

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Deletion of the long arm of chromosome 20q [del(20q)] is one of the common recurring chromosomal abnormalities associated with myeloid malignancies [1]. When del(20q) is present as an isolated abnormality, it is associated with a good prognosis for MDS as defined by the International Prognostic Scoring System (IPSS) [2]. However, the prognosis of MDS is less favorable with a high rate of transformation to acute leukemia when del(20q) is part of a complex karyotype. Accordingly, del(20q) as an isolated abnormality must be distinguished from cases of other chromosomal rearrangements for better stratification of prognosis. For de novo AML, isolated del(20q) is known to be associated with poor response to treatment and reduced survival [1, 3].
Recently, single nucleotide polymorphism array (SNP-A)-based karyotyping has been applied as a high-resolution whole-genome scanning tool. A major advantage of SNP-A over metaphase cytogenetic analysis (MC) is its ability to detect hidden chromosomal defects, including submicroscopic (cryptic) aberrations or copy neutral loss of heterozygosity (CN-LOH). SNP-A can be used to identify CN-LOH through simultaneous measurement of DNA copy number and information of genotype calls. CN-LOH cannot be recognized by conventional MC, FISH, or array comparative genomic hybridization (array CGH) because it shows long stretches of homozygosity without a concurrent change in the gene copy number [4]. Regions of CN-LOH may contain pathologically relevant genes harboring deleterious homozygous mutations that may impact clinical outcomes [4, 5]. For example, CN-LOH of 9p is associated with JAK2 homozygous mutations [4, 5].
Here, we report a case of an isolated del(20q) abnormality identified using MC, but with the additional genomic aberrations identified using SNP-A-based karyotyping.
CASE REPORT
A 39-yr-old man presented with fever for a month (February 2007). Initial laboratory evaluation showed a white blood cell (WBC) count of 61×109/L with 96% blasts, a hemoglobin count of 91 g/L, and a platelet count of 47×109/L. Bone marrow (BM) analysis revealed that 96% of nucleated cells were replaced by myeloblasts of variable sizes and some azurophilic granules. Cytochemical analysis showed that the myeloblasts were positive for Sudan black B (SBB) but negative for myeloperoxidase (MPO), naphthol AS-D chloroacetate esterase (SE), and α-naphthyl butyrate esterase (NSE) stains. Flow cytometric immunophenotyping of BM revealed that leukemic cells were positive for CD13, CD33, CD56, and HLA-DR and negative for CD34, CD14, CD19, and CD3. The diagnosis of AML without maturation was made on the basis of WHO classifications of tumors of hematopoietic and lymphoid tissue 2008 [2].
Conventional cytogenetic analysis using BM aspirates revealed 20 metaphases with 46,XY,del(20)(q11.2) (Fig. 1). FISH analysis with D20S108 (Abbott Molecular/Vysis, Des Plaines, IL, USA) probe confirmed a 20q12 deletion in 99% of interphase cells; nuc ish(D20S108×1)[198/200]. Using FISH, other rearrangements such as BCR/ABL1, RUNX1/RUNX1T1, PML/RARA, CBFB/MYH11, and MLL were found to be negative (data not shown).
For the SNP-A, DNA was extracted from BM (QIAGEN DNA purification kit; Qiagen, Hilden, Germany) according to the manufacturer's instructions. SNP-A was performed using a Genome-wide Human SNP 6.0 Array (Affymetrix, Santa Clara, CA, USA) and analyzed using Genotyping Console Version 4.0 software (hg18) (Affymetrix). In order to detect the somatic origin copy number alterations distinguished from constitutional polymorphic copy number variants (CNVs), the lesions identified using SNP-A were compared with the database of genomic variants (http://projects.tcag.ca/variation/). When regions of copy number changes were located within those of CNVs, we did not consider them as the somatic changes and excluded them from the final results. To detect somatic CN-LOH, we excluded homozygous stretches of DNA regions less than 25 Mbp in the interstitial chromosomal regions, except those encompassing telomeric regions of the chromosome, according to an algorithm adopted in a previously published study [4]. The SNP-A identified CN-LOH of 11q13.1-q25, not detected by MC (Fig. 2); arr 11q13.1q25 (65,966,684-134,375,799)×2 hmz. Furthermore, SNP-A allowed for a more precise definition of the breakpoints of the 20q deletion (20q11.22-q13.31); arr 20q11.22q13.31 (32, 253,686-55,192,062)×1 (Fig. 2). Unexpectedly, the terminal regions showed a gain on chromosome 20q; arr 20q13.31q13.33 (55,192,062-59,271,669)×3 (Fig. 2).
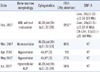
The patient received 2 cycles of standard induction chemotherapy (daunorubicin 60 mg/m2×3 days and Ara-C 200 mg/m2×7 days), but he did not achieve complete remission. Four months after the initial diagnosis (June 2007), he presented with paralysis in both legs. Cerebrospinal fluid analysis revealed 100% of leukemic cells with a WBC count of 0.38×109/L and RBC count of 0.01×109/L, indicating central nervous system (CNS) involvement in the leukemia. He received intrathecal chemotherapy with cytarabine (15 mg/m2). One month later (July 2007), BM biopsy showed hypercellular marrow with abnormal localization of immature precursors (ALIP), and MC revealed 100% of metaphase cells with del(20)(q11.2). Three months later (October 2007), he died due to invasive pulmonary aspergillosis and neurologic complications induced by leukemic cell infiltrations of the CNS (Table 1).
DISCUSSION
In the present study, we described a case of isolated del(20q) abnormality with additional 11q CN-LOH identified using SNP-A-based karyotyping. Our patient was found to have CNS involvement in the leukemia and was unable to achieve remission. During the follow-up, no additional abnormalities or clonal evolutions were detected by MC. This result suggests that identifying additional CN-LOH using SNP-A may be associated with a poor prognosis.
An isolated del(20q) is generally associated with a better prognosis in MDS, whereas AML patients have a significantly shorter overall survival [1-3]. Cases that have del(20q) with one or more additional chromosomal abnormalities predict a poor prognosis [3]. Therefore, we hypothesized that AML patients with isolated del(20q) may have, in fact, additional chromosomal abnormalities not identified by MC. One study also showed that additional CN-LOH or copy number changes could be identified by SNP-A analysis in patients with del(20q) as the isolated abnormality by MC [6].
As for the prognostic impact of 11q CN-LOH, one study showed that the 11q CN-LOH region was present only in a few fractions of the cells in the MDS phase; however, in the late relapse AML sample, the 11q CN-LOH region was present in more than 90% of leukemic cells. This finding suggests that clones with 11q CN-LOH may have conferred a selective growth advantage during the AML transformation and may be associated with a poor prognosis [7].
In particular, somatic CN-LOH on 11q is associated with homozygous mutations of the c-Cbl gene as a known oncogene encoding E3 ubiquitin ligase, which is involved in the ubiquitylation and degradation of active protein tyrosine kinase receptors [7, 8]. A previous study showed that oncogenic c-Cbl mutations were acquired in a subset of myeloproliferative neoplasms (MPN) with poor prognosis or during evolution to AML and that clones with homozygous mutations have a selective growth advantage over those with heterozygous mutations [9]. In the present study, c-Cbl mutation sequencing was not conducted.
For a prognostic impact of the additional abnormalities that were not detected by MC, another study confirmed that cases with isolated del(5q), which is known to be a good prognostic factor, showed adverse clinical courses when additional genomic imbalances were identified using array CGH [10]. Similarly, we treated a 40-yr-old man with relapsed AML (data not shown). MC revealed del(9)(q22q34) as an isolated abnormality. SNP-A identified not only deletions in the regions of 9q13-q22.3, but also additional genomic aberrations of CN-LOH on 6p25.3-p12.1 and 7q31.33-q36.3. Because of general weakness, the patient received conservative treatment without chemotherapy, and he died due to complications from pneumonia and sepsis. In contrast, a separate case involved a 69-yr-old man with chronic myelomonocytic leukemia with isolated del(20q) according to MC (data not shown). SNP-A showed interstitial deletion on chromosome 20q (20q11.23-q13.32), but no additional abnormalities were observed. He received 5 cycles of azacitidine chemotherapy and continued complete hematologic remission until the last follow-up (3 yr), although isolated del(20q) was persistently identified by MC.
Taken together, we recommend that in cases with isolated chromosomal abnormalities such as del(20q), del(5q), and del(9q), molecular techniques such as SNP-A or array CGH should be performed to identify additional CN-LOH, which may be associated with the poor prognosis.
Apart from the ability to detect CN-LOH, another advantage of SNP-A is its high-resolution power (less than 1 Mbp), which allows for further detection of cryptic lesions that cannot be detected by MC as well as the precise delineation of aberrations. The small size of chromosome 20 and the limited number of G-bands on its long arm has hampered cytogenetic characterization of 20q breakpoints; subtle deletions or rearrangements may be beyond the resolution of traditional MC. Using SNP-A, our case showed an interstitial deletion pattern of 20q. The deletion was located between bands 20q11.22 and 20q13.31 (23 Mbp), and the distal region was duplicated (20q13.31-q13.33, 4 Mbp). For the commonly deleted region (CDR) of chromosome 20q, a study using SNP-A defined 2 CDRs [6]; CDR1 was located between bands 20q11.23 and 20q12 and CDR2 was within bands 20q13.12. The deleted regions in our case encompassed these 2 CDRs. Similarly to our case, another study demonstrated that the 20q deletion showed an interstitial pattern according to SNP-A in most cases [6]. The rarity of true monosomy 20 suggests that retained or duplicated genes on chromosome 20 are essential for the survival of mutant clones [6]. Taken together, these findings indicate that tumor suppressor genes are located in the deletion region and oncogenes, in the duplicated region of chromosome 20.
In summary, we report a case of an isolated del(20q) abnormality with additional genomic aberrations identified using SNP-A-based karyotyping. This study suggests that a presumably isolated chromosomal abnormality according to MC may have additional genomic aberrations, including CN-LOH. SNP-A-based karyotyping may be helpful for identifying true isolated cases from cases in combination with additional genomic aberrations not detected by MC. Further study is needed to determine whether additional aberrations identified by SNP-A have a negative effect on prognosis in larger cohorts of AML patients.


 XML Download
XML Download