

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Sphingobacterium species are non-fermentative, gram-negative rods that are positive for biochemical tests such as catalase and oxidase production, but are negative for that of indole [1]. Sphingobacterium species were previously described as unnamed bacteria (part of Centers for Disease Control and Prevention group IIk). Holmes et al. [2, 3] proposed the genus name Flavobacterium for the bacteria, while in 1983, Yabuuchi et al. [4] first proposed the name Sphingobacterium for the genus. The genus Sphingobacterium was created to classify organisms that contain large amounts of sphingophospholipid compounds in their cell membranes, and have other taxonomic features that distinguish them from Flavobacterium species [4].
Sphingobacterium species have usually been isolated from soil, plants, foodstuffs, and water sources, but the isolation of the species from human clinical specimens has been rarely reported worldwide [5]. Furthermore, Sphingobacterium spiritivorum have been rarely isolated from clinical specimens of immunocompromised patients, and there have been no case reports of S. spiritivorum infection in Korea to our knowledge. We report a case of S. spiritivorum bacteremia in a patient, who had undergone chemotherapy for acute myeloid leukemia.
CASE REPORT
A 68-yr-old woman was admitted to our hospital for dyspnea that had lasted for 7 days. She had no history of smoking or pulmonary diseases. A physical examination did not find lymphadenopathy or organomegaly. An initial complete blood cell count showed the following results: hemoglobin, 11.3 g/dL; white blood cell counts, 2.86×109/L (neutrophils, 40%; lymphocytes, 57%; and monocytes, 3%); platelet counts, 47×109/L. A peripheral blood smear revealed pancytopenia with no leukemic blasts.
A bone marrow (BM) examination was performed to evaluate pancytopenia. The BM aspirate smears and cytochemical staining showed increased myeloblasts (40%) and other myeloid precursors. The patient was diagnosed with acute myeloid leukemia, not otherwise specified, based on the 2008 WHO classification system [6].
She received chemotherapy of cytarabine 160 mg and idarubicin 20 mg for 3 days, and idarubucin 20 mg for 4 days. One day after the chemotherapy ended, her body temperature increased to 38.3℃. Her blood pressure, pulse rate, and respiratory rate were 90/70 mmHg, 110/min, and 20/min, respectively. Her C-reactive protein (CRP) level increased to 6.31 mg/dL, and her procalcitonin level was 0.08 ng/mL (reference range: <0.05 ng/mL).
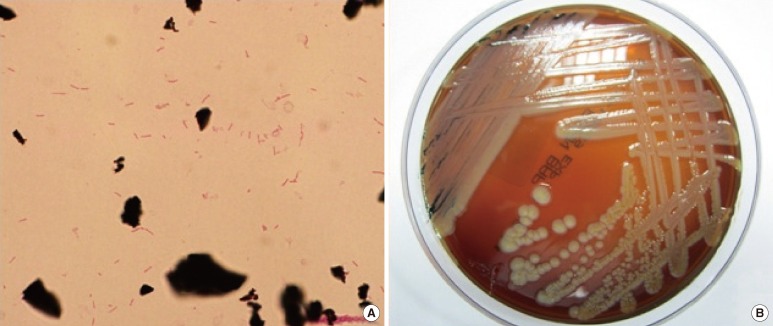
Four sets of blood cultures were collected: 2 sets from peripheral veins and 2 sets from the central venous catheter. The patient received empirical antibiotic therapy with intravenous cefepime (2 g every 12 hr). After 1 day of incubation, gram-negative bacilli grew in an aerobic culture bottle that contained the culture from the central venous catheter. After 2 days of incubation, Gram-negative bacilli also grew in an aerobic culture bottle containing the culture from the peripheral vein (Fig. 1A). The positive culture broth was inoculated onto a blood agar plate (BAP) and a MacConkey agar plate (MAC) and incubated for 48 hr at 37℃ with 5% CO2. Non-hemolytic, light yellow-colored colonies grew on the BAP (Fig. 1B). A few colonies also grew on the MAC. Catalase and oxidase tests were positive, but the indole test was negative. The organism was identified as S. spiritivorum with 98.0% probability using the Vitek 2 Gram-Negative Identification card (BioMérieux inc., Marcy-l'Etoile, France).
To confirm the identity of the isolate, 16S ribosomal RNA (rRNA) sequencing analysis was performed. InstaGene Matrix (Bio-Rad Laboratories, Hercules, CA, USA) was used to extract the bacterial genomic DNA, and the first 500 base pairs on the 5' end of the 16S rRNA gene were amplified and sequenced using MicroSeq 500 16S rDNA Bacterial Identification PCR and Sequencing Kits (Applied Biosystems, Foster City, CA, USA). The sequencing product was analyzed on a 3130 Genetic Analyzer (Applied Biosystems) according to the manufacturer's instructions.
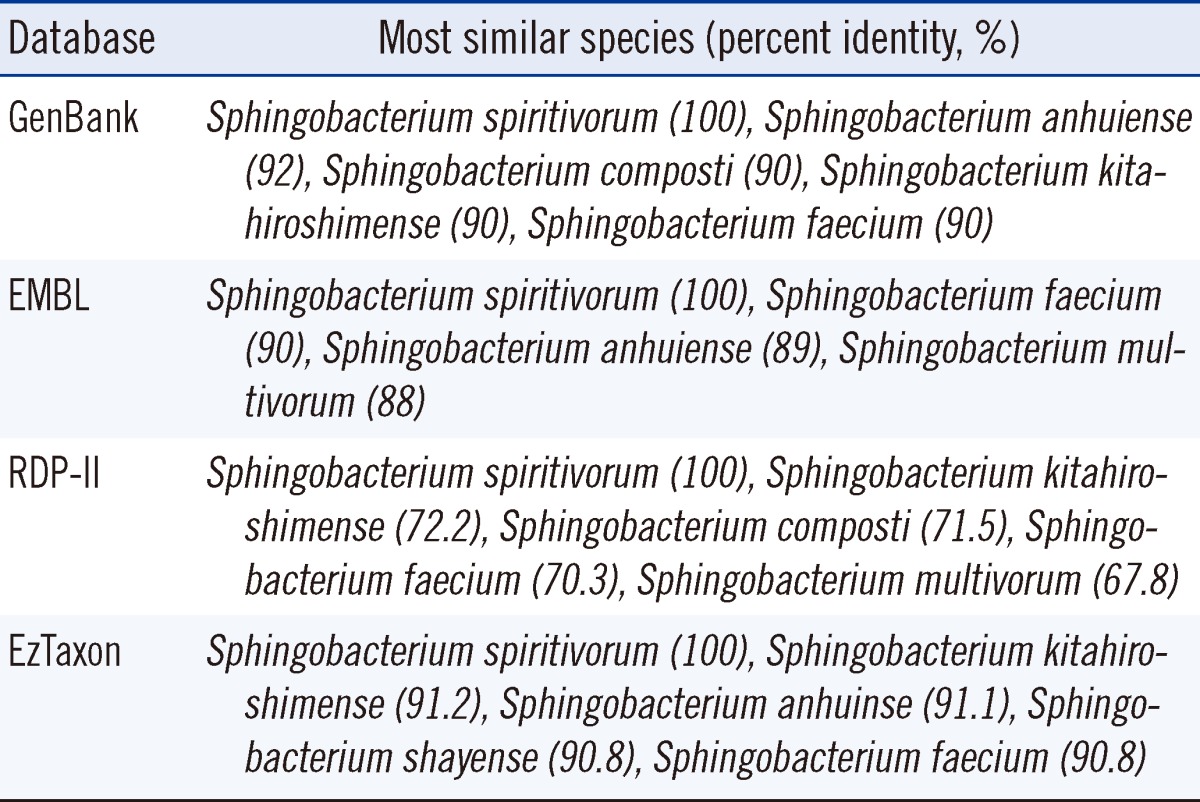
The resulting sequence of the patient-derived isolate was compared with sequences stored in GenBank (http://www.ncbi.nlm.nih.gov/genbank), EMBL (The European Molecular Biology Laboratory, http://www.ebi.ac.uk/embl), RDP-II (The Ribosomal Database Project, http://rdp.cme.msu.edu), and EzTaxon (http://www.eztaxon.org) databases. The percent identity between the isolate from the patient and its closely related Sphingobacterium species of the 4 databases are shown in Table 1. The GenBank and RDP-II databases showed that the 16S rRNA gene sequence of the isolate from the patient was 100% homologous with that of S. spiritivorum strain NCTC 11386 (Accession number: GenBank, NR044077.1; RDP-II, S000752320). The EMBL and EzTaxon databases showed that the 16S rRNA gene sequence of the isolate from the patient was 100% homologous with that of S. spiritivorum strain ATCC 33861 (Accession number: EMBL, ACHA02000013; EzTaxon, ACHA01000008). The isolate from the patient showed percent identity of >99% with S. spiritivorum and >0.8% separation from other species. Thus, the isolate was confirmed to be S. spiritivorum [7].
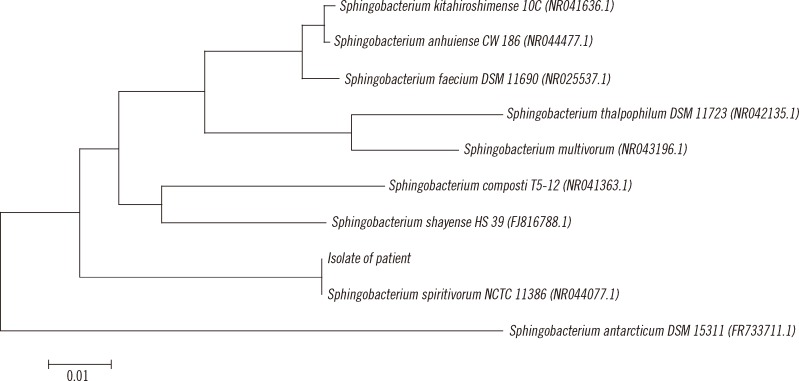
For phylogenetic analysis, the resulting sequence was compared with those of reference strains of the most closely related Sphingobacterium species present in the GenBank databases. A phylogenetic tree was constructed by the neighbor-joining method using the Microseq 500 bp 16S rRNA sequences (Fig. 2).
Antimicrobial susceptibility was tested using the AST-N132 card from the Vitek 2 system (BioMérieux). The isolate was susceptible to cefepime, ciprofloxacin, levofloxacin, meropenem, minocycline, and trimethoprim-sulfamethoxazole; had moderate susceptibility to cefotaxime, ceftazidime, imipenem, and ticarcillin-clavulanic acid; but was resistant to amikacin, aztreonam, colistin, gentamicin, piperacillin, piperacillin-tazobactam, ticarcillin, and tobramycin.
The central venous catheter was removed. The antibiotic regimen was changed from cefepime to ciprofloxacin, because nephrotoxicity was suspected to be due to increased blood urea nitrogen and creatinine levels. After 3 days, the patient's fever subsided. Subsequent blood culture tests were negative for S. spiritivorum and any other microorganism. However, on the fifth day of ciprofloxacin therapy, she developed a fever again and her general condition worsened. On the eleventh day, she died of septic shock.
DISCUSSION
Sphingobacterium species are non-fermentative, non-motile, non-spore-forming aerobic gram-negative bacilli. They produce catalase, oxidase, and urease [1]. Sphingobacterium species grow on both BAP and MAC [2, 3]. Colonies are yellowish, circular, slightly convex, smooth, opaque, and non-hemolytic on BAP after 2 days of incubation [2, 3]. To date, 15 species, including S. anhuiense, S. antarcticus, S. bambusae, S. canadense, S. composti, S. daejeonense, S. faecium, S. heparinum, S. kitahiroshimense, S. multivorum, S. piscium, S. shayense, S. siyangense, S. spiritivorum, and S. thalpophilum, have been described in the genus Sphingobacterium [4, 8-17].
Sphingobacterium species are usually isolated from soil, water, and plant material, and only a few case reports of human infections caused by the species have been published [5]. Previously reported Sphingobacterium species isolated from human clinical specimens were S. multivorum and S. spiritivorum. To date, 7 cases of S. multivorum infection have been reported worldwide in relation to septicemia [5, 18-20], peritonitis [21], respiratory tract infection [22], and necrotizing fasciitis [23]. Only 3 cases of S. spiritivorum infection have been reported worldwide [24-26]. The present case and previously reported cases are compared in Table 2. In 2002, Marinella [24] first described a case of cellulitis-associated sepsis caused by an S. spiritivorum infection. In 2003, Tronel et al. [25] reported a case of S. spiritivorum bacteremia. In 2005, Kronel et al. [26] reported a case of cellulitis-associated sepsis caused by S. spiritivorum from the water reservoir of a steam iron.
In the present case, the patient was in an immunosuppressed condition due to the chemotherapy to treat acute myeloid leukemia. The patient was diagnosed with a catheter-related blood-stream infection because the time interval of positive blood culture signs from those between the peripheral vein and central venous catheter cultures was more than 2 hr. The source and transmission route of the S. spiritivorum infection in this case may have been a skin entry site of an intravascular device or a subcutaneous path of the catheter that had been in a close proximity with the natural habitats of this organism.
The 16S rRNA sequencing analysis can be a useful and definitive method particularly for the identification of clinically significant bacterial isolates with ambiguous biochemical profiles or of rarely encountered bacterial species [27, 28]. We confirmed the identity of the blood isolate, first identified biochemically as S. spiritivorum, by 16S rRNA sequencing analysis.
Sphingobacterium species are generally resistant to aminoglycosides and polymyxin B, but are susceptible to quinolones and trimethoprim-sulfamethoxazole in vitro. Susceptibility to β-lactam antibiotics is known to vary [1]. In 2009, Lambiase et al. [29] reported that 13 S. multivorum and 8 S. spiritivorum isolates from sputum samples in 332 patients with cystic fibrosis were resistant to aminoglycosides, but susceptible to quinolones and trimethoprim-sulfamethoxazole. They also found that S. multivorum isolates were resistant to all β-lactams, whereas the S. spiritivorum isolates were susceptible to ceftazidime, piperacillin, and carbapenems. The isolate of this case was susceptible to cefepime, meropenem, minocycline, as well as ciprofloxacin, levofloxacin, and trimethoprim-sulfamethoxazole.
This is the first reported case of human S. spiritivorum infection in Korea, which shows that S. spiritivorum can be a fatal human opportunistic pathogen in immunocompromised patients, despite human infection being rare.

 XML Download
XML Download