

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chlamydia trachomatis is a common sexually transmitted microorganism that causes severe ocular and urogenital tract infections. Undiagnosed and untreated infections pose an increased risk of additional infections in other individuals [1, 2, 3, 4]; thus, early and rapid detection is essential in mitigating the transmission of the bacterium. Compared with cell culture, enzyme immunoassay, and immunofluorescence, the amplification of nucleic acids has been the most widely used method for the clinical diagnosis of C. trachomatis infection [5, 6, 7, 8, 9, 10, 11].
Several types of samples, such as urethral and endocervical swabs, semen, and first-void urine samples, can be used for PCR detection of C. trachomatis infection [12, 13, 14]. Generally, the target sequences for amplification include the cryptic plasmid [13, 15], genes for the major outer membrane protein, ribosomal RNA (rRNA), or cysteine-rich proteins [16, 17, 18]. Assays using the cryptic plasmid as a target are 10- to 1,000-fold more sensitive than those targeting genes for the major outer membrane protein or rRNA [18]. Plasmid-based PCR is more sensitive, partly because the cryptic plasmid of C. trachomatis is present at a level of approximately 7 to 10 copies per bacterial cell [19]. Generally, commercial nucleic acid amplification tests-including COBAS AMPLICOR CT/NG and AMPLICOR CT/NG (Roche, Branchburg, NJ, USA) and LCx (Abbott, Abbott Park, IL, USA)-use the conserved region in the cryptic plasmid as a detection target [20, 21, 22].
Previous studies have demonstrated that PCR amplification of nucleic acids may be unreliable owing to the presence of inhibitors in samples, cross-contamination, or inappropriate sample handling leading to the loss of target DNA [23]. Therefore, quality assurance of the testing is critical. First, an appropriate internal quality control (QC) that is coamplified with samples should be included to distinguish false-negative results of one-run PCR [24]. Second, laboratories should participate in external quality assessment (EQA) programs conducted by an independent organization. Such programs are the best means of identifying testing problems and deficiencies and maintaining and improving the quality of laboratory diagnosis [20, 22, 25, 26].
Three kinds of material have been used in clinical applications as a QC for C. trachomatis detection: 1) positive clinical urine specimens have potential infection, problems with stability and storage, and difficulty in detecting C. trachomatis at lower concentrations, which restrict the use of it [20, 22]; 2) simulated specimens (C. trachomatis cultured in McCoy cells or SiHa cells) have factors such as the chemical matrix, physical presentation, and strain types which can affect the EQA results [23, 25]; 3) a plasmid containing a single target sequence of C. trachomatis cannot simulate clinical samples for nucleic acid extraction because C. trachomatis exists within epithelial cells [20, 22, 25].
The present study describes a simple, general approach for constructing a QC material using mammalian HTB-SiHa cells transfected with a recombinant plasmid containing the conserved cryptic plasmid sequence of C. trachomatis. Then, the QC materials were used for EQA study, and the results were analyzed to illustrate whether it could be a noninfectious, stable QC material with sufficient volume for PCR detection of C. trachomatis.
METHODS
1. Preparation of epithelial cells transfected with a recombinant plasmid containing the sequence of C. trachomatis
Cultured C. trachomatis (kindly provided by Professor Anping Ni at the Peking Union Hospital, China) was used as a template to amplify five fragments in a first-round reaction. The five pairs of primers corresponded to the cryptic plasmid of C. trachomatis (GenBank accession no. X07547: nt178-610, 1219-1993, 2471-3260, 5239-5864, 6722-7499) and are the most commonly used targets for the PCR detection of C. trachomatis. The amplicons were used as targets in overlap PCR, in which the first three amplified fragments and the last two amplified fragments were ligated. The two purified aimed fragments that resulted were ligated into pTARGET vector (Promega, Madison, WI, USA) and pGEM-T Easy vector (Promega), respectively. These recombinant plasmids were then excised by using the SalI and NotI restriction enzymes simultaneously to produce a recombinant plasmid, pTARGET-CT.
Transfection of the recombinant plasmid pTARGET-CT into mammalian HTB-SiHa cells (kindly provided by the Shanghai cell bank of the Chinese Academy of Science) was performed by using Lipofectamine 2000 reagent (Invitrogen, Carlsbad, CA, USA) according to the manufacturer's instructions. The cells were grown in DMEM (Hyclone, Logan, UT, USA) with 20% newborn calf serum as the final form for the control materials. The cultivated SiHa cells transfected with pTARGET-CT were tested using two commonly used commercial C. trachomatis DNA PCR fluorescence quantitative diagnostic kits (PG Biotech, Shenzhen, China; DaAn Gene, Guanzhou, China). Amplification and detection were performed using the same real-time PCR detection system.
Stability assessments for time and temperature were performed for the cultivated SiHa cells containing pTARGET-CT. The control materials were serially diluted 10-fold with DMEM containing 20% newborn calf serum to 3.21×106, 3.21×105, and 3.21×104 copies/mL. The samples were then incubated at 4℃, 37℃, and room temperature for various periods of time. For each dilution, a single batch was separated into 40 aliquots in individual time-point samples of 0.5 mL. The samples were then incubated at 4℃, 37℃, and room temperature. Samples were removed at each time point and stored at -80℃. All samples were quantified in duplicate using a C. trachomatis DNA PCR fluorescence quantitative diagnostic kit (PG Biotech). Two samples were stored at -80℃ as controls. The cycle threshold of each PCR was recorded. Time and temperature stabilities were compared across all experiments using a random group of two-factor analysis of variance.
2. Analytical sensitivity of the PG Biotech real-time PCR assay
To evaluate the sensitivity of the control materials, we prepared serial 10-fold (10-2-10-7) dilutions of cultivated SiHa cells in DMEM with 20% newborn calf serum. Each dilution was tested at a single laboratory using the same commercial C. trachomatis DNA PCR fluorescence quantitative diagnostic kit (PG Biotech). All extraction and assay steps were performed according to the manufacturers' instructions. The data were then analyzed to obtain low levels of target material for evaluation of sensitivity at the lower limits of detection.
3. Panel design and EQA scheme of the constructed materials
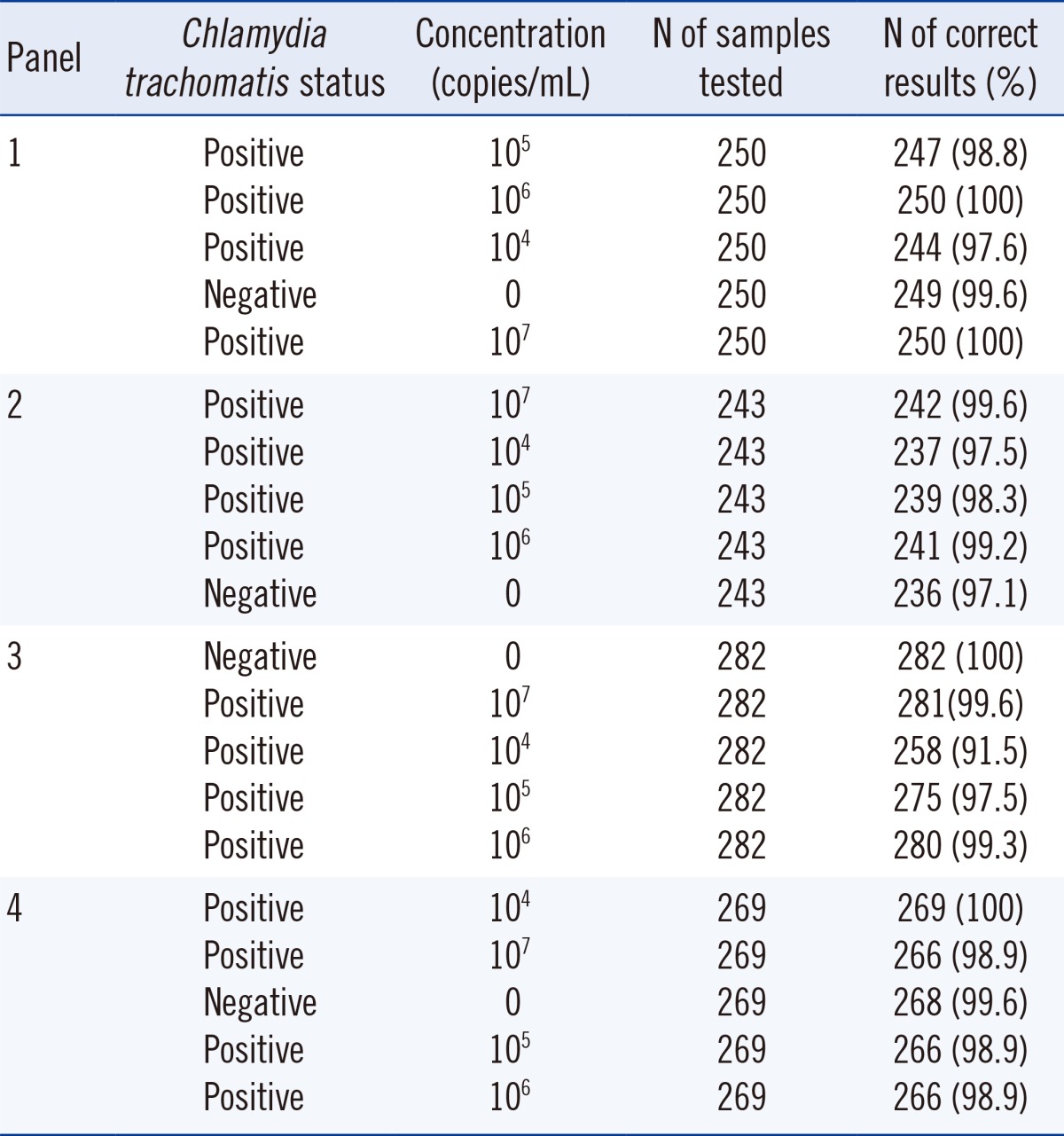
To assess the suitability of samples for detection in clinical laboratories, we designed four proficiency panels according to the measurements of sensitivity of the constructed control materials in real-time PCR assays. Positive samples in the four panels were prepared by spiking 0.5 mL cultivated SiHa cells transfected with pTARGET™-CT into DMEM containing 20% newborn calf serum in a 10-fold dilution series of 104, 105, 106, and 107. One negative sample (0.5 mL) without cultivated SiHa cells was included in each panel. The four panels, totaling 20 samples consisting of 16 positives and 4 negatives, were distributed by the National Center for Clinical Laboratories (NCCL) from 2011 through 2012. The composition and codes of the panels are presented in Table 1. Before distribution to participants, each panel was tested at NCCL by using two commercial C. trachomatis DNA PCR fluorescence quantitative diagnostic kits (PG Biotech and DaAn Gene) to confirm positivity and negativity. According to stability results, the panels were shipped from the production laboratory in Beijing via surface mail at ambient temperature (approximately 10℃ to 20℃) to various laboratories across China. An information sheet with instructions and a questionnaire about detection results, the instruments, and reagents used in the test were also included.
4. Evaluation of results and statistical analysis
The participating laboratories were asked to use an online system to report whether the samples were positive or negative for C. trachomatis. The number of participating laboratories detecting C. trachomatis was calculated in total and by methods per sample. The results were analyzed by the EQA provider. Results obtained from different methods and laboratories were considered together. The Pearson's chi-square test was used for statistical calculations for all panels tested using different kits. P value equal to or less than 0.05 was considered statistically significant.
RESULTS
1. Construction of epithelial cells transfected with the recombinant plasmid containing the C. trachomatis sequence
The recombinant plasmid pTARGET-CT was constructed successfully and analyzed via restriction with SalI and NotI. Two aimed fragments (data not shown) were seen clearly and confirmed through sequencing to contain the corresponding target sequences. The cultivated SiHa cells transfected with pTARGET-CT were tested using two diagnostic kits (PG Biotech and DaAn Gene). Representative amplification curves of these two commercial kits demonstrated strongly positive results for the cultivated cells (data not shown).
Real-time PCR results of the serially diluted samples incubated at different times and temperatures revealed no overall differences (P>0.05) in cycle threshold across the time and temperature parameters. The serially diluted samples were stable at 4℃, 37℃, and room temperature for at least 1 month, demonstrating that the constructed control materials were stable under different temperature conditions and met stability requirements for panel distribution via surface mail at ambient temperature.
2. Analytical sensitivity of the PG Biotech real-time PCR assay
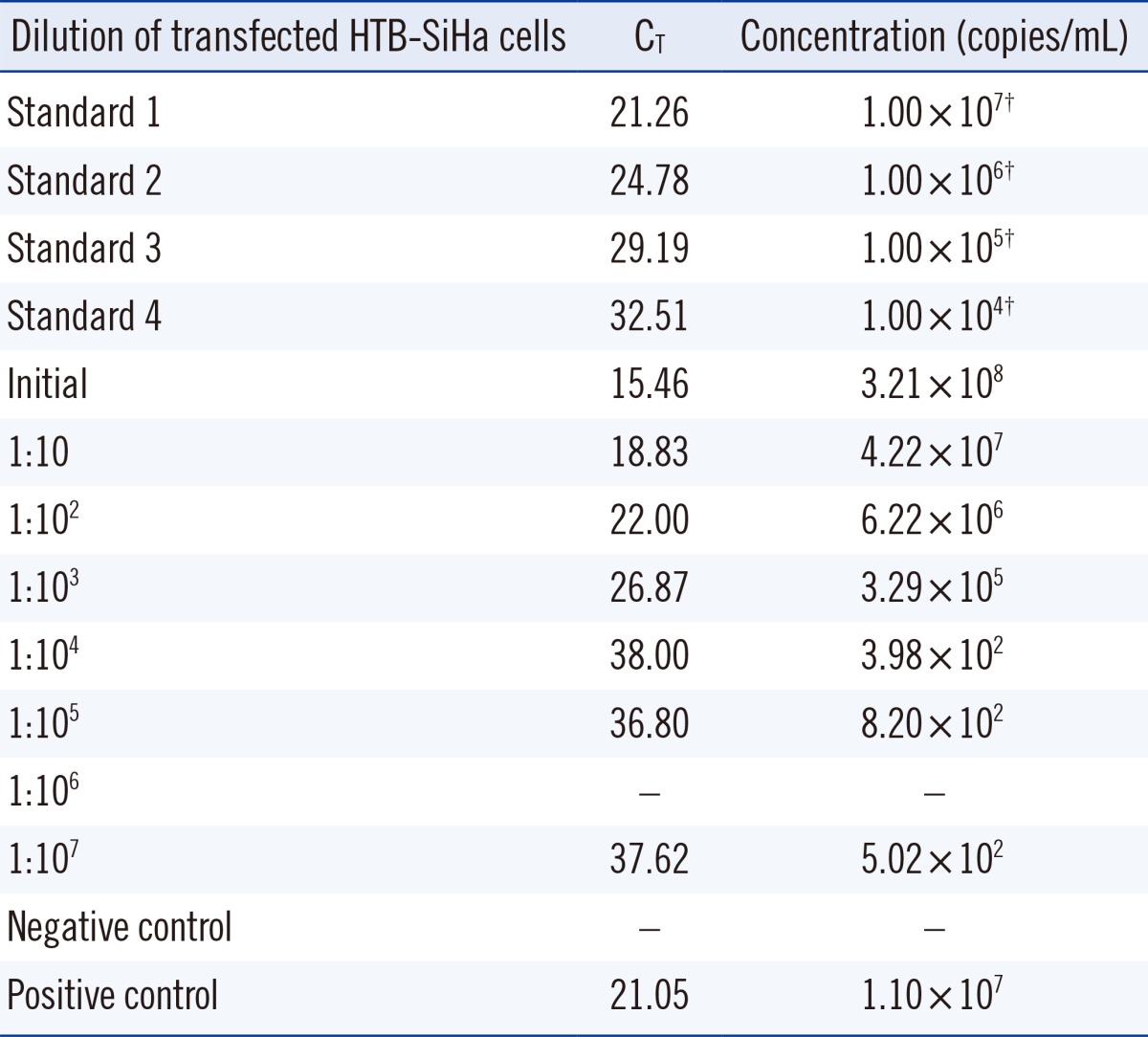
The analytical sensitivity data of the constructed control material in this study using C. trachomatis DNA PCR fluorescence quantitative diagnostic kits (PG Biotech; see Table 1) indicated that the detection concordance of a high-concentration sample (≥3.29×105 copies/mL) was better than that of a low-concentration sample (<3.29×105 copies/mL). The results showed that the original material was approximately 3.21×108 copies/mL. According to the results, the concentrations of the positive samples in the EQA panels were higher than 104 copies/mL.
3. Distribution and response
Panels 1, 2, 3, and 4 were sent to groups of 275, 268, 317, and 304 laboratories, respectively. The median transport time was 3 days via surface mail at ambient temperature. Results received from 250, 243, 282, and 269 participating laboratories (with response rates of 90.9%, 90.7%, 90.0%, and 88.5%), respectively, are shown in Table 2. The total number of data sets returned was 1,044.
4. EQA performance
As shown in Table 1, as the serial dilution of positive samples increased to 107, 106, 105, and 104 copies/mL, the number of data sets reported correctly decreased. Among the 1,044 data sets, 1,005 (96.3%) reported the weakly positive samples (104 copies/mL) correctly, which was lower than the correct reporting of other dilutions (98.4%, 99.3%, and 99.8% for 105, 106, and 107, respectively). The results of all four panels conformed to this pattern, indicating that PCR detection was excellent at higher concentrations of C. trachomatis (Table 2).
For the four negative samples distributed, false-positive results were reported by nine laboratories. The overall proportion of false-positive results was 9/1,044 (0.9%). Seven of nine laboratories in the EQA program used kit B; the remaining laboratories used kit E. The lower specificity of the negative sample in panel 2 contributed to false-positive results throughout the EQA program. All false-positive results were received from separate participants.
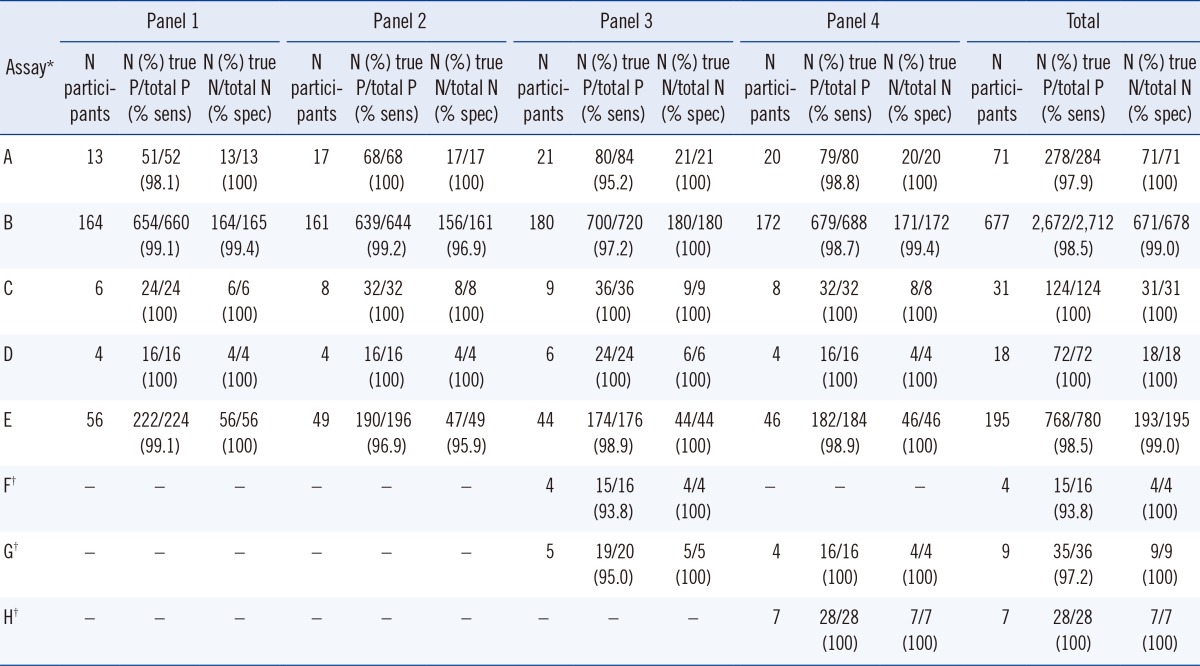
The false-negative rate was 60/4,104 (1.46%), and the false-positive rate was 9/1,026 (0.88%). As shown in Table 3, no incorrect results were reported by laboratories using kits C, D, or H, and one false-negative and no false-positive results were found using kits F and G; however, kits F, G, and H were not used widely in the EQA scheme. The number of laboratories using commercial kits A, B, C, and E were 71, 677, 31, and 195, respectively. Eight laboratories reported false-positive results, and 42 laboratories reported false-negative results. The results of commercial kits A, B, C, and E showed no differences in the detection of positive constructed C. trachomatis quality material (97.9%, 98.5%, 100%, and 98.5%, respectively; P=0.36) and negative samples (100%, 99.0%, 100%, and 99.0%, respectively; P=0.764). The results obtained with kits D, F, G, and H were not analyzed statistically because of the low frequency of use of these kits.
DISCUSSION
In the present study, mammalian epithelial cells containing specific sequences of C. trachomatis were constructed and first used successfully as control materials in an EQA program for PCR detection of C. trachomatis. Previous studies have demonstrated that detection is excellent irrespective of method at high concentrations of C. trachomatis [22, 25, 28]. The rate of correct reporting of stronger positive concentrations (≥105 copies/mL) was higher than 98.4% in the present study, which is in concordance with previous studies. The rate of false-positive results reported by nine laboratories in this study was low (0.9%), and all false-positive results were received from separate participants. This low rate has also been reported in previous reports (0.3% to 1.5% false-positive results with simulated specimens and 0-3% false-positive results with urine specimens) [20, 25].
The amount of chlamydial elementary bodies is low in clinical specimens [27]. Weakly positive samples are reportedly missed more frequently than strongly positive samples, indicating a problem with test sensitivity [20, 22]. The results of the EQA scheme in the present study also found that the number of data sets reported correctly decreased with the increase in series dilution; the lowest correct rate was 96.3% in the weakest positive samples (104 copies/mL). Table 1 shows the analytical sensitivity of the PG Biotech real-time PCR assay, demonstrating that dilution above 1:1,000 abolishes the linearity of C. trachomatis, which has a copy number on the order of 100,000/mL at this dilution. Therefore, EQA materials of 10,000 copies/mL were out of analytical range. The lack of detection may be ascribed to cell loss after centrifugation, especially in samples with low cell concentrations. Therefore, weaker positive samples in an EQA program can help detect problems in clinical operations.
Verkooyen et al. [22] have reported no differences among AMPLICOR CT/NG (Roche), COBAS AMPLICOR CT/NG (Roche), and Abbott LCxin (Abbott) in testing urine samples for C. trachomatis (P=0.48). Goessens et al. [28] also found no difference between two commercial tests [AMP-CT (Gen-Probe Inc., San Diego, CA, USA) and COBAS AMPLICOR CT/NG (Roche)] for the detection of C. trachomatis in female urine and genital swab specimens (P=0.101). Another study has indicated that differences in strain detection did not occur with the BD ProbeTec ET (BD, Franklin Lakes, NJ, USA) or Roche AMPLICORCOBAS CT/NG (P=1.0) [25]. In the present study, no significant differences were observed in the detection of positive constructed C. trachomatis control material (P=0.36) and negative samples (P=0.764) with four PCR kits.
Panel samples used in EQA have been clinical urine specimens, C. trachomatis cultured in cells, or plasmids [20, 22, 25, 26], but their use in QC procedures is problematic. The control materials described herein have several advantages over commonly used controls. First, the surrogate can be easily produced in large volumes without the restrictions imposed by sample resources. In the present example, a recombinant plasmid generated with consecutive PCR using five sets of overlapping primer pairs was transfected into epithelial cells. This construction is straightforward and avoids the need for clinical sample collection, which has generally been used for QC in previous studies [20].
Second, the surrogate is more stable. The serially diluted samples were stable at 4℃, 37℃, and room temperature for at least 1 month, and the stability results demonstrated that a range of temperature and time conditions did not influence panel performance. The material could be shipped to clinical laboratories at ambient temperature in an EQA scheme. However, in previous studies, QC materials had to be freeze-dried or shipped on dry ice [20, 22]. The process of freeze-drying can damage C. trachomatis cells by disrupting their cellular integrity, and shipping samples to testing laboratories on dry ice is cost prohibitive. Previous studies have found that plasmids consist of bare, unprotected, double-stranded DNA that may be digested by exogenous DNase [29, 30]. The recombinant plasmid in the present study was transfected into epithelial cells, thus preserving the target DNA. C. trachomatis is an obligate intracellular bacterium, and nucleic acid should be extracted in PCR assays; therefore, the construct in this study seems appropriate for nucleic acid extraction.
Third, the construct can be used widely in clinical assays because the most common cryptic plasmid sequences of C. trachomatis used in the PCR assays (see methods) were inserted, making it useful for the evaluation of various commercial kits that detect different sequence regions. Also, compared with the urine collected from individuals with overt symptomatic genital C. trachomatis infection or the strains cultured in cells that have been used in previous studies [20, 25], the surrogate panel in the PCR assay in the present study may preclude the risk of infection because it is produced solely through molecular methods, and no infectious C. trachomatis bacterium is used.
Commercial tests [e.g., Aptima CT assay, Gen-Probe TMA (Gen-Probe Inc)] [31] targeting 23S rRNA are not widely used in clinical laboratories in China. The targets for commercial kits used by the laboratories participating in the NCCL EQA for C. trachomatis detection in the present study were all cryptic plasmids. In countries where tests using rRNA as the target for C. trachomatis detection are in wide use, the rRNA target should be the focus and its design detectable. The construction of EQA material for RNA detection is different than that for DNA detection.
In conclusion, this study is the first to demonstrate a molecular method for constructing QC material with cultivated SiHa cells containing a target sequence of C. trachomatis for an EQA scheme. PCR assay with this constructed QC material was a safe and stable alternative to the use of positive clinical urine specimens, simulated specimens, or plasmids containing a single target sequence of C. trachomatis as a source of PCR positive controls. The constructed material can be widely used in the detection of C. trachomatis during EQA to compare the accuracy of detection of participant laboratories or for internal QC to monitor test reliability on a run-by-run basis. Furthermore, the sensitivity and specificity problems that occurred in the present study highlighted the need for participation in EQA schemes for the detection of C. trachomatis and demonstrated that these schemes provide valuable information to laboratories performing PCR for C. trachomatis detection in routine clinical practice in other countries.
 XML Download
XML Download