

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Coronary artery disease (CAD) is a complex and multifactorial human disease. Age, environment, lifestyle, and genetic factors are thought to contribute to the disease by exerting interactive effects, and research efforts have focused on various gene polymorphisms in relation to the prediction of disease occurrence and severity as well as drug response. Oxidation and inflammation have recently been suggested to be two important etiological mechanisms underlying atherosclerotic vascular disease [1, 2]. Increase in the expression of endogenous stress proteins such as heme oxygenase (HO) is considered a physiological response that prevents further cell damage caused by oxidative stress [3, 4].
HO is an enzyme that controls the rate of enzymatic degradation, heme to biliverdin. HO-1 is the only inducible form of HO isoenzymes and has potent anti-inflammatory, anti-oxidant, and anti-proliferative effects [5, 6]. Among the polymorphisms of the gene for HO-1 (HMOX1), the (GT)n repeat polymorphism in the promoter position is considered to have important functional implications [7, 8].
A number of studies have examined the association between cardiovascular diseases and HMOX1 polymorphisms. The risk of coronary heart disease was low in carriers of short (GT)n repeats, whereas carriers of long (GT)n repeats had an increased risk [9]. Furthermore, it was reported that patients with short (GT)n repeats had a lower risk of in-stent restenosis by decreasing inflammation [10, 11], whereas those with long (GT)n repeats had a higher risk [12].
The purpose of this study was to investigate the HMOX1 polymorphisms in the Koreans and to elucidate the association between HMOX1 polymorphisms and the occurrence of CAD as well as the risk of restenosis after coronary angioplasty or stent insertion.
Go to : 
METHODS
1. Study population
We examined 150 cardiac patients who underwent coronary angiography at a university hospital and were suspected of having heart disease because of the symptoms, such as chest pain at rest or on exertion and the electrocardiographic findings from November 2001 to October 2002.
According to the coronary angiography findings, patients with obstructive lesions of over 50% in one or more coronary arteries were classified as a group of CAD with obstructive lesions (n=110), and those who had been found to be normal or to have less than 50% stenosis were classified as the CAD with minimal or no lesions group (n=40). Patients in the group of CAD with obstructive lesions were further divided into three groups depending on the number of vessels with obstructive lesions: 1 vessel disease (VD) (n=48), 2VD (n=36), and 3VD (n=26).
Patients with obstructive lesions also underwent coronary angioplasty and stent insertion and received follow-up coronary angiography after six months in order to verify the presence of restenosis. Thirty-nine patients completed the follow-ups. Healthy adults who visited the health examination center were randomly included in the control group (n=107).
Exclusion criteria were as follows: 1) subjects who had any abnormal results in the complete blood count, chemistry tests (including liver enzymes), total protein and albumin, total and direct bilirubin, blood urea nitrogen (BUN) and creatinine, thyroid hormones, and various tumor markers; 2) history of hypertension or diabetes; and 3) family history of cardiovascular disease. We gathered information regarding whether the subject had hypertension or diabetes, their smoking status, and family history of cardiovascular disease from their medical records.
Hypertension was defined when blood pressure exceeded 140/90 mmHg in repeated measurements or anti-hypertensive agents were administered. Diabetes was defined when fasting plasma glucose exceeded 126 mg/dL or anti-diabetic agents were administered. Hyperlipidemia was defined as fasting cholesterol level exceeding 200 mg/dL or LDL cholesterol (LDL-C) exceeding 130 mg/dL. The entire study population was classified according to the risk factors for CAD: hypertension (n=70), diabetes (n=47), and hyperlipidemia (n=57). Restenosis was defined as 50% or greater coronary lumen stenosis that was confirmed in the 6-month follow-up coronary angiography.
Informed consent was obtained from all the subjects. This study was approved by the hospital's institutional review board.
2. Specimens
Venipunctures were performed after 12-hr overnight fasting before coronary angiography or regular health check-up. The venous blood was collected in a serum-separating vacutainer and in an EDTA-containing vacutainer. The sera were stored in a deep freezer at -70℃ until analysis, and DNA was extracted from whole blood by using Wizard Genomic DNA Purification kit (Promega, Madison, WI, USA) and stored in a deep freezer in -70℃ until genotyping.
3. Biochemical parameters
The sera were used to analyze the levels of cholesterol, triglyceride, HDL cholesterol (HDL-C), bilirubin (Wako, Osaka, Japan), LDL-C, and high sensitivity C-reactive protein (hsCRP) (Denka Seiken, Tokyo, Japan) with a chemistry autoanalyzer (Hitachi 7600; Hitachi Chemical Co., Tokyo, Japan). The hsCRP had a lower detection limit of 0.1 mg/L and reference intervals of equal to or less than 3.0 mg/L.
4. HMOX1 promoter polymorphism analysis
HMOX1 polymorphism was analyzed by the number of (GT)n repeats in the promoter region by PCR with Gene Amp PCR system 9600 (Applied Biosystems, Foster City, CA, USA). The HMOX1 promoter polymorphisms were classified as (GT)n repeats less than 25 were termed "S25 (S for short)" alleles and those with 25 repeats or more were termed "L25 (L for long)" alleles, yielding S25/S25, S25/L25, and L25/L25 genotypes, and the carriers of S25 alleles comprised homozygous and heterozygous S groups. The following pair of primers was used: sense, 5'-AGAGCCTGCAGCTTCTCAGA-3' and anti-sense, 5'-ACAAAGTCTGGCCATAGGAC-3'. The PCR products were analyzed using ABI 3130 (Applied Biosystems), and their sizes were determined with GeneScan software (Applied Biosystems).
5. Statistical analysis
All biochemical indicators except triglycerides and hsCRP were expressed as mean±standard deviation. Triglyceride and hsCRP values were expressed as median and interquartile range. In addition, the positive rates of hsCRP were compared, and 1.0 mg/L or more was considered positive according to the recommendations for clinical and public health practice, in which the patients with less than 1 mg/L of hsCRP were categorized as low risk for cardiovascular disease [13].
Total cholesterol, LDL-C, and HDL-C were compared by using an ANOVA with Bonferroni post-hoc tests; however, triglyceride and hsCRP were compared by non-parametric Mann-Whitney test. Sex, hypertension, diabetes, smoking, frequency of positive hsCRP, and genotype and allele frequencies were compared by Chi-square test. The associations between CAD and risk factors were analyzed using multivariate logistic regression. Multivariate logistic regression analysis was applied to assess the association of HMOX1 genotype, group classification, and to adjust for potentially confounding variables. We compared all CAD patients to the control group. In the first step, we performed univariate analysis using Chi-square test. Next, for variables that showed suggestive evidence of association (P<0.2), multivariate logistic regression were performed with adjustments for covariates. P values of <0.05 were considered statistically significant. SPSS software (ver. 18, SPSS Inc., Chicago, IL, USA) was used for statistical analyses.
The Hardy-Weinberg equilibrium test was performed on genotype and allele frequencies, and the sample size adequacy of this study was tested with a power analysis (Epi Info software, Centers for Disease Control and Prevention, Atlanta, GA, USA).
Go to :
RESULTS
1. Clinical and biochemical characteristics of study populations
The average age of patients in both groups was significantly higher than that of the controls (63±11 and 60±10 yr vs. 52±12 yr; P<0.001). There were no intergroup gender differences. Moreover, while there were no differences between the CAD with obstructive lesions and CAD with minimal or no lesions groups with respect to the frequencies of hypertension, diabetes and smoking history; however, there were higher frequencies than the control group (hypertension, diabetes; P<0.001, smoking; P=0.012). Among the biochemical parameters, total cholesterol, LDL-C, and hsCRP levels were significantly higher in both CAD groups than in the control group, and total bilirubin level was higher in CAD with obstructive lesions than in the control group (Table 1).
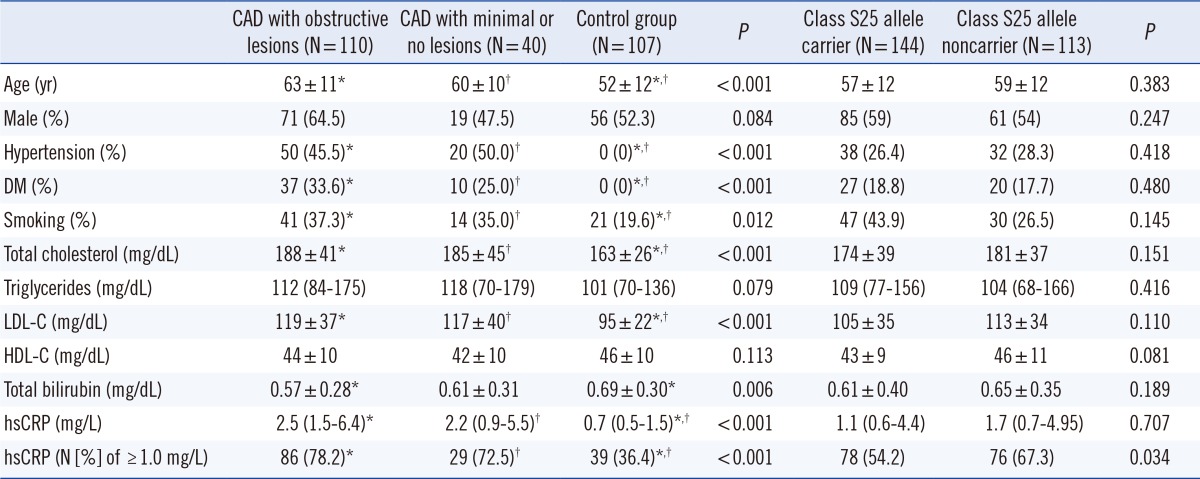
Table 1
Demographic and biochemical data and comparisons of all study populations according to HMOX1
Data are given as counts and percentages, mean and standard deviation, or median and interquartile range. P<0.05 is considered statistically significant. The class S25 allele carrier involves the genotypes of S25/S25 and S25/L25; class S25 allele noncarrier, genotype L25/L25.
*,†The P value was calculated between the groups marked with the same superscript.
Abbreviations: CAD, coronary artery disease; DM, diabetes mellitus; LDL-C, LDL cholesterol; HDL-C, HDL cholesterol; hsCRP, high sensitivity C-reactive protein.
![]()
Regarding the subgroups of the number of coronary arteries with lesions, the intergroup comparisons revealed no significant differences in all parameters except for age, whereby the average age of the 3VD group was significantly higher than that of the 1VD and 2VD groups (69±10 vs. 61±10 and 62±12 yr, respectively; P<0.007).
2. HMOX1 promoter polymorphism
Analysis of the HMOX1 gene promoter polymorphism revealed that the number of (GT)n repeats ranged from 16 to 41, showing a bimodal distribution, in which the highest frequencies were shown at 23 and 30 repeats (Fig. 1).
 | Fig. 1The frequency distributions of the numbers of (GT)n repeats of the HMOX1 promoter. (A) Total study populations (N=257), (B) CAD with obstructive lesions group (N=110), (C) MD (N=40), and (D) controls (N=107).
Abbreviations: CAD, coronary artery disease, CAOD, coronary artery disease with obstructive lesions; MD, coronary artery disease with minimal or no lesions.
|
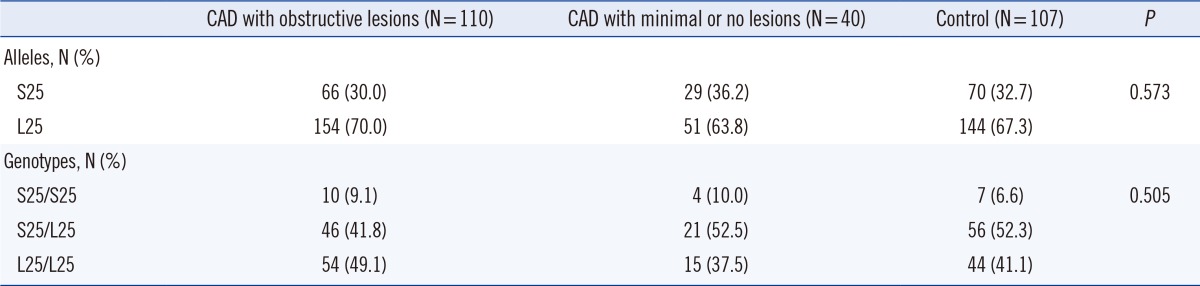
There were no significant differences in allele and genotype frequencies between patient and control groups (Table 2).
Furthermore, we divided the entire study population into two groups: an S25-carrier group with the alleles of less than 25 (GT)n repeats and a non-S25 carrier group that lacked the S25 allele. We then performed comparative analyses with respect to all parameters. The S25-carrier group included S25/L25 and S25/S25 genotypes, and the non-S25 group included only the L25/L25 genotype. Among age, sex, hypertension, diabetes, and biochemical parameters, only the positive rate of hsCRP was significantly higher in the non-S25 carrier group than in the S25 carrier group (P=0.034) (Table 1).
3. Restenosis following coronary stenting at the 6-month follow-up
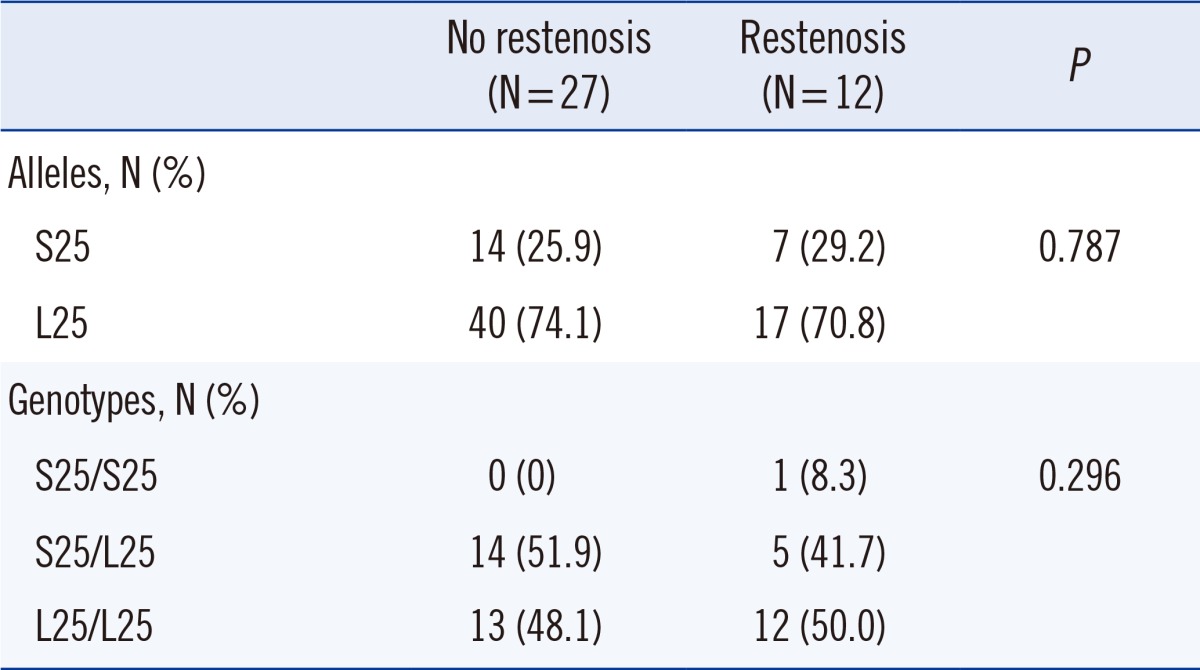
In the CAD group with obstructive lesions, 39 patients completed 6-month follow-ups and subsequent coronary angiographies. Four patients underwent percutaneous transluminal coronary angioplasty, 34 patients had coronary angioplasty with a stent insertion, and 1 patient underwent coronary artery bypass graft. Among these 39 patients, 12 had vascular restenosis, whereas 27 were restenosis-free. Comparative analyses revealed no significant intergroup differences in any of the clinical and biochemical parameters as well as allele and genotype frequencies (Table 3).
4. Multivariate logistic analysis of HMOX1 polymorphisms and other coronary risk factors
Analysis of the genotypes and CAD for each risk factor group did not yield any significant differences.
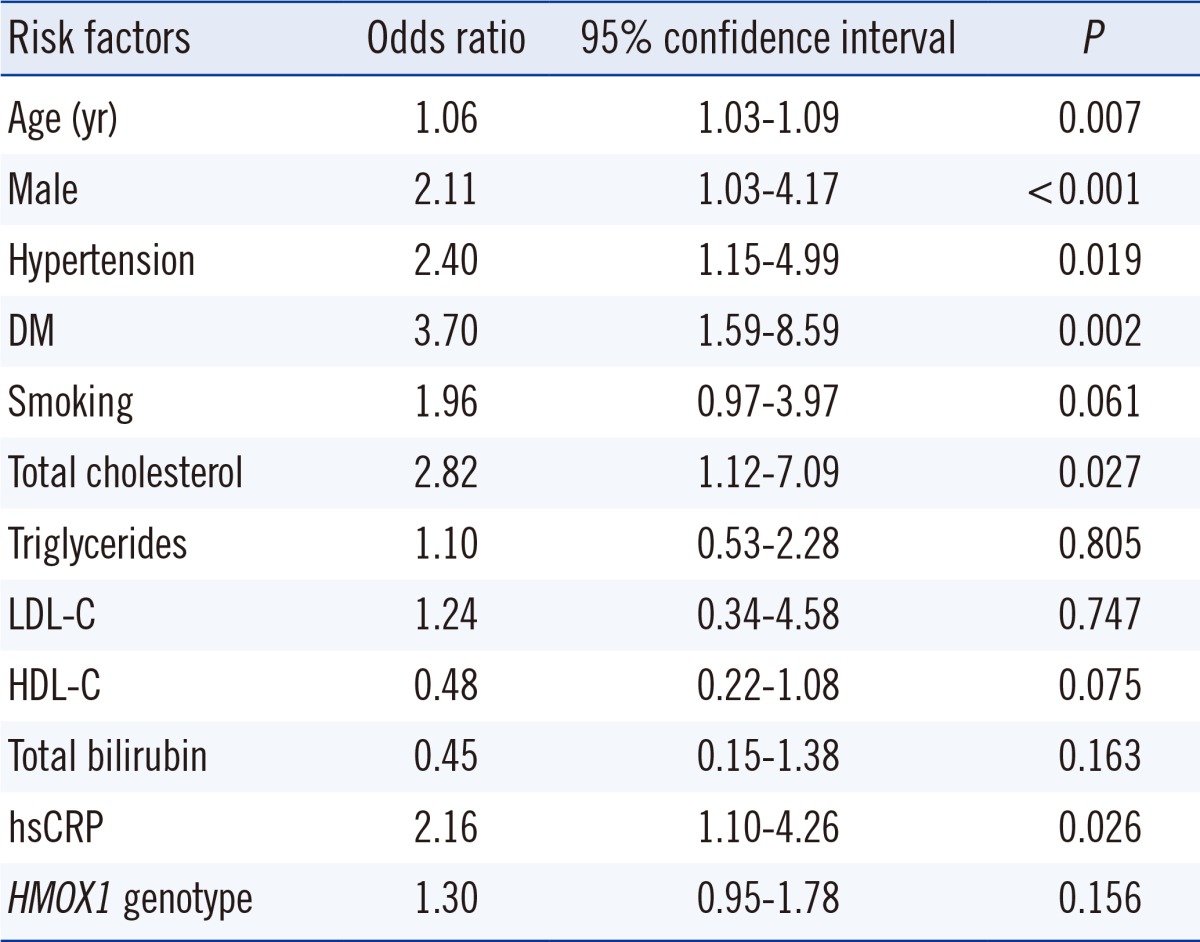
Multivariate regression analysis revealed a significantly high odds ratio for sex, age, hypertension, diabetes, cholesterol, and hsCRP, whereas HMOX1 genotype and bilirubin levels did not yield a significant odds ratio (Table 4). Most traditional cardiovascular risk factors were significantly associated with CAD; however, there was no significant association between HMOX1 genotype and CAD in these patients.
Go to :
DISCUSSION
Inflammatory responses play a crucial role in various atherosclerosis-related diseases such as CAD. The fact that atherosclerosis, which is the key cause of CAD, is an inflammatory disease indicates that its relevant immune mechanism interacts with metabolic risk factors, thereby developing and activating arterial lesions [14]. Recently, oxidative stress has also been considered a pathogenic mechanism of a variety of diseases, such as atherosclerosis, myocardial ischemia, and neurodegenerative diseases [8, 15]. Increase in the expression of endogenous stress proteins such as HO can be a physiological response to prevent further cell damage by oxidative stress [1, 2].
The heme-HO system is a regulator of the integrity of endothelial cells and oxidative stress [3]. The anti-oxidant activity of HO-1 generates biliverdin and bilirubin by degrading heme during the process of releasing carbon monoxide. Carbon monoxide plays an important role in controlling the vascular tone [16]. Induction of HO-1 activity has a protective effect for atherosclerosis, sepsis, diabetes, lung injury, vascular obstructive disease, and ischemic heart [6, 17]. Because bilirubin reduces oxidative stress, high bilirubin levels are related to a lower risk of LDL oxidation and hinders CAD [18, 19]. The increase in HMOX1 transcription mediated by statins is related to the increase in HO-1 proteins and decrease in free radicals [20].
The capacity to induce HO-1 differs from individual to individual, and there are 3 polymorphisms at the HMOX1 promoter, which regulates the quantitative activities of HO-1. Among them, (GT)n repeat polymorphism and the single nucleotide polymorphism (SNP) at the -413 position are believed to have functional importance [8]. The (GT)n repeat polymorphism is a purine-pyrimidine sequence with a Z-conformation structure and is known to have negative effects on transcription activity [9].
With respect to the distribution of (GT)n repeats, several studies found bimodal distributions with 23 and 30 repeats as the (GT)n alleles, which is consistent with the findings observed in our study. From this, we inferred that this distribution pattern is common to humans, regardless of racial differences. The previous studies divided the alleles with this bimodal distribution pattern into either two groups of short- and long-allele groups or three groups by adding a medium-allele group. When classifying these groups, they used the reference sequences to be 22, 23, and 25 for the short alleles and 27, 29, and 30 for the long alleles [10, 11, 12, 21, 22, 23, 24]. For the analyses in the present study, we classified the alleles into S and L groups, setting 25 repeats as a cut-point; 29 repeats were also used as a cut-point, but did not find any differences in genotypic and allelic frequencies between the patient and control groups (data not shown).
There are a number of studies regarding the association between HMOX1 polymorphisms and various diseases, such as chronic pulmonary emphysema [23], lung disease [6, 25], cancer [24], hyperbilirubinemia [18, 26], renal disease [27], and stroke [16, 28, 29]. The consensus from these studies is that the ability of upregulation of HO-1 exerts an important protective role against specific diseases.
Research on the HMOX1 polymorphism is especially focused on CAD. These are based on the findings of studies that showed that HO-1 expression played a crucial role in the formation of atherosclerotic lesions in the aorta of LDL receptor knockout mice [5]. A previous study stated that short (GT)n repeats were associated with a reduced risk of CAD under high oxidative stress [15]. In a study on Chinese people with type 2 diabetes, the patients with long (GT)n repeats had a 4.7-fold higher risk for CAD [12]. A similar study conducted in Japanese people revealed that, among the high-risk groups of people with hyperlipidemia or diabetes as well as smokers, the carriers of short (GT)n repeats had a reduced risk for CAD [9]. On the other hand, in another study, similar distributions of polymorphic (GT)n repeats were found in patients with myocardial infarction and stable angina versus controls, and that only the group with short repeat sequences showed significantly high concentrations of bilirubin and high-density lipoprotein [30].
In the present study, there were no significant differences in genotype and allele frequencies between the CAD patients and control groups, but the non-S carrier group showed a significantly higher hsCRP positive rate than the S-carrier group. This result is similar to the one by Li et al. [31] that revealed the baseline CRP of the patients with CADs differed by genotype by showing that those carrying the long allele had higher CRP than those who did not have a long allele. These results seem to be consistent with other reports that carriers of the short allele showed fewer incidences of inflammation and thus they had a lower risk of restenosis [7, 11, 32].
The restenosis rate in this study was about 30%, which is similar to previous reports. Many of the factors inhibited by HO-1 are involved in restenosis occurrence by suppressing inflammation of the vascular wall, vascular spasm and remodeling, and formation of neointimal thickening through smooth muscle cell proliferation. With regard to HMOX1 promoter genotype, short (GT)n repeats are thought to decrease the risk for restenosis after coronary angioplasty by reducing inflammatory responses compared with long repeats [11]. These results were verified in two prospective studies, in which the risk for restenosis in patients with short (<25) GT repeats who underwent percutaneous angioplasty on peripheral arteries was reduced to 0.24 and 0.43, respectively [7, 11].
The long allele has been reported to be a risk factor for the occurrence of restenosis in several studies [22, 31]. As such, these findings are similar to other studies conducted on people of different ethnic backgrounds, and therefore provide strong evidence that the mechanism of vascular restenosis is associated with the HMOX1 (GT)n repeat polymorphism. This can also be explained by its implications for predicting significant adverse effects or outcomes [12]. In our study, however, no significant differences in the allelic and genotypic frequencies were exhibited by the restenosis and restenosis-free groups after coronary angioplasty or stent placement. This discrepancy between our results and those of previous studies is presumably attributable to the small sample size of the patients in our study (n=39) who completed the follow-up coronary angiography to determine the risk factors for restenosis.
The clinical conditions which showed associations with the HMOX1 genotype are very different across studies, thus leaving room for debate regarding how they are related with known risk factors in various clinical settings. In the present study, the comparisons of disease frequencies according to genotype distribution in the presence of various risk factors did not yield any significant differences.
The limitations of this study are that there was a small sample size and the gene-gene interaction and association with other genetic polymorphisms could not be taken into account because only a specific gene was studied.
In conclusion, a microsatellite polymorphism in the HMOX1 gene promoter was observed in the Korean population with a bimodal distribution, which is similar to that of previous studies. The HMOX1 genotypes were not associated with CAD in the Korean population, but the short allele carrier group contained more individuals with hsCRP values that place them at low risk for cardiovascular disease.
Go to :
 XML Download
XML Download