

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Neuromyelitis optica (NMO; also known as Devic syndrome) is a chronic inflammatory demyelinating disorder of the central nervous system (CNS), which was first described in the late 19th century by E. Devic and others [1]. It preferentially affects the optic nerves and the spinal cord, thus frequently manifests as recurrent optic neuritis (RON) and longitudinally extensive transverse myelitis (LETM) [2, 3]. The condition which is considered to be a type of neuromyelitis optica spectrum disorder (NMOSD) includes NMO and an array of high-risk NMO disorders such as Asian optic-spinal multiple sclerosis (OSMS), recurrent myelitis associated with longitudinal extensive spinal cord lesions, recurrent isolated or simultaneous bilateral optic neuritis (RON/BON), and optic neuritis (ON) or myelitis/LETM in the context of certain organ-specific and non-organ-specific autoimmune diseases or with brain lesions typically observed in cases of NMO [4, 5]. Due to its relapsing course with rare spontaneous remission, the accumulation of irreversible deficits and rapid progression of NMO often renders patients severely disabled. These characteristics highlight the need to distinguish NMO from other demyelinating CNS conditions as early as possible; however, it is often difficult to differentiate inflammatory demyelinating CNS disorders that have differing etiologies but similar clinical presentations and cerebrospinal fluid (CSF) and magnetic resonance imaging (MRI) findings. In particular, both NMO and multiple sclerosis (MS) have a relapsing-remitting course in the majority of cases, thus NMO has been typically considered to be a localized form of MS due to the lack of an NMO-specific laboratory test [3, 5, 6].
However, recent reports suggest that NMO is a distinct disease entity with a fundamentally different pathogenic mechanism than that of MS or other demyelinating diseases. An NMO-specific IgG, designated NMO-IgG, and antibodies to aquaporin-4 (AQP4) that serve as relevant antigens of NMO-IgG, are detectable in 60-90% of patients with NMO but are virtually absent in patients with MS and other inflammatory and non-inflammatory neurological diseases [7-10]. This evidence of autoantibody-mediated NMO pathogenesis enabled the development of therapeutic strategies targeted to the humoral arm of the immune system. Treatments based on B cell- and antibody-depleting strategies such as rituximab administration and plasmapheresis have been effective in combination with conventional immunosuppressive treatment, in contrast to the inefficacy of these approaches for treating MS and other diseases associated with inflammatory lesions [11-13].
In 2004, Lennon et al. demonstrated that NMO-IgG was capable of specifically binding to CNS microvessels, pia mater, subpia mater, and Virchow-Robin spaces in rodent brain tissue by using an indirect immunofluorescence method [7]. The target antigen of this autoantibody was quickly identified to be AQP4, the most abundant water channel in the CNS [8, 14]; subsequently, the immunopathogenic role of AQP4 antibodies in NMO was reported [14]. The presence of AQP4 antibodies has been verified by various methods, including visualization of AQP4-antibody immunoprecipitates by western blotting, fluorescence immunoprecipitation assay (FIPA), ELISA, and cell-based indirect immunofluorescence assay (CIIFA) [14-18]. The sensitivity and specificity of these tests were variable in approximately 60-90% and 90-100% of cases, respectively, depending on the method used. With the full native conformation of AQP4 antigen, the antibody is known to enhance the sensitivity and specificity of its binding [15]. Therefore, FIPA and CIIFA studies using human embryonic kidney (HEK) cells transfected with AQP4 as the source of antigen resulted in improved performance relative to other assays for the diagnosis of NMO and related disorders, thus differentiating them from other demyelinating disorders [15].
Recently, commercially available CIIFA was introduced by EUROIMMUN AG (Lubeck, Germany), which utilizes fixed, AQP4-transfected HEK cells on slides as an antigenic substrate. The aim of this study was to evaluate the diagnostic performance of CIIFA compared to FIPA for the detection of AQP4 antibodies and to assess the usefulness of CIIFA for the diagnosis of NMO and high-risk NMO in routine clinical practice using a commercially available CIIFA kit.
METHODS
1. Patients
We included 36 patients for the initial comparison of different assay methods and another 101 patients for whom AQP4 testing was requested at the neurology clinic from June 2010 through March 2011 to investigate the performance of the CIIFA-based AQP4 antibody test. For the purpose of diagnosis, a systemic work up including demographic features, neurologic manifestations, serologic findings, and brain and spinal cord MRI scans were performed in all patients; patients were initially evaluated clinically without consideration of their NMO-IgG or AQP4 assay status. Clinical diagnosis of NMO, ON, and myelitis with spinal cord lesions extending over 3 or more vertebral segments by MRI, was made according to the revised diagnostic criteria proposed by Wingerchuk et al. (2006), with the exception of NMO-IgG or AQP4 assay status [19]. Diagnosis of high-risk NMO included Asian OSMS, LETM (monophasic or relapsing), BON/RON, and ON or myelitis/LETM associated with systemic autoimmune disease or with brain lesions typical of NMO. In addition, various neurological disorders were included when differential diagnoses were necessary from NMOSDs, for example MS, acute disseminated encephalomyelitis (ADEM), and clinically isolated syndromes (CIS) such as brain stem syndrome (BS), acute myelitis, or ON that did not meet the diagnostic criteria of high-risk NMO.
In our comparison study, 14 patients with NMO, 11 patients with NMOSD (6 LETM, 3 RON, and 1 OSMS), 7 patients with MS, and 4 patients with other neurologic diseases (OND) were included. Forty-six serum samples from 36 patients were collected at the time of initial diagnosis and/or during treatment. The samples were aliquoted and stored at -70℃ for the comparison study. One aliquot from each patient was sent to Dr. Angela Vincent's laboratory in the Department of Clinical Neurology, University of Oxford, Oxford, UK, to be tested by FIPA and CIIFA; another aliquot was used for CIIFA at Samsung Medical Center. The serum samples of 101 patients who consecutively enrolled for the prospective investigation were analyzed for the presence of AQP4 antibodies by CIIFA at Samsung Medical Center. The diagnoses of the 101 patients included 6 NMO, 24 LETM, 11 BON/RON, 31 CIS (17 BS, 10 myelitis, 4 monophasic ON), 7 MS, 6 ADEM, 2 autoimmune neurologic diseases, and 14 miscellaneous OND. This study was approved by the institutional review board of Samsung Medical Center.
2. CIIFA for AQP4 antibody detection
CIIFA was performed using the commercially available kit from EUROIMMUN AG according to the manufacturer's instructions at Samsung Medical Center (CIIFA A); the results from our assay were compared with those measured in Dr. Vincent's laboratory at the University of Oxford (CIIFA B), according to a protocol developed in-house [20]. The principles of both tests are basically identical. Briefly, human M23 AQP4 complementary DNA was cloned into a plasmid to yield enhanced green fluorescent protein (EGFP)-tagged AQP4. Then, HEK 293 cells were transfected with EGFP-AQP4 using the standard polyethyleneimine transfection method. The transfected cells were subsequently fixed with 0.5% formaldehyde on glass slides and were used as an antigen substrate. The cells were incubated with either patient or control serum samples diluted with phosphate buffered saline (PBS) containing 1% bovine serum albumin or 0.002% Tween 20 in either 1:10 dilutions for commercial CIIFA or 1:20 dilutions for the in-house CIIFA protocol for 30 min to 1 hr at room temperature (RT), washed 3 times with buffer, and then incubated with goat anti-human IgG fluorescein isothiocyanate (FITC)-conjugated secondary antibody. After antibody labeling, cells were washed 4 times in PBS and observed under a fluorescence microscope. Since the EGFP-AQP4 protein is synthesized in the cytoplasm and expressed on the cell membrane, a flat, smooth, fine granular green fluorescence signal is detected both in cytoplasm and at the cell surface membrane, but not in the nucleus. The BIOCHIP slide is composed of combinations of transfected and non-transfected cellular substrate for each patient's test, and the negative and positive control sera are provided to ensure quality control of the entire procedure. The fluorescence was scored from weak positive to 4 positive (w+ to 4+), according to the intensity scale of the conventional fluorescence anti-nuclear antibody test (FANA; Fig. 1). The presence of AQP4 was confirmed if the intensity was 1+ or stronger. For the semi-quantitative evaluation, the titer was defined as the sample dilution factor for which specific fluorescence was identifiable. The dilution series was 1:10 to 1:640, by a factor of 2.
3. FIPA for AQP4 antibody detection
FIPA was performed according to the in-house protocol described in detail elsewhere [20]. Cloning of AQP4 and transfection of human HEK 293 cells were performed in a same manner as that of CIIFA. EGFP-AQP4 extract was acquired from lysis and high-speed centrifugation of EGFP-AQP4-transfected HEK 293 cells and was used as an antigen substrate. Individual serum samples were incubated with cellular extract at 4℃ overnight. Then, the IgG-AQP4 complexes were precipitated using Protein A sepharose beads, washed thoroughly, resuspended in extract buffer, and transferred to a 96-well black PCR plate. The amount of EGFP-AQP4 bound by antibody was detected by counting the green fluorescence at 512 nm (excitation 472 nm; cut-off 495 nm) on a fluorescence plate reader (SpectraMAX Gemini XS; Molecular Devices, Sunnyvale, CA, USA). Results were given as arbitrary quantitative fluorescence unit (FU) and the mean +3SD from healthy control samples was used as a cut-off value. In this study, the cut-off value was derived from 14 healthy controls and was 575 FU.
4. Statistical analysis
The sensitivity and specificity of autoantibody detection by each assay, individually and in combination, was determined by reference to the clinical diagnoses. Antibody positivity and levels between groups were analyzed by Fisher's exact test and the Mann-Whitney test, respectively. The McNemar test was used to analyze the agreement between the 2 CIIFA results and between CIIFA and FIPA, and also to compare the significance of differences in sensitivity and specificity between CIIFA and FIPA. P<0.05 was considered significant. Analyses were performed using MedCalc® version 12.0.4.0 (MedCalc Software, Mariakerke, Belgium).
RESULTS
1. Comparison of FIPA and CIIFA for the detection of AQP4 antibodies
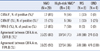
We performed the AQP4 antibody detection assay in 46 serum samples of 36 patients using FIPA and 2 different CIIFA methods, the first was commercially available (CIIFA A) and the other was developed in-house (CIIFA B). The concordance rate between the 2 CIIFA methods was 76% (Kappa coefficient (κ=0.6522, 95% confidence interval [CI]=0.4331-0.8713, P=0.2891) and between CIIFA A and FIPA B was 89% (κ=0.781, 95% CI=0.5997-0.9623, P=0.3750). There were 11 discordant results between CIIFA A and CIIFA B, where only 3 were true discrepancies and the other 8 resulted in discrepancies mainly due to inability of the CIIFA B to provide data regarding the conclusive fluorescence pattern, as the in-house cellular substrate preparation was of variable quality. The results of each test are summarized in Table 1.
The sensitivity of CIIFA using the commercial kit (data from CIIFA A) and FIPA in this comparison set was 86% and 79% in NMO patients and 55% and 36% in high-risk NMO patients, respectively. The combination of CIIFA and FIPA did not increase the sensitivity of detection of the presence of AQP4. Neither the sensitivity nor the specificity differed significantly in the 2 assays (McNemar test; Tables 1, 2).
The semiquantitative titer of CIIFA was well correlated with the arbitrary quantity (FU) of FIPA (r=0.66; Fig. 2). The AQP4 titers measured by CIIFA and FIPA were elevated in NMO patients compared to those in high-risk NMO patients (1:240 vs. 1:180 and 8,390 FU vs. 4,059 FU, respectively).
2. Frequency of AQP4 antibodies detected by CIIFA in patient populations
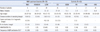
For the routine detection of AQP4 antibodies as a clinical laboratory practice, the commercially available CIIFA was used. AQP4 antibodies were detected in 17 of 101 consecutive patients in whom AQP4 testing was requested at the neurology clinic during a 10-month period. The clinical characteristics and presence of other autoantibodies are summarized in Table 3. NMO patients who were AQP4 antibody-positive were predominantly female (males : females=1:5) and were associated with a longer disease duration than other patients. Autoantibodies such as anti-nuclear antibodies (ANA), anti-Ro antibodies (SSA), and anti-La antibodies (SSB) were found in 1 (17%) NMO patient. AQP4 antibodies were present in 6/6 (100%) patients with NMO, in 7/24 (29%) LETM patients, and 1/11 (9%) RON/BON patients, but only 3/65 (4.6%) in control patients (2/31 in CIS patients, 1/2 in patients with autoimmune neurological diseases (AND), and none in 51 other demyelinating neurological diseases such as MS, ADEM, and OND (Chi-square test, P<0.0001; Fig. 3). These results correspond to a sensitivity of 100% and a specificity of 95% for the test in NMO, and to 39% and 94%, respectively, if NMO and high-risk NMO patients such as LETM and RON/BON patients are considered together. The fluorescence intensities of the CIIFA in NMO patients were significantly higher than those in the other disease groups (Mann-Whitney test, NMO vs. NMOSD, P=0.0026; NMO vs. OND, P<0.0001).
DISCUSSION
In recent years, tests such as CIIFA, radioimmunoprecipitation assay (RIPA), FIPA and ELISA have been developed for the detection of the presence of specific AQP4 antibodies. The cell-based assay (CBA), which utilizes AQP4 expressed on the cell surface in a naturally folded state as an antigen, showed advantages in sensitivity and specificity over NMO-IgG using mouse brain tissue or ELISA using synthesized recombinant peptide or protein [15, 18, 20, 21]. Subsequently, in-house CBAs based on different detection principles such as indirect immunofluorescence [20, 22], flow cytometry [23, 24], or cytotoxicity [25] were developed. All of these methods utilize HEK cell lines transfected with full-length recombinant human AQP4 for antigenic preparations, thus providing the naturally folded AQP4 protein as an antigenic target.
Recently, EUROIMMUN AG has introduced the commercially available CIIFA [16]. In our comparison set between the in-house CIIFA and the commercially available CIIFA, we had several discordant results due to an inconclusive fluorescence pattern observed in the in-house CIIFA, which was derived primarily from the poor quality of cellular substrate preparation. In contrast, by using the commercially available kit we completely avoided inconclusive results in 147 samples, including 46 comparison samples and 101 consecutively enrolled patient samples. Nevertheless, the preparation of transfected cells as an antigenic source in the CBA might have caused the variation of results. Test kits manufactured under standardized conditions may improve the consistency of in-house test preparation. In our prospective cohort in which we evaluated the clinical usefulness of CIIFA, AQP4 antibodies were present in 100% (6/6) of patients with NMO and 23% (8/35) of high-risk NMO such as LETM and BON/RON patients, but was virtually absent in patients with MS and other inflammatory and non-inflammatory neurological diseases with the exception of 1 patient with an autoimmune disease and 2 CIS patients. Considering the differences in diagnostic criteria, the study design (i.e., whether patients and sera were acquired consecutively on a clinical basis rather than selected from a pool of known cases and controls), and the test method, direct comparisons of diagnostic values of AQP4 antibody tests reported in other studies may not be applicable. However, the sensitivity of the CIIFA used in this study was superior compared to those of other studies, such as 91% sensitivity reported by Takahashi et al. [18, 22] and 73% sensitivity reported by McKeon et al. [26]. More importantly, the specificity of CIIFA for detection of AQP4 antibodies was excellent (94%), thus the clinical relevance of this test in the discrimination of NMO from MS and other demyelinating diseases was significant.
NMOSDs have been reported in patients with systemic connective-tissue diseases such as systemic lupus erythematosus (SLE) or Sjögren's syndrome [27, 28]; of note, autoantibody markers of SLE or Sjögren's syndrome are found in almost 40% of patients with NMO and high-risk NMO [14]. However, AQP4 antibodies are not present in patients with systemic connective-tissue diseases in the absence of CNS involvement or with CNS involvement other than NMO [29]. In our study, 4 Sjögren's syndrome patients were diagnosed with NMO and LETM (1 patient) and high-risk NMO (3 patients), and 3 of these patients had AQP4 antibodies. Min et al. reported that 75% of Sjögren's syndrome patients with recurrent brain lesions had AQP4 antibodies and met the criteria for NMOSDs such as NMO in Korean patients with Sjögren's syndrome [30].
FIPA has been developed by using the principle of an immunoprecipitation assay for routine use and quantitative measurement of AQP4 antibodies [20]. Detection of AQP4 antibodies using FIPA was reported to have comparable sensitivity and specificity and correlate highly with the results of CBAs [15, 20]. The concordance between FIPA and CIIFA performed at our hospital was 86-100%, depending on the diagnosis. The AQP4 antibody level detected by FIPA and titers detected by CIIFA derived from the dilution factor of the patient sera were proportional and had a tendency to correlate well with each other. Since the in vivo pathogenic role of AQP4 antibodies (which are predominantly of the IgG1 subclass and activate complement after binding to extracellular epitopes) is well described [20, 21], the quantitative measurement of AQP4 antibodies may provide insight into the clinical course and treatment response of AQP4 antibody-related diseases. Serial measurements of the AQP4 antibody level by FIPA to monitor the treatment response or relapse during the clinical course have been reported [18, 29, 31]. Takahashi et al. [18] observed that the AQP4 antibody titer was related to spinal cord lesion length and Jarius et al. [31] noted that antibody levels were higher if serum samples were obtained during a relapse and before commencement of immunosuppression. However, in spite of these potential applications, the establishment of in-house FIPA is quite problematic since there are several steps that can cause variability during the test procedure. In particular, the preparation of antigenic material in each batch of test includes multiple procedures such as maintenance of HEK cell lines, preparation of the transfecting vector and DNA, transfection, and cell lysate processing. Moreover, establishment of a cut-off point is arbitrary in each laboratory, thus the transferability of quantitative data is limited, and there is no standardized control material to validate the quantitative value generated from each test. In this respect, CIIFA, a CBA using indirect immunofluorescence principles has several advantages over FIPA. First, the antigenic material prepared on slides can be manufactured on a large scale and stored for a relatively long duration of time. Second, the test procedure is conventional IIFA, which is widely performed in clinical laboratories. Third, the interpretation of fluorescence intensity is a standardized concept among clinical pathologists.
In this study, we demonstrated that the commercially available CIIFA was well correlated with FIPA for the detection and quantitation of AQP4 antibodies, and exhibited a high sensitivity and excellent specificity for the diagnosis of NMO and high-risk NMO diseases. Nevertheless, the usefulness of titration of CIIFA for the prediction of the extent of spinal cord lesions and monitoring of disease progression or treatment response needs to be actively investigated in a prospective study on a larger scale.




 XML Download
XML Download