

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acute leukemia is a heterogeneous disorder, and chromosomal aberrations are found in leukemic cells. Cytogenetic aberrations are found in 60% and 65-90% of AML and ALL cases, respectively [1]. The World Health Organization classification categorizes patients with cytogenetic or molecular evidence of genetic abnormalities into specific disease subsets. The concept of classifying acute leukemia according to genetic abnormalities has been accepted by most leukemia investigators. This classification is based on the detection of chromosomal aberrations to predict response to induction therapy, relapse risk, and overall survival [1, 2, 3, 4, 5].
Conventional G-banding analysis (G-banding) is the most commonly used method to detect cytogenetic abnormalities. However, detection of clonal chromosomal abnormalities by G-banding is often unsuccessful; subtle or submicroscopic (i.e., cryptic) rearrangements affecting regions smaller than a chromosomal band cannot be detected by G-banding. FISH may be used to supplement G-banding, but FISH is restricted to the defined chromosome regions of the probes used. Multiprobe FISH panels are designed to detect up to eight different FISH probes on a single slide. Multiple FISH probes can be hybridized on the same slide in a spatially separated manner, allowing rapid analysis of cytogenetic aberrations in a single hybridization experiment. Thus, multiprobe FISH assay can be used effectively in acute leukemia, but few studies were reported compared to other hematologic disease [7]. We evaluated the multiprobe FISH assay in acute leukemia in comparison with the G-banding analysis. To the best of our knowledge, this is the first comparative study of G-banding and multiprobe FISH for diagnosis of ALL and first study of utilization of multiprobe FISH assay for diagnosis of acute leukemia in Korea.
METHODS
1. Patients and samples
Thirty acute leukemia patients were enrolled in the study, including 15 AML and 15 ALL, with median ages of 54 yr (range, 35-72 yr) and 32 yr (range, 4-60 yr), respectively. All patients attended the hematology clinic at Dong-A University Hospital, from October 2008 to October 2012. Bone marrow aspirates were collected at diagnosis before any treatment. The diagnosis of leukemia was established according to the WHO classification and the French-American-British (FAB) classification [5, 6]. In most cases, the slides were prepared with the cells collected at presentation, and in some cases, new slides were prepared from cells that were kept frozen in liquid nitrogen. The study was approved by the Institutional Review Board of Dong-A University Hospital. All patients gave signed informed consent to use a part of the samples for scientific purposes.
3. Multiprobe FISH
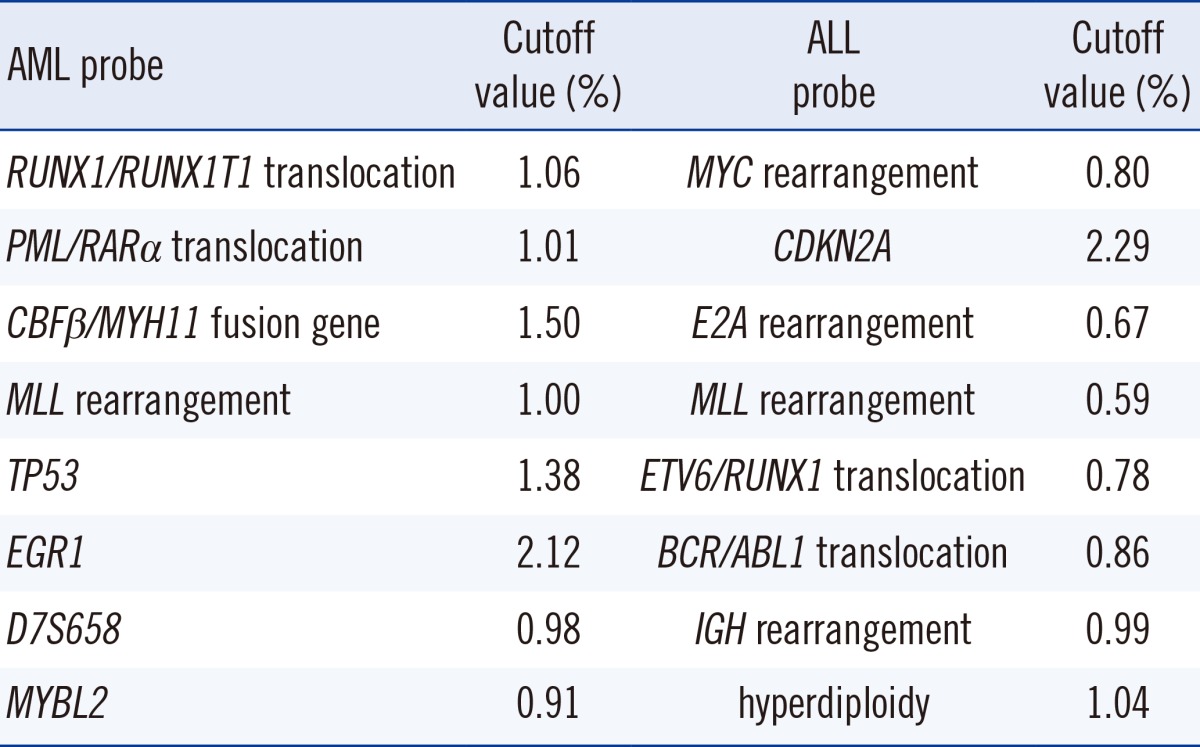
The multiprobe AML panel was designed to detect eight different FISH probes: RUNX1/RUNX1T1 translocation, PML/RARα translocation, CBFβ/MYH11 fusion gene, MLL rearrangement, TP53, EGR1, D7S658, and MYBL2 probes. The multiprobe ALL panel included eight different FISH probes: MYC rearrangement, CDKN2A, E2A rearrangement, MLL rearrangement, ETV6/RUNX1 translocation, BCR/ABL1 translocation, IGH rearrangement, and hyperdiploidy probes consisting of CHIC2, D10Z1, and D17Z1. Multiprobe FISH was performed according to the manufacturer's instructions (Cytocell, Cambridge, UK). FISH probes are reversibly bound to the surface of a glass device, and upon contact with hybridization buffer, they dissolve in the solution; denaturation of the probes and target DNA occurs simultaneously upon heating. Probes were validated according to the American College of Medical Genetics (ACMG), and cutoff values were established by testing five normal peripheral blood samples [8]. To establish a normative database for the probes, data were gathered from at least 500 interphase cells from each individual in the control group. The normal cutoff for the analysis of 500 interphase cells was calculated for FISH results by using a binominal distribution assessment [8, 11, 12]. The cutoff values established by validation procedures are shown in Table 1. By definition, abnormality was diagnosed only when the percentage of cells with aberrant FISH signals was greater than the cutoff value. At least 300 nuclei were evaluated for each probe.
RESULTS
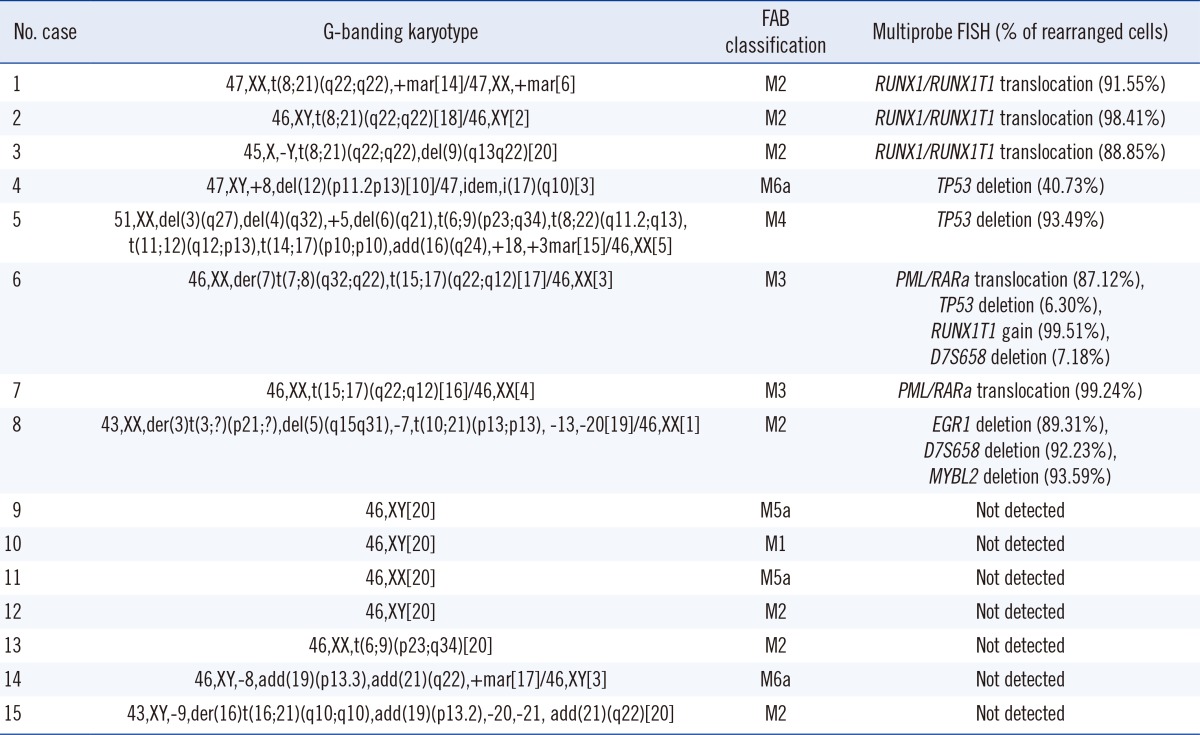
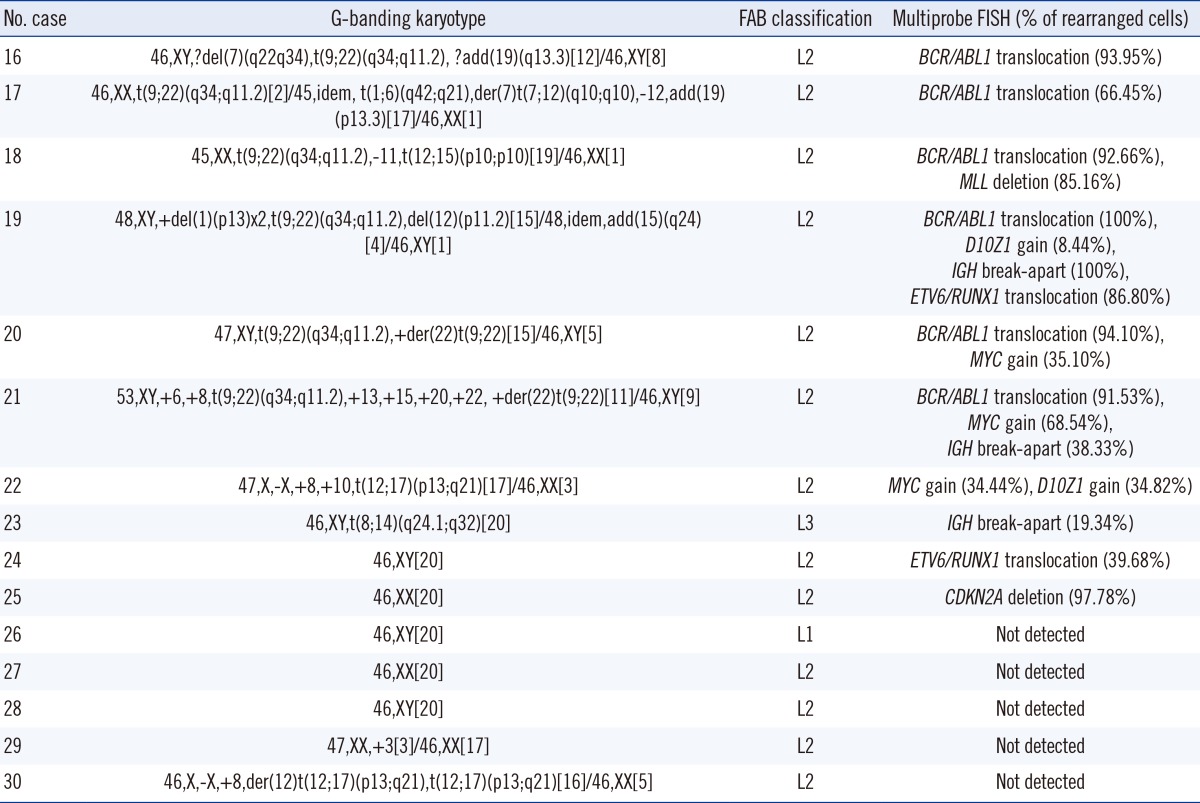
Among the 30 patients, G-banding detected clonal cytogenetic aberrations in 11 AML patients and 10 ALL patients. Tables 2 and 3 show the cytogenetic results of the patients, in comparison with multiprobe FISH assays.
Multiprobe FISH also detected the chromosomal aberrations detected by G-banding. Among the nine cases detected by normal G-banding, multiprobe FISH showed discordant results in two cases: ETV6/RUNX1 translocation (case no. 24) and p16 deletion (case no. 25). Additional aberrations were detected by multiprobe FISH in four patients: TP53 deletion (case nos. 5 and 6) and IGH break-apart (case nos. 19 and 21). Six cases were analyzed by traditional FISH probe (Abbott Molecular Inc., Abbott Park, IL, USA) for these aberrations to determine the false positive rate of multiprobe FISH. The ETV6/RUNX1 translocation in case 24, p16 deletion in case 25, TP53 deletion in cases 5 and 6, and IGH break-apart in cases 19 and 21 were detected by traditional FISH.
Quantitative FISH results for RUNX1/RUNK1T1 translocation (r2=0.698), PML/RARα translocation (r2=0.892), and BCR/ABL1 translocation (r2=0.697) showed good correlation with the G-banding and multiprobe FISH results.
DISCUSSION
In this study, multiprobe FISH identified additional genetic aberrations in 6 of 30 cases (2 and 4 in AML and ALL, respectively). Previous studies showed that AML FISH tests revealed additional genetic abnormalities in 4-8% of cases [13, 14, 15], including AML1/ETO fusion, MLL rearrangement, and CBFβ/MYH fusion. In this study, multiprobe FISH additionally identified TP53 deletion in AML cases 5 and 6. Case 5 carried (14;17)(q10;q10) translocation, but whether it causes TP53 deletion is unclear because the majority of the cytogenetic rearrangements are unbalanced translocations between 17p and another chromosome. Multiprobe FISH can reliably detect TP53 deletion. The activity of p53 may also be affected by PML/RARα translocations. Case 6 has TP53 deletion with PML/RARα translocations. TP53 mutations were found in 4.5-9% of AML cases [16]. TP53 deletion is not commonly used in FISH profiling in general laboratories. The results of this study show that the probe may be useful in the prognosis of patients without TP53 deletion [16,17,18]. Valencia et al. [7] reported the usefulness of the multiprobe FISH in AML, showing that this assay was very useful in the detection of an inv(16)(p13q22), a cryptic t(15;17)(q22;q21), and a cryptic deletion of the CBFβ. In ALL, previous studies showed that FISH revealed genetic aberrations not detected by G-banding in up to 50% of cases [13, 15]. In this study, multiprobe FISH detected additional genetic aberrations in ALL, including ETV6/RUNX1 translocation (case no. 24), p16 deletion (case no. 25), MYC rearrangement (case no. 21), and IGH break-apart (case nos. 19 and 21).
Previous studies showed that G-banding failed to detect ETV6/RUNX1 translocation, with a low sensitivity of 6% [17], whereas FISH was able to detect ETV6/RUNX1 translocation in about 21% of cases [18]. FISH is useful for detecting cryptic rearrangements such as ETV6/RUNX1 translocations. In previous studies, the rates of p16 deletion detected by FISH, but not by G-banding, were 25% [17] and 44.4% [13]. MYC rearrangement and IGH break-apart are not commonly used in FISH profiling in general laboratories. Patients with MYC rearrangement were originally thought to have poor prognoses, but they do respond well to intensive chemotherapy, which results in increased survival rates [21]. IGH gene rearrangement has been considered a useful marker for determining clonality as well as detecting minimal residual disease in lymphoid malignancies, with clonal rearrangement detected in around 82% of lymphoid tumors [22]. Most BCR/ABL1-positive ALL cells do not carry IGH gene rearrangement. In cases 19 and 21, IGH gene rearrangement was accompanied by BCR/ABL1 translocation and was nonfunctional. Klein et al. [23] investigated the function of antigen receptor signaling in B-cell precursor leukemia cells with BCR/ABL1 translocation. Analyses of the IGH loci showed that, in most cases, the dominant tumor clone does not carry a potentially functional IGH gene rearrangement; this rearrangement was a secondary V region gene rearrangement, which may have rendered an initially productive rearrangement nonfunctional, indicating ongoing recombination of IGH V region genes [23].
In conclusion, FISH shows higher detection rates of cytogenetic aberrations compared with G-banding. However, traditional FISH is restricted to the defined chromosome regions of the FISH probes used; it is also expensive and time-consuming. Since traditional FISH is limited by the number of probes used, it may underestimate the complexity of prognostic cytogenetic aberrations in acute leukemia. Multiprobe FISH can hybridize multiple probes to a single slide, thereby detecting higher number of genetic aberrations, and thus is more cost- and time-effective compared with traditional FISH. We conclude that multiprobe FISH assay is an efficient technique for the detection of cytogenetic aberrations in acute leukemia, providing critical information for diagnosis and prognosis, and for monitoring the course of the disease.
 XML Download
XML Download