

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Rheumatoid arthritis (RA) is a systemic autoimmune disorder characterized by articular inflammation eventually leading to joint destruction. Although the mechanism of RA pathogenesis is not fully understood, humoral and cellular immunity are known to be involved. In particular, CD4+ T lymphocytes and their cytokines have been reported to play a major role in the initiation of inflammation in this disease [1, 2].
CD4+ T helper (Th) cells are activated by the antigenic stimulation of T-cell receptors and differentiated into different subsets of effector Th cells. Among these cells, interferon-γ (INF-γ)-producing Th1 cells are predominant in RA [3]. Recent reports have suggested that interleukin-17 (IL-17)-producing Th17 cells are a new subset of cells critical to the pathogenesis of RA [2, 4]. IL-17 induces the production of inflammatory cytokines such as IL-1, IL-6, IL-8, and tumor necrosis factor-α (TNF-α) [5, 6], and it has been detected in the serum, synovial fluid (SF), and synovium of patients with RA [4, 7].
However, very few studies have focused on the role of Th17 cells in arthritis, and the published results are controversial. A previous report has suggested that Th17 cells are proinflammatory and play an important role in various autoimmune diseases, including RA [8]. Subsequently, Zhang et al. reported that the percentage of pure Th17 cells (CD4+INFγ-IL-22-IL17+) was significantly higher in RA patients than in osteoarthritis (OA) patients and healthy controls [9]. In contrast, Yamada et al. [10] reported that the frequency of Th17 cells was neither increased in the SF or peripheral blood (PB) of RA patients nor correlated with disease activity. Another study showed that the percentage of Th17 cells in the SF correlated with inflammatory activity in arthritis, irrespective of the type of disease [11]. To date, a few studies have quantified the prevalence of Th17 cells in RA, and their results have been discrepant [9-12]. Therefore, it is necessary to analyze the prevalence of Th17 cells in RA.
Recently, the Th17 cell-associated cytokines have been proposed. IL-6 and TNF-α induce the differentiation of Th17 cells, whereas IL-21 and IL-23 promote the proliferation of Th17 cells [8, 13, 14]. Recent studies [12, 15] have shown that the plasma levels of IL-21 and IL-23 are increased in RA and correlated with disease activity. In addition, a previous study reported that IL-23 levels are correlated with the SF and serum levels of IL-17 and TNF-α [16]. However, only a few previous studies have simultaneously examined the levels of major cytokines in RA.
In this study, we investigated the distribution of Th1 and Th17 cells in the PB and SF of RA and OA patients and measured the levels of related cytokines. We also evaluated the frequencies of Th1 and Th17 cells with regard to disease activity of RA and the relationship between their frequencies and inflammatory markers.
Go to : 
METHODS
1. Patients
In this study, we prospectively enrolled 55 RA patients (age, 55.2±14.1 yr; 14 men and 41 women) and 20 OA patients (age, 61.1±13.3 yr; 4 men and 16 women) referred to the outpatient clinic of the Rheumatology Department at Chungnam National University Hospital between September and November 2011. Among the 55 RA patients, 46 had been receiving disease-modifying antirheumatic drugs (DMARD). Corticosteroids (≤10 mg/day) were given to 39 patients, whereas the remaining 9 were newly diagnosed patients naïve to steroids and DMARD. Disease activity was assessed using the 28-joint disease activity score (DAS28) [17]. The study protocol was approved by the Institutional Review Boards of Chungnam National University Hospital and written informed consent was obtained from all participants.
The erythrocyte sedimentation rate (ESR) level and serum levels of C-reactive protein (CRP), rheumatic factor (RF), and anti-cyclic citrullinated peptide (CCP) were also measured. PB and SF samples were collected for mononuclear cell separation. SF was aspirated only in patients presenting with symptomatic effusion. Serum samples were collected and stored at 80℃ until assayed.
2. Th1 and Th17 analyses
1) Lymphocyte stimulation
PB and SF were diluted with phosphate-buffered saline (PBS; 1:1 and 1:2, respectively) and then layered on Ficoll-Paque separation media (GE Healthcare Bio-Science AB, Uppsala, Sweden). Mononuclear cells were separated by centrifugation and stimulated in 48-well plates at 1×106 cells/well with 50 ng/mL of phorbol myristate acetate (PMA) (Sigma Aldrich, St. Louis, MO, USA) and 1 µg/mL ionomycin in the presence of 10 µg/mL Brefeldin A for 6 hr at 37℃ in a 5% CO2 incubator.
2) Flow cytometric analysis
After stimulation, the cells were collected and washed with PBS (1,500 rpm for 10 min); thereafter, 5×105 cells were resuspended in 100 µL of PBS and incubated in the dark at room temperature for 30 min with 10 µL of anti-CD4-phycoerythrincyanin (PC) 5 (Beckman Coulter, Marseille, France). The cells were then fixed and permeabilized with IntraPrep (Beckman Coulter) according to the manufacturer's instructions. Subsequently, the cells were incubated in the dark at room temperature for 30 min with 20 µL anti-INF-γ-fluorescein-isothiocyanate (FITC) (Beckman Coulter) and 5 µL anti-IL-17-phycoerythrin (PE) (eBioscience, San Diego, CA, USA). The samples were analyzed using a Cytomics FC 500 flow cytometer (Beckman Coulter). In the flow cytometric analysis, lymphocytes were first gated in a forward scatter and side scatter, and then, at least 10,000 CD4-positive cells were analyzed. The CD4-positive cells were further classified as CD4+INFγ+IL17- cells (Th1), CD4+INFγ-IL17+ cells (Th17), and CD4+INFγ+IL17+ cells (Fig. 1). The isotype controls IgG1-FITC and IgG1-PE (Beckman Coulter) were used to correct compensation and detect nonspecific staining.
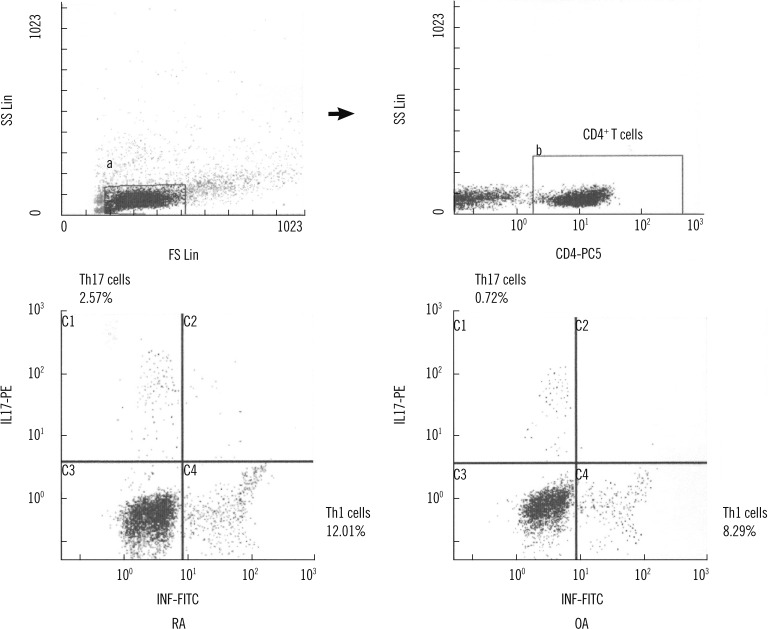 | Fig. 1The percentage of Th1 cells and Th17 cells in representative rheumatoid arthritis (RA) and osteoarthritis (OA) patients. Lymphocytes (a) were gated in a forward scatter (FS)/side scatter (SS) dot plot, and then CD4+ T cells (b) within indicated lymphocytes were isolated. CD4+ T cells were divided into CD4+INFγ+IL17- (Th1 cells), CD4+INFγ-IL17+ (Th17 cells) and CD4+INFγ+IL17+ cells.
Abbreviations: Th1, T helper 1; Th17, T helper 17; RA, rheumatoid arthritis; OA, osteoarthritis; INF, interferon; IL, interleukin.
|
3. Determination of IL-6, IL-17, IL-21, IL-23, and TNF-α
The serum levels of IL-6, IL-17, IL-21, IL-23, and TNF-α were quantified by ELISA according to the manufacturer's instructions (eBioscience). All stored samples were diluted 1 in 2 with the sample diluent provided in the kit and analyzed in duplicate. The concentration was calculated using the average optical density (OD) value. Serum samples with a concentration exceeding the highest standard were rediluted. The minimum detection limits for IL-6, IL-17, IL-21, IL-23, and TNF-α were 0.92, 0.5, 20.0, 4.0, and 2.3 pg/mL, respectively.
4. Statistics
All statistical analyses were performed using the MedCalc statistical software 11.3.0.0 (MedCalc Software, Mariakerke, Belgium). Continuous variables are presented as the mean±SD or median (95% confidence interval [CI]). Intergroup comparisons were made using the Student's t-test, Mann-Whitney U test, or Kruskal-Wallis test, where applicable. To assess the correlation between 2 parameters, linear regressions were calculated. Detection frequencies of cytokines were compared between groups using the chi-square test or Fisher's exact test when appropriate. A P value of less than 0.05 was considered statistically significant.
Go to :
RESULTS
1. Patient characteristics
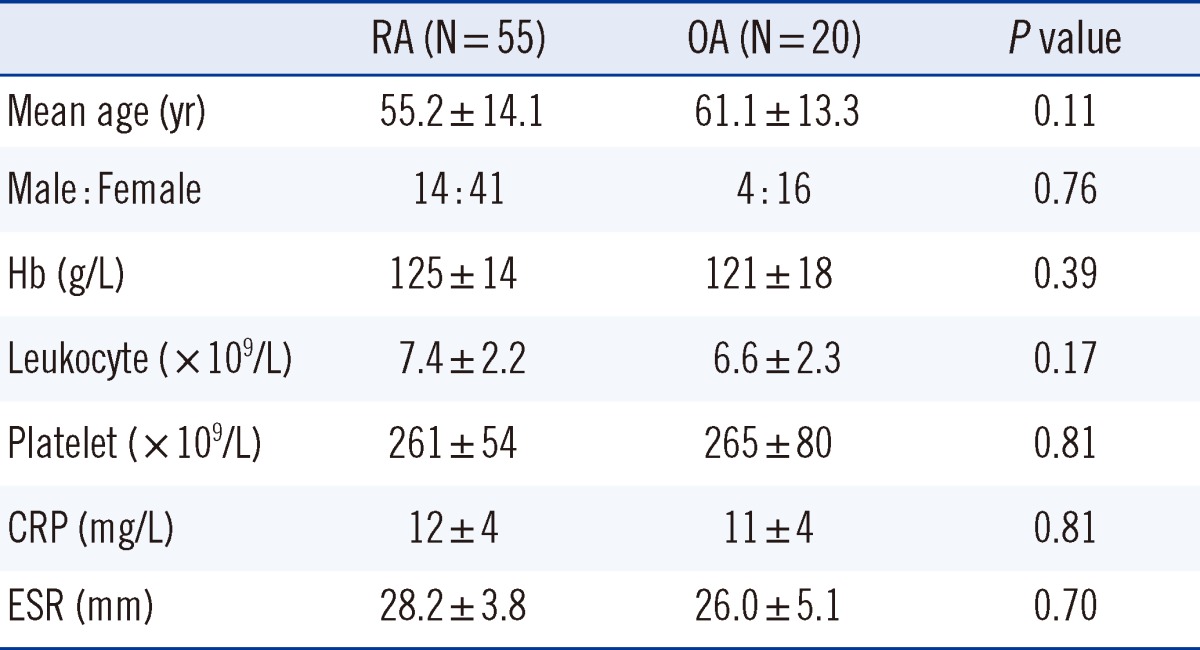
As illustrated in Table 1, no significant differences were observed between the RA and OA patients with regard to age and sex distribution. Furthermore, hemoglobin concentration, leukocyte count, and platelet count in RA patients were similar to those in OA patients. In addition, the 2 patient groups showed similar serum levels of CRP and ESR.
2. Frequency of Th1 and Th17 cells in RA and OA
PB samples were obtained from all 75 patients, and SF samples were collected from 3 RA patients and 5 OA patients. We identified Th1 and Th17 cells in PB and/or SF mononuclear cells after the samples were treated with PMA and ionomycin. Neither Th1 cells nor Th17 cells were detected in the RA and control specimens without stimulation treatment (data not shown).
The median percentages of CD4+ T cells were 30.05% (26.62-33.05%) and 32.42% (15.15-34.28%) in the RA and OA patients, respectively, indicating no significant intergroup difference (P=0.69). The median percentages of Th1 cells, Th17 cells, and CD4+INFγ+IL17+ cells were 10.67% (9.13-11.39%), 1.59% (1.08-2.09%), and 0.08% (0.05-0.10%), respectively, in the PB mononuclear cells (PBMCs) of RA patients, and 7.95% (6.70-10.78%), 0.93% (0.53-1.28%), and 0.06% (0.02-0.15%), respectively, in PBMCs of OA patients. The frequency of Th17 cells was significantly higher in RA patients than in OA patients (P=0.04), but the frequency of Th1 cells did not differ significantly between the 2 groups (P=0.19) (Table 2).
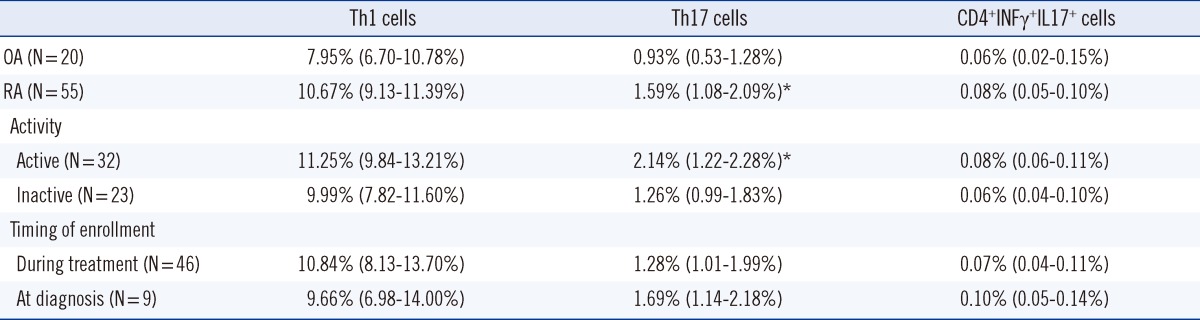
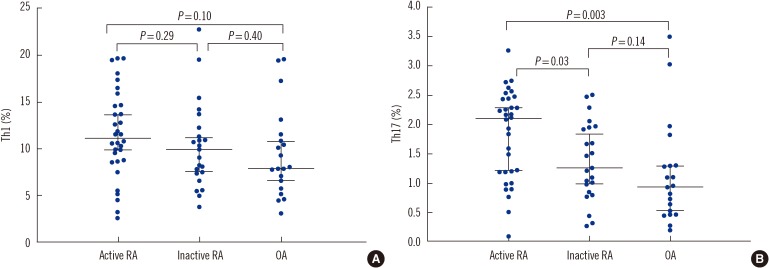
The median percentages of Th1 cells and Th17 cells were 11.25% (9.84-13.21%) and 2.14% (1.22-2.28%) in the 32 active RA patients (DAS≥2.6), and 9.99% (7.82-11.60%) and 1.26% (0.99-1.83%) in the 23 inactive RA patients. The frequency of Th17 cells was significantly higher in active RA patients than in inactive RA patients (P=0.03) or OA patients (P=0.003), but no significant difference in the frequency of Th1 cells was observed between active RA and inactive RA (P=0.29) or between active RA and OA patients (P=0.10) (Fig. 2). The median percentages of Th1 cells and Th17 cells were 9.66% (6.98-14.00%) and 1.69% (1.14-2.18%) in the 9 newly diagnosed RA patients, and 10.84% (8.13-13.70%) and 1.28% (1.01-1.99%) in the 46 RA patients under treatment. The frequencies of Th1 and Th17 cells did not show any significant difference between the 2 groups according to the treatment (P=0.53 and P=0.39, respectively) (Table 2). SF samples of 8 patients were analyzed. For the 3 RA patients, the median percentages of Th1 cells, Th17 cells, and CD4+INFγ+IL17+ cells were 12.91%, 1.92%, and 0.26% of the SF mononuclear cells, respectively, and for the 5 OA patients, the corresponding values were 10.68%, 1.19%, and 0.13%. These 8 patients, whose SF samples were analyzed for determining the frequency of Th1 and Th17 cells, showed higher percentages of both cell types in the SF samples than in PB samples although the number of samples tested was very small.
3. Relationships of the frequency of Th1 and Th17 cells with inflammatory indices or disease activity in RA patients
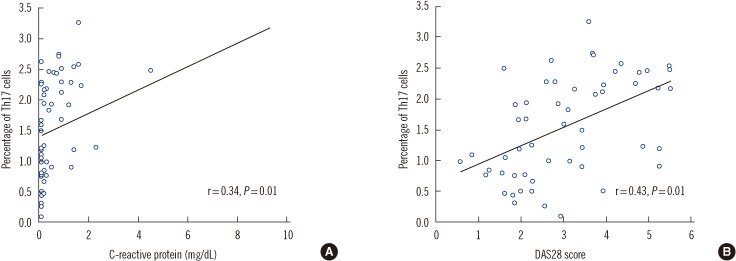
The percentage of Th1 cells was not significantly correlated with that of Th17 cells in both RA (r=0.26, P=0.07) and OA patients (r=0.31, P=0.12). In the RA patients, a significant positive correlation was found between the percentages of Th17 cells in the PBMCs and serum CRP (r=0.34, P=0.01) or ESR levels (r=0.30, P=0.03). However, Th1 cells in the PBMCs were not correlated with CRP or ESR levels. Furthermore, the percentages of the Th1 and Th17 cells in the PB were not correlated with leukocyte count or neutrophil percentage. In addition, Th1 and Th17 cell percentages in the PB were not correlated with the serum RF or anti-CCP levels. However, the frequencies of Th17 cells were positively correlated with the DAS28 (r=0.43, P=0.01), whereas those of Th1 cells were not (r=0.14, P=0.27) (Fig. 3). A trend of positive correlation between the percentages of Th17 cells and DAS28 was also observed in the 32 active RA patients but was not significant (r=0.30, P=0.13).
4. Serum cytokines in RA and OA
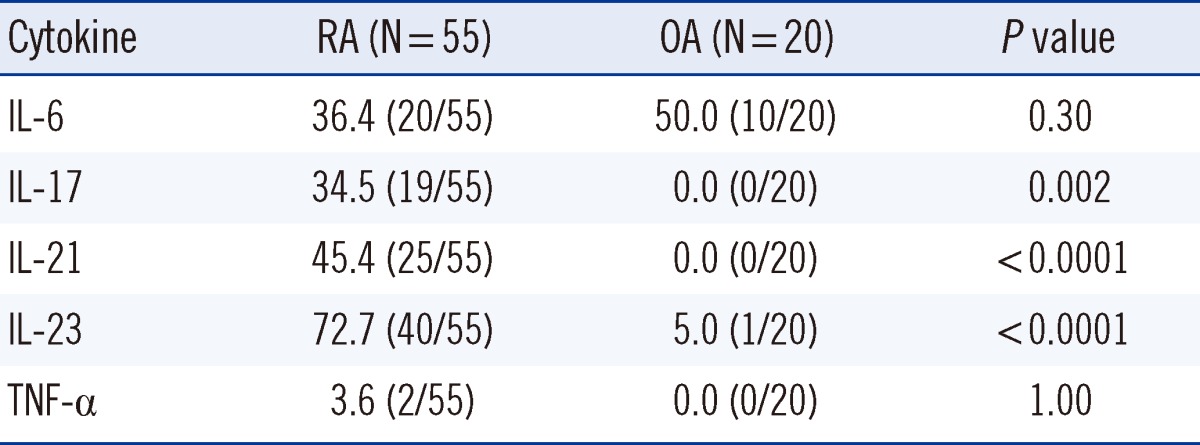
IL-17 and IL-21 levels were detectable in 19 (34.5%) and 25 (45.4%) RA patients, respectively, but in none of the OA patients (Table 3). Detectable serum levels of IL-23 were present in 40 (72.7%) RA patients and 1 (5.0%) OA patient, whereas serum TNF-α levels were detected in the serum of only 2 (3.6%) RA patients. Serum IL-6 levels were detectable in 20 (36.4%) RA patients and 10 (50.0%) OA patients. The frequency of detectable serum levels of IL-17, IL-21, and IL-23 was significantly higher in RA patients than in OA patients (P=0.002, P<0.0001, and P<0.0001, respectively), but that of IL-6 and TNF-α did not show any intergroup differences (P=0.30 and P=1.00, respectively).
In active RA patients, IL-6, IL-17, IL-21, IL-23, and TNF-α were detected in 50.0% (16/32), 46.9% (15/32), 62.5% (20/32), 81.3% (26/32), and 6.3% (2/32) patients, respectively. However, inactive RA patients showed detectable cytokines in 17.4% (4/23), 17.4% (4/19), 21.7% (5/23), 60.9% (14/23), and 0.0% (0/23) patients, respectively. The frequency of detectable serum levels of IL-6, IL-17, and IL-21 was significantly higher in active RA patients than in inactive RA patients (P=0.02, P=0.04, and P=0.006, respectively), but the frequency of detectable serum levels of IL-23 and TNF-α did not show any significant intergroup differences (P=0.13, and P=0.50, respectively).
For each cytokine, the frequencies of Th1 and Th17 cells showed no significant difference according to the detection of cytokine.
Go to :
DISCUSSION
Th17 cells are a distinct subset of T helper cells that play a role in the activation of the immune system by stimulating proinflammatory cytokine production via IL-17 [8]. Generally, INFγ or IL-17 in mononuclear cells cannot be detected by staining without stimulation. This fact held true in this study, where INFγ- or IL-17-expressing helper T cells in the PB or SF could be detected only after mitogen stimulation.
The percentage of Th17 cells was found to be relatively smaller than that of Th1 cells. In addition, the number of Th1 or Th17 cells in the SF was higher than that in the PB, although the number of comparable patients was very small. These results are consistent with those of previous studies [11, 18] that analyzed the frequency of peripheral and synovial Th17 cells in RA patients.
We found that the frequency of peripheral Th17 cells was significantly higher in RA patients than in OA patients, whereas the frequency of peripheral Th1 cells showed no significant intergroup differences. Although a previous study has reported contradictory results and has suggested no such difference between RA and healthy controls [10], the findings of more recent studies [9, 15, 19] are consistent with our current results. The higher frequency of Th17 cells in RA patients implies that these cells may potentially play a role in the pathogenesis of RA.
We also observed that the frequencies of peripheral Th17 cells were higher in patients with active RA than in those with inactive RA and that the frequencies were positively correlated with the DAS28 as well as serum CRP levels in RA patients. However, peripheral Th1 cells were not correlated with inflammatory markers or disease activity. Chen et al. reported that the baseline levels of peripheral Th17 cells were positively correlated with DAS28 before therapy and that a significant decrease in the frequencies of peripheral Th17 cells was observed after anti-TNF-α therapy, in parallel with decreased DAS28 [15]. A recent report also suggested that the percentages of synovial Th17 cells show a direct correlation with joint and systematic inflammation markers, whereas percentages of synovial Th1 cells do not show such a correlation [11]. Our findings support the notion that peripheral Th17 cells may influence inflammatory status and that their levels may reflect the disease activity in RA.
The present study showed that the serum levels of cytokines, determined by ELISA, were detectable in some RA patients but not in most OA patients. Compared to previous studies [9, 12, 15, 20, 21], the measured levels of cytokines in our study were rather low. We infer that the low cytokine levels in our study were due to variation in cytokine measurements because differences among cytokine levels have been reported in previous studies. Thus, we compared the frequency of detectable cytokines between RA and OA instead of the quantitative analysis of cytokine levels to investigate the effects of Th17-related cytokines in the pathogenesis of RA. A previous study has proposed that IL-6 plays a predominant role in directing the differentiation of Th17 cells in animal models of autoimmune disease [22]. Another recent study has suggested that TNF-α triggers the differentiation of T cells into Th17 cells [14]. In this study, the detection frequency of IL-6 and TNF-α in PB was similar in both OA and RA patients, but detectable levels of serum IL-6 were observed more frequently in active RA (50.0%) patients than in inactive RA (17.4%). Kang et al. [20] reported that IL-6 levels were higher in active RA patients than in inactive RA patients and that TNF-α levels were not different between the 2 groups. Although we could not accurately compare IL-6 levels between the 2 groups because IL-6 was not detected in some RA patients, we assumed that the measurement of serum levels of IL-6, unlike TNF-α, is related to disease status in RA.
We observed that the serum levels of IL-17, IL-21, and IL-23 were mainly detected in RA patients, and IL-17 and IL-21, in particular, were more frequently detected in active RA patients. Similarly, the serum levels of IL-21 and IL-23 were previously reported to be higher in RA patients than in healthy controls [12, 15, 21]. It is estimated that the serum levels of IL-21 and IL-23, which are related to the proliferation of Th17 cells, are highly specific for RA, and IL-21 and IL-23 could be candidate inflammatory biomarkers in RA. However, reports on levels of IL-17 have been inconsistent: some recent studies have shown that plasma IL-17 levels in RA patients did not differ from those in OA patients or healthy controls [9, 12, 23], whereas other studies have reported an elevation of the serum levels of IL-17 in RA patients [15, 24]. Notably, our finding supported a pathogenic role of IL-17 in RA. Inconsistent with our data, the disparate findings concerning IL-17 levels in a few previous reports may because of differences among the RA patients, medication administered, and the presence of RF [25].
Thus far, only a few reports on the correlation between the frequency of peripheral Th17 cells and serum levels of Th17-related cytokines have been published [9, 11], and most of these could not clearly establish this relationship, except for one study [15] that reported a correlation between the frequencies of Th17 cells and IL-17 levels. In this study, no differences were reported in the frequency of Th17 cells according to the detection of cytokine and our data could not prove an association between Th17 cells and Th17-related cytokines. Kim et al. [16] found that IL-23 levels are correlated with serum levels of IL-17 in RA, and IL-23 has been known to stimulate IL-17 production from Th17 cells [26]. In this study, detectable levels of IL-17 were observed in 19 (47.5%) of the 40 patients with detectable IL-23 levels and 19 (76.0%) of the 25 patients with detectable IL-21 levels. The limited number of cases of cytokine coexistence failed to show a correlation between IL-17 and IL-21 or IL-23. Further study is necessary to evaluate Th17 cells and Th17-related cytokines in RA.
In conclusion, our study demonstrated that the percentages of Th17 cells were higher and that detectable serum levels of the related cytokines IL-17, IL-21, and IL-23 were more frequently observed in RA patients than in OA patients; we also found that the frequency of Th17 cells correlated with the DAS28, ESR, and the serum CRP level. Although the sample size of this study was very small to establish a definitive conclusion, our findings implicate Th17 cells and Th17-related cytokines (IL-17, IL-21, and/or IL-23) in the pathogenesis of RA and suggest that Th17 cells may be associated with disease activity.
Go to :
 XML Download
XML Download