

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Most clinical laboratories have been using automated analyzers since the mid-1950s with the first introduction of autoanalyzers for laboratory use [1]. However, automated systems for blood banks are not common in Korea, because of the abundance of well-trained technologists, inexpensive reagents, low medical insurance fees, and difficulty automating blood bank testing methods [2]. Automated laboratory testing has several advantages including increased quality of pre-analytical steps, reduced error rates, reduced operator exposure to potentially hazardous biological materials, and minimized non-value-added steps in the laboratory testing process [1, 2]. The reliability of results and economic feasibility should be secured when implementing automation. Many published studies compared manual techniques with automated systems for ABO/Rh(D) typing and unexpected antibody screening; however, most of these studies evaluated the concordance rates of results. This study aimed to compare the estimated costs and required times for ABO/Rh(D) typing and unexpected antibody screening in a clinical laboratory using an automated system and manual methods.
METHODS
1. Cost estimation by workflow analysis
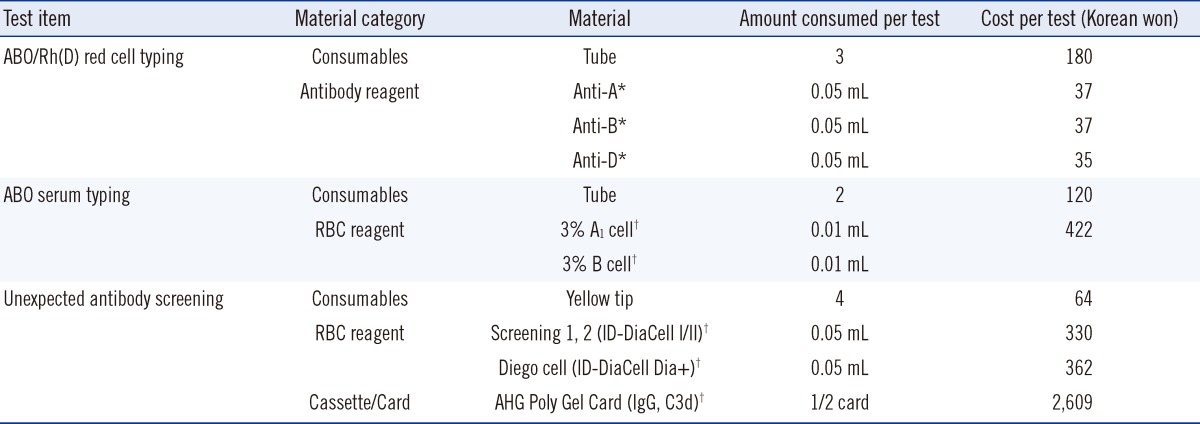
The total cost included direct costs (e.g., reagents and consumables), depreciation costs, and labor costs. Direct costs for using manual methods and the automated system for red cell and serum typing for ABO/Rh(D) and unexpected antibody screening are described in Table 1 and 2, respectively. Depreciation costs were taken into account only when the instruments used were directly related to the tests and purchased within the last 5 yr. Since any of instruments in the present study was not purchased within the last 5 yr, depreciation costs were not included.
Labor costs were calculated on the basis of the average operator salaries and unit values. The average operator salary per minute in the present study was 359 Korean won. We defined a unit value (minutes) as the hands-on time to test one sample from sample preparation to reporting of the results. To estimate the unit values, the workflows of ABO/Rh(D) typing and unexpected antibody screening using the manual techniques and automated system were recorded by video, and work processes identified were analyzed individually. All processes performed by operators using clinical samples in a clinical laboratory were recorded. The unit values for unexpected antibody screening did not contain the times required for centrifugation and incubation, because the operators worked on other tasks in the meantime.
2. Data collection
The workflow in a transfusion medicine laboratory in March 2012 was recorded. "Regular working hours" were defined as 8:30 AM to 17:30 PM from Monday through Friday except holidays. "unsocial working hours" were defined as 17:30 PM to 8:30 AM from Monday through Friday and all Saturdays, Sundays, and holidays. The numbers of tests performed during regular and unsocial working hours were recorded separately in March 2012. In addition, the numbers of ABO/Rh(D) typing and unexpected antibody screening tests alone and simultaneously in March 2012 were recorded.
3. Manual method for ABO/Rh(D) typing using the tube technique
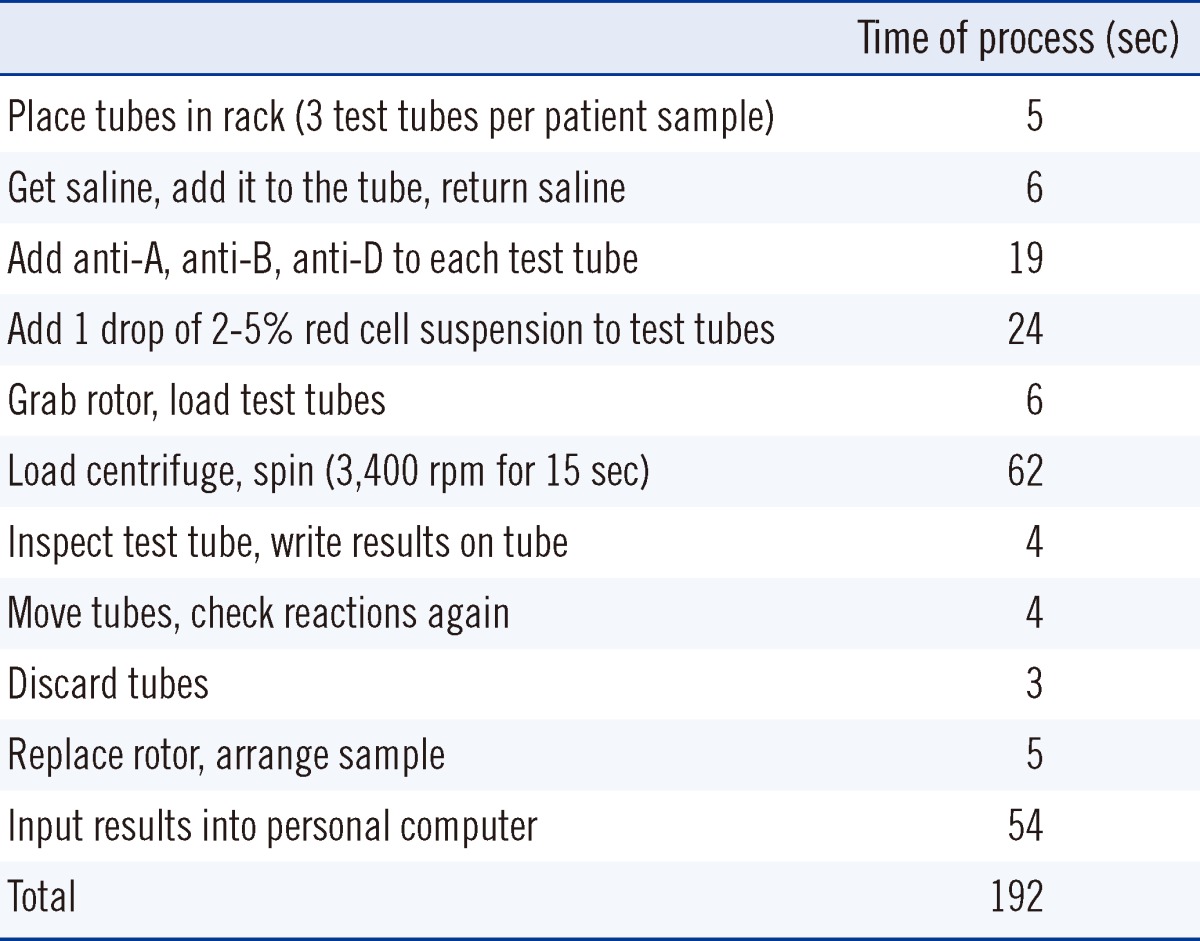
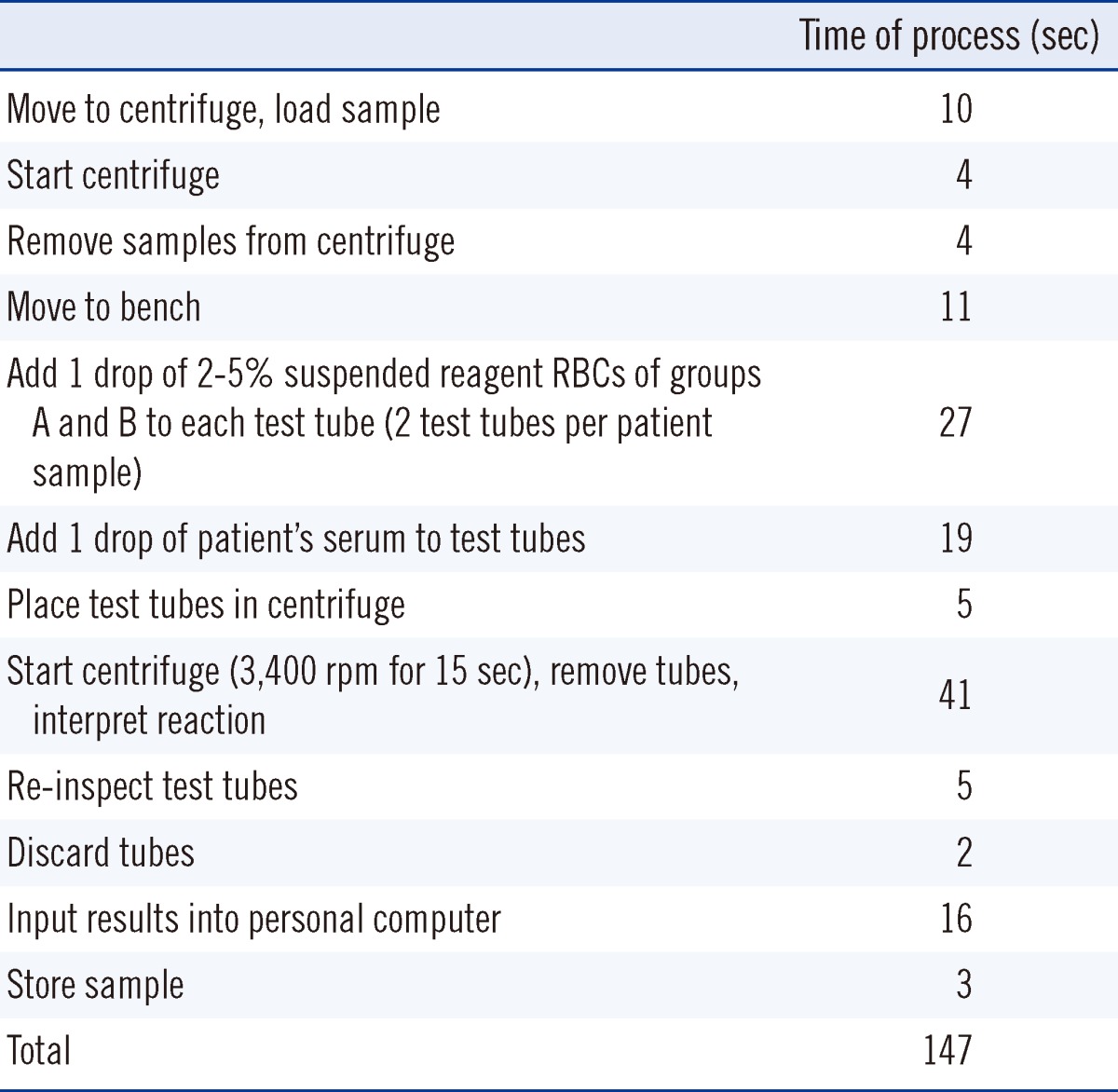
The tube test was used for ABO/Rh(D) red cell and serum typing. ABO typing required both antigen typing of red cells for A and B antigens as well as screening of the serum for the presence of anti-A and anti-B isoagglutinins. The protocols for red cell and serum typing are described in Table 3 and 4, respectively. Anti-A, anti-B, and anti-D blood grouping reagent IgM monoclonal antibodies (Millipore, Billerica, MA, USA) and ID-Dia Cell ABO (DiaMed AG, Cressier s/Morat, Switzerland) were used to determine the ABO/Rh(D) types. Red cell and serum typing were performed by different operators to reduce the possibility of incorrect blood type reports and detect ABO subgroups. During unsocial working hours, only one operator examined the red cell and serum typing, while the other operator re-examined serum typing the next day. During regular working hours, most samples were tested in batches.
4. Manual method for unexpected antibody screening using the microcolumn agglutination technique
ID-DiaCell I-II-Diego (DiaMed AG) and microtubes of the ID-Card "LISS/Coomb" (DiaMed AG) containing polyspecific anti-human globulin were used for unexpected antibody screening. According to the manufacturer's instructions, 50 µL of each test cell reagent ("ID-Diacell") was pipetted, and 25 µL of the patient's serum was added to each microtube. The ID-Card was incubated for 15 min at 37℃ in the ID-Incubator and centrifuged for 10 min in the ID-Centrifuge. The results were read and scored.
5. Automated system for ABO/Rh(D) typing and unexpected antibody screening using the microcolumn agglutination technique
The automated technique used was the Ortho AutoVue Innova system column agglutination technique (Ortho Clinical Diagnostic, Raritan, NJ, USA). For the AutoVue Innova, 0.8% Affirmagen A1, B Grouping Red Blood Cell (Ortho Clinical Diagnostic), and ABO/Rh Reverse Cassette (Ortho Clinical Diagnostic) were used to determine ABO group and the Rh(D) type of red cells; 0.8% Surgiscreen Reagent Red Blood Cell (Ortho Clinical Diagnostic), and the Polyspecific Anti-Human Globulin Cassette (Ortho Clinical Diagnostic) were used for unexpected antibody screening.
RESULTS
Among the 2,164 samples for ABO/Rh(D) typing in March 2012, 1,949 and 215 samples were tested during regular and unsocial working hours, respectively. Moreover, 1,255, 786 and 909 samples were tested solely for ABO/Rh(D) typing, solely for unexpected antibody screening, and both simultaneously, respectively. During regular working hours and the entire study period, the operators tested averages of 12 and 5.5 test samples simultaneously, respectively.
The total times consumed for one test using an automated analyzer for ABO/Rh(D) typing, unexpected antibody screening, and both during regular hours were 8.4, 23, and 24.7 min, resp-ectively; total times using the manual method were 5.65, 27.6, and 33.25 min, respectively.
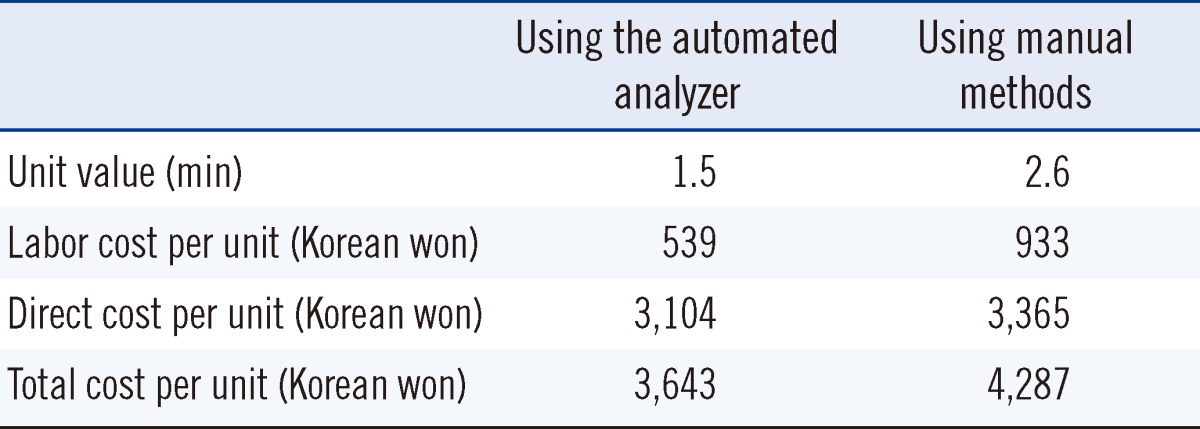
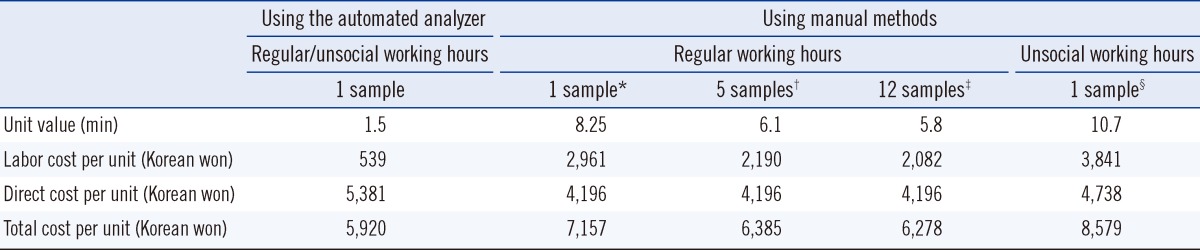
The unit values for manually testing one test sample were 3.2 minutes for red cell typing (Table 3) and 2.45 min for serum typing (Table 4). The unit values for ABO/Rh(D) typing per test sample were 5.65 and 8.1 min during regular and unsocial working hours, respectively. The unit values of ABO/Rh(D) typing during regular working hours were 3.5 and 3.2 min when 5 and 12 samples were tested simultaneously, respectively. The unit value for unexpected antibody screening was 2.6 min (Table 5). The unit values using an automated analyzer for ABO/Rh(D) typing and unexpected antibody screening as well as both tests simultaneously were 1.5 min (Table 5).
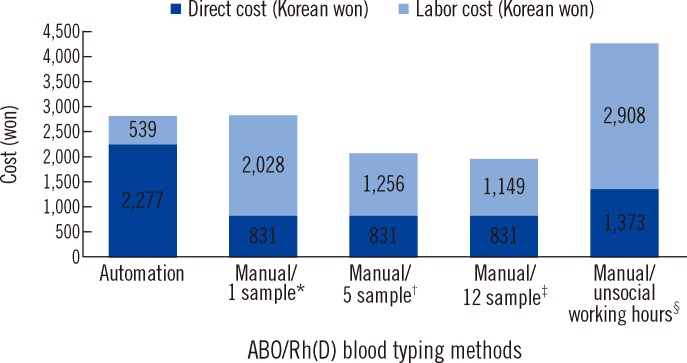
The analysis of the total cost of ABO/Rh(D) typing revealed that the total cost of using an automated analyzer was lower than that of testing one sample at a time using the manual technique but higher than that of testing several samples simultaneously (Fig. 1). Because the direct cost of testing using the manual te chnique was very inexpensive, the labor cost composed most of the total cost of the manual technique (Fig. 1). The total cost of unexpected antibody screening using an automated analyzer was lower than that using the manual technique (Table 5). The total cost of testing both ABO/Rh(D) typing and unexpected antibody screening simultaneously for one sample using an automated analyzer was lower than that using the manual method (Table 6).
DISCUSSION
In the present study, the unit values of ABO/Rh(D) typing and unexpected antibody screening both individually and simultaneously required for one test sample using the automated analyzer were less than those required using the manual methods. The total time consumed for one test sample for ABO/Rh(D) typing using an automated analyzer was more than that using the manual method. However, the total time consumed to analyze one sample for unexpected antibody screening using the automated analyzer was less than that using the manual method. In the present study, performing ABO/Rh(D) typing and unexpected antibody screening simultaneously shortened the turnaround time, which is similar to the findings of previous studies. Lee et al. [3] reported that the turnaround time for the antibody screening test was significantly shorter when using the AutoVue Innova than the tube method; up to 5 times more samples could be tested without requiring more labor. Shin et al. [4] simulated the turnaround times of ABO/Rh(D) typing with unexpected antibody screening and found that they are significantly lower using the AutoVue Innova than the manual methods. In that study, the times consumed for one test using the AutoVue Innova were 9, 23, and 23 min for ABO/Rh(D) typing, unexpected antibody screening, and both simultaneously, respectively; those using the manual method were 5, 30, and 30 min, respectively. This means that less hands-on time is required for pipetting and mixing the samples and reagents, operating the incubator and centrifuge, and carrying the cassettes. Chizhevsky et al. [5] demonstrated that using an automated system for ABO/Rh(D) typing and unexpected antibody screening improves productivity compared to using the manual methods by decreasing the hands-on time required. Besides transfusion medicine, automation in a clinical laboratory decreases labor requirements. Sarkozi et al. [6] reported that the introduction of a robotic system for perianalytical automation substantially improved productivity and decreased operational costs in a clinical chemistry laboratory. This system enabled them to significantly increase their workload while reducing personnel.
The costs of tests using automated systems in a transfusion medicine laboratory are reasonable. In the present study, the total cost of ABO/Rh(D) typing using an automated analyzer was lower than that of testing only one sample at a time using the manual technique but higher than the cost of testing when several samples were tested simultaneously. This is because labor is the main cost of the manual technique. However, automated systems perform the routine tasks of test processes, allowing qualified staff to spend more time on other activities that add more value to the process [2]. The total cost of unexpected antibody screening using an automated analyzer was lower than that using the manual technique, because both the direct and labor costs of a single test using the manual technique were more expensive. The total cost of simultaneous unexpected antibody screening and ABO/Rh(D) typing using an automated analyzer was lower than that using the manual technique. A previous report indicated the costs of ABO/Rh(D) typing and unexpected antibody screening using an automated blood test analyzer to be 4,588 and 3,416 won, respectively [7]. The reason for the difference in the costs of ABO/Rh(D) typing and unexpected antibody screening between the present and previous reports is the lower material costs in the present study, including the ABO/Rh Reverse Cassette and AHG Poly Cassette (IgG, C3d).
It is imperative that ABO/Rh(D) typing and other tests in blood banks are accurate, because errors cause fatal transfusion complications [8]. ABO/Rh(D) typing and unexpected antibody screening tests using the AutoVue Innova produce reliable results [9]. Shin et al. [4] compared automated and manual results; the concordance rates were 100%, 99.6%, and 100% with respect to forward ABO typing, reverse typing, and Rh typing tests, respectively. However, 10 cases were discrepant between the results using automated and manual methods, probably due to weak red blood cell antibodies. Microaggregations missed by the tube method highlighted the limitations of humans and the need for a more sensitive and objective protocol [10]. Lee et al. [3] reported concordance rates between AutoVue Innova and manual methods of 99.6% and 100% for ABO/Rh(D) typing and unexpected antibody screening, respectively; the cause of the discrepancy was hemolysis of the specimens. Kim et al. [9] analyzed 136 samples using the unexpected antibody screening test and found that 2 results were positive only on the AutoVue Innova and not the LISS/Coombs card; these 2 results were identified as being anti-Lea because of the use of frozen specimens and specimens with less volume. In addition, automated system can reduce error rate. Han et al. [11] reported the use of automated equipment dramatically reduced the risk priority number compared to manual processes.
The present study provide information about the overall distribution and comparison of the costs and workload of tests performed using different methods for ABO/Rh(D) typing and unexpected antibody screening. Contrary to popular belief, the results showed that ABO/Rh(D) typing using an automated analyzer incurs less unit value and cost than using a manual technique when only one sample is tested at a time, despite inexpensive reagents. Furthermore, unexpected antibody screening using an automated analyzer incurs less unit value and cost than using the manual technique regardless of working hours. The results of the present study support the use of automated equipment to reduce variability while increasing operator safety and the quality of test results.

 XML Download
XML Download