

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The emerging resistance to glycopeptide antibiotics (vancomycin and teicoplanin) observed in enterococci is soon becoming one of the most serious issues related to infection control. The first outbreak of vancomycin-resistant Enterococcus (VRE) in Turkey was reported in 1998 [1], and the increase in its prevalence since then has been associated with higher healthcare costs and mortality rates [2]. Vancomycin resistance in enterococci is mainly due to the acquisition of vanA and vanB genes, which have been primarily detected in Enterococcus faecium [3].
Asymptomatic intestinal colonization with VRE is widely reported, and it can act as a reservoir for dissemination and subsequent infection [4-6]. Effective infection control and prevention measures can reduce the colonization and transmission rates, thus reducing the infection rate. Early diagnosis of VRE colonization is, therefore, critical to reduce the incidence of VRE infections and outbreaks. Culture-based methods are typically used for the detection of VRE, which requires 24-72 hr for isolation, identification, and susceptibility testing [7, 8]. However, a screening assay that could detect VRE colonization in < 24 hr would prevent the spread of VRE by allowing earlier implementation of appropriate barrier precautions. Several nucleic acid amplification tests have been developed and evaluated for the detection of VRE, but quite a few of these require complex regimens for extraction and detection [9-12] or an enrichment step involving the use of a selective enrichment broth [13, 14] or isolates recovered from solid medium [15, 16]. The Vancomycin Resistance 3 Multiplexed Tandem PCR kit (AusDiagnostics, Alexandria, Australia) is designed for direct use on rectal swabs for active VRE surveillance. In this study, we aimed to evaluate this kit for early detection of VRE colonization.
METHODS
1. Specimens
A total of 211 non-duplicate rectal swabs collected at the Hematology and Oncology unit at Akdeniz University Faculty of Medicine during an outbreak and submitted to the Clinical Microbiology laboratory were used in this study. This study was performed in April 2012 in accordance with the institutional VRE surveillance program.
2. Culture method
Two rectal swab specimens were collected from all patients, and one was inoculated into Enterococcosel broth containing 6 µg/mL vancomycin (BD Diagnostic Systems, Sparks, MD, USA) and incubated in 5-10% CO2 at 35℃ for 24-72 hr. Black discoloration or cloudiness in the broth was considered positive; the culture was then subcultured on Enterococcosel agar containing 6 µg/mL vancomycin (BD Diagnostic Systems). Cultures were considered negative, if no growth was observed on the third day. Black colonies on Enterococcosel agar were identified as potential VREvancomycin-resistant enterococci; these were then subcultured to sheep blood agar plates and incubated at 35℃ for 24 hr. Catalase-negative, gram-positive cocci positive for leucine aminopeptidase (LAP; Remel, Lenexa, KS, USA) and L-pyrolidonyl-β-naphthylamide (PYR; Remel) were further identified using colony morphology, methyl-α-D-glucopyranoside (MDG; Sigma, Taufkirchen, Germany) test, and motility. Species identification and antimicrobial susceptibility testing was performed by using BD Phoenix System (BD Diagnostic Systems). Enterococcus faecalis strain (ATCC 29212) was used as a the control strain in the identification assays. The minimum inhibitory concentrations (MICs) of vancomycin and teicoplanin were determined by the E-test method according to the manufacturer's recommendations. The van gene was typed using the BD GeneOhm™ VanR Assay (BD Diagnostic Systems).
3. Vancomycin resistance 3 multiplex tandem PCR assay
All the specimens were studied with the PCR assay according to the manufacturer's instructions. Vancomycin Resistance 3 Multiplex Tandem PCR assay was configured to screen for VRE colonization in hospital patients by testing perianal and/or rectal swabs for the presence of vanA and vanB genes. The assay uses the principle of Multiplexed Tandem PCR employing 2 sequential PCR steps. Step 1 is multiplex amplification using primers homologous to all targets in the panel. The product from Step 1 is then diluted into individual wells for real-time PCR (Step 2) using primers "nested inside" the primers used for Step 1. This process is automated by the Easy-Plex system (AusDiagnostics). The Rotor-Gene Q thermal cycler (Qiagen, Hilden, Germany) was used for DNA amplification, which was measured by the increase in fluorescence when Eva-Green™ dye is incorporated into the DNA being formed. The 3 targets (vanA, vanB, and an internal control) were amplified together in Step 1 by using 3 tube strips for 24 samples. Step 2 is performed in individual wells fused together into a 72-position Gene-Disc. The assay could be completed in approximately 90 min for every 24 samples.
RESULTS
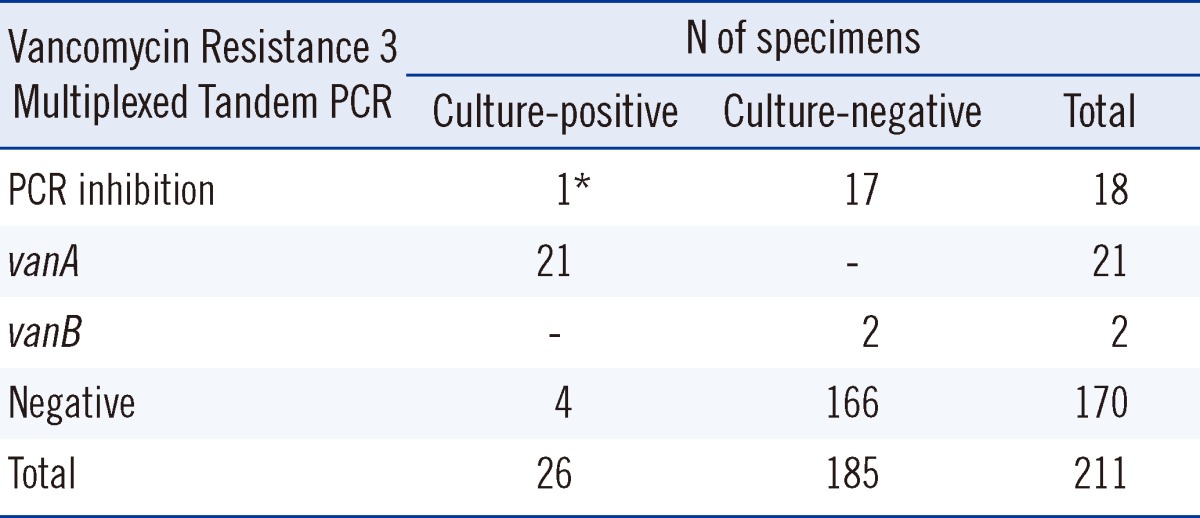
Of the 211 rectal swab samples, 18 (8.5%) were not effectively amplified by the PCR-presumably because of the presence of PCR inhibitors in the samples; one of them tested positive for VRE by using the enrichment culture method. Samples showing PCR inhibition were excluded from the study, leaving 193 samples for consideration. Comparative results for the culture-based method and PCR are listed in Table 1 and described in detail in the following results section. The PCR assay was assessed using the results obtained with the enrichment culture method as the gold standard. Of the 25 positive PCR results, 21 were positive for vanA, and 2, for vanB. All the 21 vanA-positive results tested positive for VRE by culture method; we confirmed vanA genotype by using BD GeneOhm™ VanR Assay. None of the vanB-positive PCR results confirmed with those obtained with the culture method. Four of the samples that tested positive in the culture method tested negative in the PCR assay. Compared to the culture method, the Vancomycin Resistance 3 Multiplexed Tandem PCR assay yielded a sensitivity of 84.0%, specificity of 98.8%, positive predictive value (PPV) of 91.3%, and negative predictive value (NPV) of 97.6%.
DISCUSSION
The increasing global prevalence of VRE [17-22] has led to increased interest in screening of patients for colonization and in development of methods for rapid, sensitive, and reliable detection of VRE [23]. Various commercial phenotypic and genotypic assays with different sensitivity and specificity are available for VRE screening [12, 24-30]; however, genotypic assays are generally more rapid and sensitive [28, 31, 32]. The Cepheid GeneXpert vanA/vanB assay, BD GeneOhm VanR assay, and other commercially available assays have high sensitivity and specificity for detecting vanA-positive specimens [24, 28-30], but a low specificity due to the comparably high rates of apparent false-positive vanB-positive specimens [12, 28]. The low specificity of detection of the vanB gene by various assays has been explained by the presence of commensal bacteria of the fecal flora carrying the vanB gene [8, 12, 13, 25, 28, 33]. Consistent with these findings, the 2 vanB genes we detected by PCR were not confirmed using the culture method. To the best of our knowledge, this is the first study involving Vancomycin Resistance 3 Multiplexed Tandem PCR assay, and like all other methods studied for the active surveillance and detection of VRE, it produced false-positive results due to vanB. Therefore, it has been suggested that follow-up culture should be performed on all vanB-positive specimens [12, 27]. The vanB genotype has never been detected in this hospital until date [1, 34]. In our sample set, vanB was present in 8.0% (2/25) of the total number of specimens, and in this setting, confirmation with the culture method has prevented unnecessary precautions during isolation of strains.
In our study, 18 (8.5%) of the 211 rectal swab samples contained PCR inhibitors. Because one of these samples tested positive for VRE using the culture method, this finding highlights a disadvantage of the assay. PCR inhibitors are often present in stool samples, and may originate from dietary components, polysaccharides, or chlorophyll from herbs and vegetables, bile salts, urea, glycolipids, hemoglobin, and heparin [35]. Although automated nucleic acid extraction systems improve the consistency and throughput of PCR tests, these systems may prove insufficient for removal of PCR inhibitors [36]. Although various protocols have been developed to remove PCR inhibitors (e.g., heat treatment before PCR, chloroform extraction, treatment with activated carbon, sample dilution), they may affect the sensitivity of the assay or lead to false-negative results [35].
In our study, 12.9% of the specimens tested positive for VRE, and all the strains were found to display vanA phenotype. This is not an unexpected result, considering that there has been only 1 report describing the isolation of vanB-positive E. faecium in Turkey [37]. As a part of our study, we collected samples during an outbreak period from the Hematology and Oncology unit and from pediatric and adult patients. Many of them could have been treated with antibiotics, which might increase the selective pressure for VRE. However, as the antibiotic therapy received by the patients was not documented for the present study, the effects of antibiotics could not be compared.
The Vancomycin Resistance 3 Multiplexed Tandem PCR kit had an excellent NPV and PPV for the detection of vanA. Because the kit can rapidly identify patients not carrying vancomycin-resistance genes and those who have acquired the vanA and vanB genes, healthcare professionals can, within 3 hr of patient admission, determine appropriate infection control policies to prevent cross infections. Strains testing positive for vanA can be rapidly identified as VRE, but strains testing positive for vanB need to be confirmed by the culture method.
In conclusion, direct application of Vancomycin Resistance 3 Multiplexed Tandem PCR assay on rectal swabs is a reliable option to give rapid and accurate results for vanA-VRE surveillance.
 XML Download
XML Download