-ID test. Thirteen of 26 NBC samples with positive real-time PCR results were not amplified by sequencing reactions. Eight NBC samples produced colonies that grew on subculture media (Table 3). A significant agreement was found between conventional culture method and REBA-Sepsis ID test (kappa coefficient=0.916, P<0.001).
4. Identification of mecA and vanA genes
Ninety of 92 (97.8%) blood culture samples with methicillin-resistant Staphylococcus isolates were mecA positive. MecA was not detected in the two methicillin-resistant Staphylococcus saprophyticus isolates. No mecA genes were identified by PCR-REBA in the 44 methicillin-susceptible Staphylococcus spp. The vanA gene was detected in one blood culture sample, from which vancomycin-resistant Enterococcus was isolated (Table 1).
DISCUSSION
The clinical treatment of bacterial infections with antibiotics depends on the bacterial species, and especially differs among GPB, GNB, and fungal infections. Antibiotic therapies are usually selected empirically until antimicrobial susceptibility test results are completed. Therefore, rapidly identifying pathogens and their resistance genes is important for treating septic patients. Diagnostic methods that can reduce the time to identify a BSI pathogen, and its antimicrobial susceptibility have great potential to improve patient care. Recently, a molecular diagnostic approach was proposed to be advantageous [20, 21]. The advantage of molecular approaches is notable when the infectious agent is fastidious or fungal, when blood culture fails to identify the causative agent, or when a quick diagnosis is needed.
The agreement rates between the conventional culture method and the REBA Sepsis-ID test in identifying GPB, GNB, fungi, and the mecA gene in 300 PBC samples were 94.5%, 97.3%, 100%, and 97.8%, respectively. Steindor et al. [22] reported correct identification of 96.1% of GPB, 89.9% of GNB, and 92.9% of mecA using the PCR-based DNA strip assay, GenoType BC. Results from our PBC samples demonstrated that the overall agreement rate between the culture method and the REBA Sepsis-ID test was high at 95.3%, which was similar to that indicated in other reports [23, 24].
Two monomicrobial PBC samples with discrepant results between culturing and the REBA Sepsis-ID test were proven to have additional S. aureus isolates. In contrast, five samples containing Staphylococcus spp., including S. aureus isolates, were not correctly identified the by the REBA Sepsis-ID test. It is difficult to accurately identify more than one organism in a sample by using the culture method, as additional blind subculturing of PBC samples with positive flagging is not a common practice in clinical laboratories. PCR inhibitors have been an obstacle to obtaining accurate results. Achieving accurate PCR results from blood culture samples is difficult owing to PCR inhibitors in the blood such as sodium polyanetholsulfonate, heme, hematin, hemoglobin, lactoferrin, and IgG [25, 26, 27, 28, 29]. An optimal PCR sample preparation procedure should efficiently lyse resistant bacterial cell walls, including those in GPB, without being too harsh on the DNA released from the cells [30]. Differentiating S. pneumoniae from mitis group streptococci is difficult because of their close genetic relationship [31]. However, the REBA Sepsis-ID test discriminated between S. pneumoniae and other streptococci, including viridians group streptococci.
Poor accuracy in the identification of more than one organism in a sample is a well-known drawback of PCR-based tests. Molecular tests that detect a limited number of targets may report only one species, which can be misleading. Buchan et al. [32] reported that the agreement rate between a reference culture and a microarray-based nucleic acid test for polymicrobial cultures was only 72%. However, the REBA assay in the present study had an agreement rate of 91.7%. REBA may not detect multiple types of bacteria in a blood culture sample owing to technical limitations, such as interference between multiple probes and undetectable concentrations of minor bacterial constituents. The five PBC samples that had a single bacterial species by blood culture contained two isolates as determined by the REBA Sepsis-ID test, which was confirmed by 16S rRNA sequence analysis. The reason that the REBA Sepsis-ID test detected more isolates than the blood culture method is not clear. However, C. freundii was detected by the blood culture method on the day following its detection by using the REBA Sepsis-ID test. This result indicates that the REBA Sepsis-ID test may be able to detect nonviable bacteria or those at a low concentration that is not detectable by CMBCS. Therefore, the REBA Sepsis-ID test may have practical benefits in the clinical setting, particularly for patients on empirical antibiotic treatment before culture results are obtained.
The REBA Sepsis-ID test did not identify two (2.2%) methicillin-resistant S. saprophyticus isolates, which were identified by the conventional method. The two mecA-negative S. saprophyticus isolates were likely methicillin-susceptible organisms. The Clinical and Laboratory Standards Institute interpretive criteria for detecting mecA-mediated resistance in S. saprophyticus may overestimate resistance [33].
Real-time PCR was used to evaluate NBC samples because it reduces the time required to obtain results, decreases contamination during the PCR procedure, and increases PCR sensitivity. Among the 26 NBC samples with real-time PCR positive results in this study, 13 cases were considered false positive results because they were not amplified by sequencing reactions. Matsuda et al. [34] reported that the positivity rate of PCR-hybridization using 500 µL of blood from NBC samples was 10.5% (11/105) and that the 11 culture negative, PCR-hybridization positive samples contained nine CoNS and two GPB species. Steindor et al. [22] evaluated a PCR-based DNA strip assay, GenoType BC, which detects bacteria from PBC samples and emphasized that the assay required abundant bacteria in the blood. Kocoglu et al. [35] reported that of 904 NBC samples, 2.6% were positive by reculture but not by PCR-based methods. They concluded that subculture was valuable in diagnosis using NBC samples, especially when only one set of blood cultures was taken. In this study, using a real-time PCR CT of 30 resulted in a very low positivity rate in NBC samples. Colonies isolated from subculture media may also have been contaminated as the sequence analysis results were not concordant between the blood suspension and colonies. These results suggest that it is not necessary for a clinical laboratory to perform supplemental subculture as a routine work after 5 days of incubation on CMBCS.
Although the REBA Sepsis-ID test will not absolutely replace the conventional culture method, it is likely to rapidly discriminate between PBC and NBC samples and provide clinical information relevant to patients by detecting important pathogens and antimicrobial resistance genes.
 XML Download
XML Download