

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
ABO antibodies can cause hemolytic transfusion reactions, hemolytic disease of the fetus and newborn (HDFN), and chronic rejection of solid organ transplants. In ABO-incompatible marrow transplants, ABO antibodies can cause hemolysis, delaying the engrafting of red blood cells (RBC) and megakaryocytes [1].
ABO antibody titration has been used to determine treatment strategies and evaluate patient outcomes in ABO-incompatible marrow transplant and solid organ transplantation and to evaluate ABO-incompatible transfusion responses [2, 3, 4, 5]. Most immune reactions related to transfusion and organ transplant are caused by IgM ABO antibodies, but IgG also plays an important role in these immune reactions. In ABO-incompatible kidney transplantation, particularly, IgG antibodies are believed to be responsible for poor graft outcomes [6]. Therefore, when performing an ABO antibody titration, a method that accurately measures all antibodies including IgG is needed.
Antibody titration can be performed using the conventional tube method, the column agglutination technique (CAT), enzyme immunoassay, flow cytometry, and a variety of other methods. Most laboratories use a conventional tube method primarily because it is cost-effective, but this technique is limited by difficulties in automation and standardization [6, 7, 8]. CAT is less prone to technical variation, and the stability of the final reaction phase allows reproducible results to be obtained by multiple individuals [9, 10].
Cho et al. [11] compared the effectiveness of microcolumn agglutination and tube methods for ABO antibody titration. They suggested that microcolumn agglutination with anti-human globulin (AHG) method could be used to standardize ABO antibody titration at different institutions. They measured only total ABO antibody, however, and did not distinguish between IgM and IgG antibodies. On the other hand, Kang et al. [7] investigated ABO antibody titer distribution of normal individuals using the AHG tube method with and without dithiothreitol (DTT) to distinguish IgM and IgG antibodies. However, they performed tests with only conventional tube methods.
In this study, we investigated the utility of CAT with and without DTT for determining total and IgG ABO antibody titers in healthy individuals in comparison to conventional tube methods. The results will also provide baseline data for ABO-incompatible organ transplantation in Korea.
Go to : 
METHODS
1. Study population
Among healthy adults between ages of 20 and 60 that underwent medical examination at our hospital from June to August 2012, 60 individuals with blood group A (30 men, 30 women), 60 with blood group B (29 men, 31 women), and 60 with blood group O (31 men, 29 women) were selected for the study, and their sera were used for antibody titration. The age distribution was 19 (10.6%), 20-29 yr; 44 (24.4%), 30-39 yr; 67 (37.2%), 40-49 yr; and 50 (27.8%), 50-59 yr. RBC were obtained from four healthy volunteers (two group A and two group B individuals) and treated with citrate phosphate dextrose-adenine 1 (CPDA-1). Approval for all study parameters was obtained from the Soonchunhyang University Hospital's institutional review board (2013-071).
2. ABO antibody titration
1) Immediate spin (IS) tube method
The IS tube method was performed as outlined in the American Association of Blood Banks (AABB) Technical Manual [12]. Briefly, 10 tubes were labeled for the appropriate dilutions, and serial dilutions of 100 µL serum in saline were prepared. To each dilution was added 3% saline-suspended group A or group B RBCs. After incubation at ambient (22-25℃) room temperature and centrifugation at 1,000 g for 25 seconds, test results were determined macroscopically by two medical technicians and two laboratory physicians. The titer endpoint was the reciprocal of the highest dilution yielding weak agglutination.
2) AHG tube method
After completing the IS tube test, the tubes were incubated at 37℃ for 30 min and washed three times using normal saline. After adding 100 µL of polyspecific AHG (Millipore, Livingston, UK), the tubes were centrifuged at 1,000 g for 15 sec. Test results were interpreted in the same manner as the IS tube method.
3) Column agglutination technique without DTT (CAT without DTT) treatment
CAT without DTT was performed as described in the AABB [12]. Ten tubes were labeled for the appropriate dilutions and serial dilutions of 100 µL serum were prepared in phosphate-buffered saline (PBS) at pH 7.3 and incubated at 37℃ for 45 min. Then, 50 µL of 0.8% group A or B RBC suspension solution and 25 µL of diluted serum were added to the LISS/Coombs card (DiaMed AG, Cressier sur Morat, Switzerland). RBCs used for CAT were the same as those used for the tube methods. After incubating for 15 min at 37℃, the card was centrifuged for 10 min at 85 g, and the agglutination reactions were examined macroscopically by two medical technicians and two laboratory physicians. The titer endpoint was the reciprocal of the highest dilution yielding weak agglutination. A weak positive reaction is characterized by only a few RBC agglutinates remaining in the gel area just above the RBC pellet at the bottom of the microtube.
4) Column agglutination technique with DTT (CAT with DTT) treatment
CAT with DTT was performed as described in the AABB [12]. Briefly, 0.01 M DTT was prepared by dissolving 0.154 g of DTT in 100 mL of pH 7.3 PBS. Ten tubes were labeled for the appropriate dilutions, and serial dilutions of 100 µL serum were prepared in 0.01 M DTT (Sigma-Aldrich, St. Louis, MO, USA). The remainder of the test was performed in the same manner as CAT without DTT.
3. Statistics
The Kruskal-Wallis and Mann-Whitney tests were used to evaluate the distribution of antibody titers according to age and gender. The Wilcoxon signed rank test was used to compare antibody titers among the IS tube, AHG tube, CAT without DTT, and CAT with DTT methods. SPSS Version 18.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analyses, and P values less than 0.05 were considered statistically significant.
Go to :
RESULTS
1. Distribution of antibody titers according to age and gender
The distribution of ABO antibody titers according to age group is shown in Table 1. There were no statistical differences among age groups (Table 1). The titers measured by the IS tube method were higher in females than in males (P=0.005), but titers by other methods showed no statistical differences between genders (Table 2).

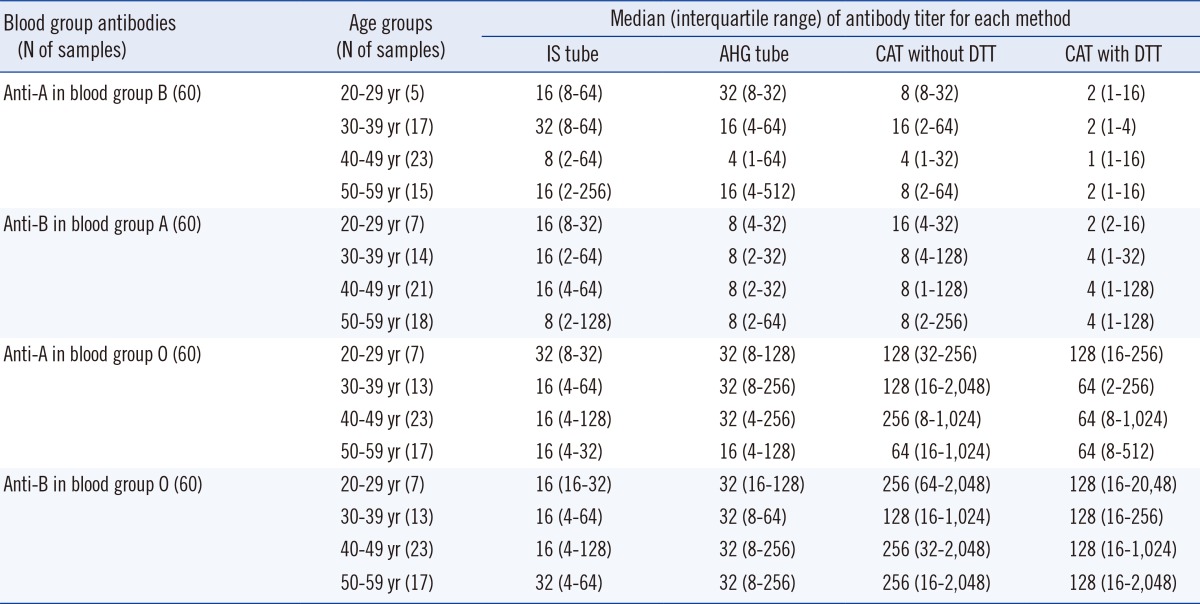
Table 2
Distribution of ABO antibody titers according to gender
*The titers measured by the IS tube method were higher in females than in males (P=0.005, Mann-Whitney test), but titers by other methods showed no statistical differences between genders.
Abbreviations: IS, immediate spin; AHG, anti-human globulin; CAT, column agglutination technique; DTT, dithiothreitol.
![]()
2. Comparison of antibody titers between the IS tube and AHG tube methods
The median (interquartile range) values of anti-B titers in blood group A obtained using IS and AHG tube methods were 16 (2-256) and 8 (1-512), respectively, and those of anti-A titers in blood group B obtained using IS and AHG tube methods were 16 (2-128) and 8 (2-64), respectively; both values were higher in IS than in AHG tube methods (anti-B, P=0.003; anti-A, P<0.001). Median (interquartile range) values of anti-B titers in blood group O obtained using IS and AHG tubes were 16 (4-128) and 32 (4-256), and those of anti-A titers in blood group O were 16 (4-128) and 32 (8-256), respectively. In these cases, titer values were higher in AHG than in IS tube methods (anti-B, P<0.001; anti-A, P<0.001) (Table 3, Fig. 1).
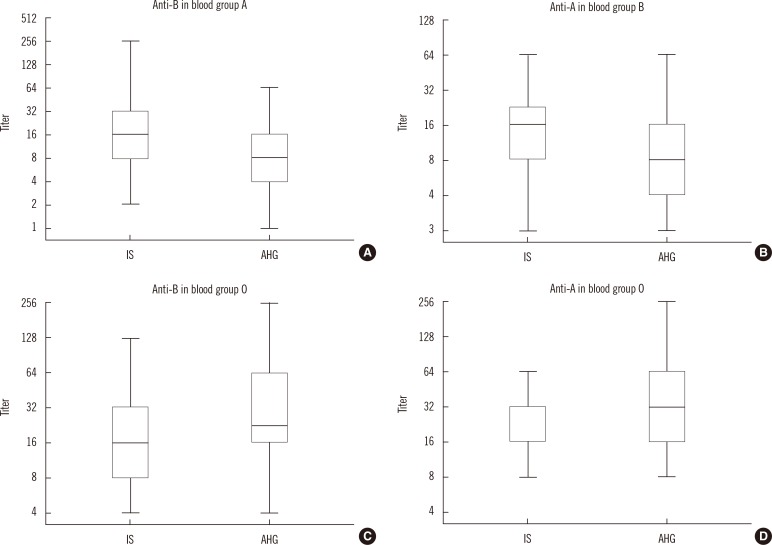 | Fig. 1Comparison of antibody titers obtained using the IS tube and AHG tube methods. The horizontal lines in the middle of each box, the top and bottom borders of each box, and whiskers above and the below the boxes represent median values, interquartile ranges, and error bars, respectively. (A) anti-B in blood group A. (B) anti-A in blood group B. (C) anti-B in blood group O. (D) anti-A in blood group O individuals.
Abbreviations: IS, immediate spin; AHG, anti-human globulin.
|

3. Comparison of antibody titers between AHG tube and CAT without DTT methods
The median (interquartile range) values of anti-B titers in blood group A obtained using AHG tube and CAT without DTT methods were 8 (1-512) and 8 (1-64), respectively, and those of anti-A titers in blood group B were 8 (2-64) and 8 (1-256), respectively. There was no statistical difference between the two methods. The median (interquartile range) values of anti-B titers in blood group O obtained using AHG tube and CAT without DTT methods were 32 (4-256) and 128 (8-2,048), and those of anti-A titers in blood group O were 32 (8-256) and 256 (16-2,048), respectively. Titers were higher in CAT without DTT than in AHG tube methods (anti-B, P<0.001; anti-A, P<0.001) (Table 3, Fig. 2).
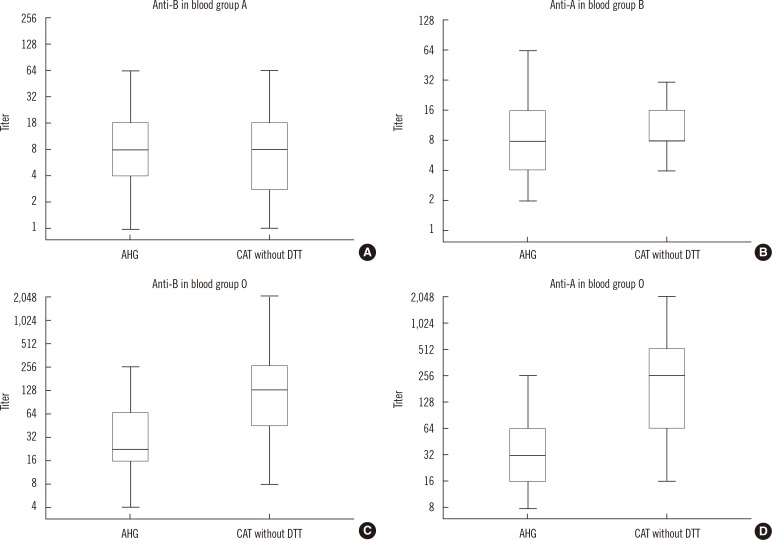 | Fig. 2Comparison of antibody titers obtained using the AHG tube and CAT without DTT methods. The horizontal lines in the middle of each box, the top and bottom borders of each box, and whiskers above and the below the boxes represent median values, interquartile ranges, and error bars, respectively. (A) anti-B in group A. (B) anti-A in group B. (C) anti-B in group O. (D) anti-A in group O individuals.
Abbreviations: AHG, anti-human globulin; CAT, column agglutination technique; DTT, dithiothreitol.
|
4. Comparison of antibody titers obtained using CAT with and without DTT methods
The median (interquartile range) values of anti-B titers in blood group A obtained using CAT without and CAT with DTT methods were 8 (1-64) and 2 (1-16), respectively, and those of anti-A titers in blood group B were 8 (1-256) and 4 (1-128), respectively; titer values were higher in CAT without DTT than in CAT with DTT methods (anti-B, P<0.001; anti-A, P<0.001). Median (interquartile range) values of anti-B titers in blood group O obtained using CAT without and with DTT were 256 (16-2,048) and 128 (16-2,048), and those of anti-A titers in blood group O were 128 (8-2,048) and 64 (2-1,024), respectively; titers were higher in CAT without DTT than in CAT with DTT methods (anti-B, P<0.001; anti-A, P<0.001) (Table 3, Fig. 3).
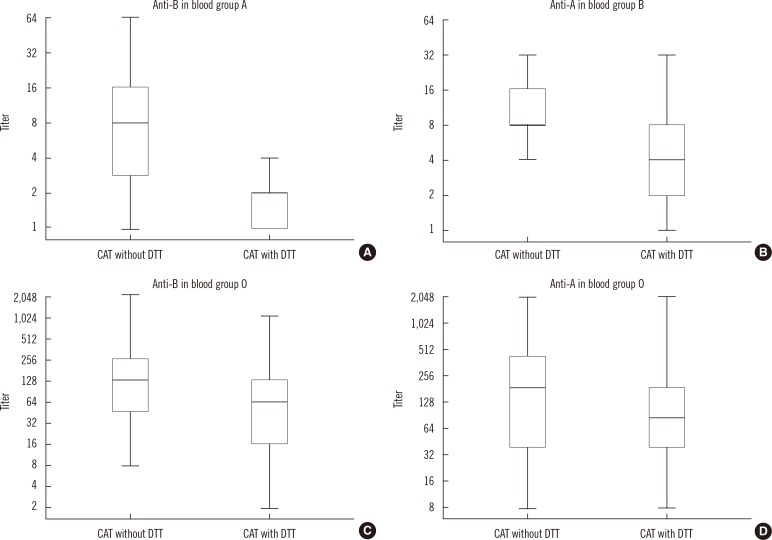 | Fig. 3Comparison of antibody titers obtained using CAT with and without DTT methods. The horizontal lines in the middle of each box, the top and bottom borders of each box, and whiskers above and the below the boxes represent median values, interquartile ranges, and error bars, respectively. (A) anti-B in group A. (B) anti-A in group B. (C) anti-B in group O. (D) anti-A in group O individuals.
Abbreviations: CAT, column agglutination technique; DTT, dithiothreitol.
|
Go to :
DISCUSSION
Titration of ABO antibodies is usually performed with serial two-fold dilutions of serum with selected red cells. Titration values can provide information on the relative amount of antibodies present in serum, and this information is especially important in cases of ABO HDFN and ABO-incompatible bone marrow and solid organ transplantations [12, 13]. However, no standard method for ABO antibody titration has been established in Korea. According to Lee et al. [13], who performed inter-laboratory proficiency tests of different ABO antibody titration methods in four university hospitals in Korea, inter-institutional maximum differences of IgM and IgG ABO antibody titers were up to 16-fold and 32-fold, respectively. On the basis of these results, knowing the differences between titer distributions exhibited by each method and each institution could be very important.
In this study, we performed ABO antibody titrations by IS tube, AHG tube, and CAT with and without DTT methods. The median values of ABO antibodies by IS and AHG tubes in our study were similar with those of Kang et al. [7], but our interquartile ranges were wider than theirs, while our median values of ABO antibodies were lower than those of Cho et al. [11]. Given the fact that our study enrolled 180 individuals (60 A, 60 B, and 60 O subjects), it was thought that our data would be more reliable than the other two studies, in which about 60 individuals were enrolled. We measured the titers of IgG ABO antibodies by CAT with DTT and compared them with those of Kang et al. [7], in which IgG titers were measured by the tube method. IgG titers of anti-A and anti-B in group B and group A individuals, respectively, were similar between the two studies, but the median values of IgG anti-A and anti-B titers in group O individuals were higher in our study (2 titers higher in anti-A and 3 titers higher in anti-B). Therefore, CAT with DTT was considered more sensitive than the tube with DTT method, especially in group O individuals. The higher sensitivity might be because IgG is the major isotype for anti-A and anti-B in group O serum, while IgM is the predominant isotype found in group A and group B individuals, and because the activity of IgG is enhanced by AHG, especially in the column agglutination method that includes both LISS and AHG (LISS/Coombs card) [12].
Monitoring ABO antibody titers is critical in several clinical situations, particularly in potential recipients of ABO-incompatible kidney transplantation, in order to determine the effectiveness of pretreatment regimens and the point at which antibody levels have been sufficiently reduced to permit successful engraftment [14, 15]. Methods with improved sensitivity and objectivity would be useful in such patients.
ABO antibody titer has typically been determined by conventional tube methods, but subjective rather than objective interpretation likely causes inter-examiner variation and, consequently, inter-institutional variation [8]. However, the high cost of the CAT method could be a burden that interferes with its adoption. For example, the cost per ABO antibody titration test, including DTT treatment for IgG titration, is about 8,000 Korean won (8 US dollars) by using the conventional tube method and about 18,000 Korean won (18 US dollars) with CAT. Korea has a compulsory nationalized healthcare system that covers the whole population, and the medical cost covered by the National Health Insurance System for blood group antibody titration is only 6,000 Korean won (6 US dollars), which was calculated only by considering the cost of running the conventional tube method without DTT treatment (3,785 Korean won). As mentioned above, IgG antibody is considered to be important for predicting poor graft outcomes in ABO-incompatible kidney transplantation [6]. Moreover, the CAT method for testing IgG anti-A and anti-B antibodies in group O individuals showed higher sensitivity than the conventional tube method. Even without consideration of labor costs, performing ABO antibody titration with DTT treatment would exceed the medical fee covered by insurance.
In conclusion, the present data show that CAT with and without DTT treatment should be performed for titration of anti-A and anti-B, especially in group O patients undergoing organ transplantation, to provide more sensitive results. However, because of the cost of reagents and personnel, it will be necessary to adjust the insurance coverage for blood group antibody titration in these cases.
Go to :
 XML Download
XML Download