

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
For patients with chronic kidney disease, kidney transplantation is preferred over dialysis, because of the significantly superior survival rates of kidney transplantation. However, many patients are unable to receive transplants due to ABO mismatch. In Korea, patients awaiting kidney transplantation numbered 8,488 in 2009, and only about 15% of these patients received kidney transplantation [1]. If ABO-incompatible kidney transplantations were possible, many more kidney transplantations could be performed.
To overcome the ABO incompatibility barrier, trials have attempted to prevent the ABO antigen-antibody reactions to the graft. To prevent attack of anti-A/B antibodies on graft antigens, anti-A/B antibody titers of the recipient must be reduced. Many reports on ABO-incompatible kidney transplantation have described the removal of anti-A/B antibodies using therapeutic plasma exchanges (PEs). For removing anti-A/B antibodies, removal of a recipient's plasma through PE is reasonable. However, despite the historic and wide usage of therapeutic apheresis, controlled clinical trials on PE for ABO-incompatible kidney transplantation have not been conducted [2]. In previous years, desensitization protocols involving splenectomy to induce a reduction in lymphoid mass and enhance efficacy of immunosuppressive medications were developed [3]. However, adverse effects and suboptimal efficacy were noted after splenectomy. Currently, studies are being conducted on the use of PE and intravenous immunoglobulin (IVIG), along with immunosuppressants, but without splenectomy [4]. This study reports 12 cases of ABO-incompatible kidney transplantation that received PE followed by IVIG and immunosuppressant administration.
METHODS
1. Patients
Between June 2010 and May 2011, 12 patients received kidney transplantations from ABO-incompatible living donors at the Yonsei University Health System (YUHS), which is affiliated with Severance Hospital, Seoul, Korea. These patients had end stage renal disease and were unable to find ABO-compatible donors; however, each of them had a family member who intended to donate his or her kidney. All patients received pre-transplantation conditioning prior to the operation. Results of the HLA crossmatch test that included testing of the antihuman-globulin phase were negative for all patients.
2. Protocol for pre-transplantation conditioning
We used the conditioning protocol illustrated in Fig. 1, as previously reported [5]. The YUHS protocol consists of PE followed by IVIG (100 mg/kg) and immunosuppressants (tacrolimus 0.1 mg/day, mycophenolate 1,500 mg/day, prednisone 20 mg/day, rituximab 375 mg/m2) administration. The medical staff explained the pre-transplantation conditioning protocol to all patients, and all patients provided informed consent for the protocol. PE was conducted using the COBE spectra system (Gambro BCT, Lakewood, CO, USA) for the patients who had anti-A/B antibody titers greater than 1:8. One plasma volume was removed from each patient, and 100% replacement was provided using a 5% albumin solution and fresh frozen plasma (FFP) of AB blood group. PE and IVIG treatments were conducted every other day before transplantation until both IgM and IgG titers were under 1:8. PE was performed with 5% normal serum albumin for the initial sessions, and the last 2 sessions of PE were carried out with AB blood group FFP. Immunosuppressive drugs were used before transplantation to prevent graft rejection. Administration of tacrolimus, mycophenolate, and prednisone was initiated 7 days prior to transplantation, and administration of rituximab was performed 2 days before transplantation. Splenectomy was not included in the conditioning protocol.
3. Measurement of anti-A/B antibody titers
Anti-A/B antibody titers were determined by testing two-fold serial dilutions of the patients' serum with commercially available A/B indicator red cells [6]. The highest serum dilution ratio that showed 1+ reactivity indicated the anti-A/B antibody titers. IgG titers were measured using serum samples treated with dithiothreitol, while IgM titers were determined from untreated samples. Antibody titers were evaluated every day after initiation of the conditioning protocol.
4. Estimated glomerular filtration rate and proteinuria
Graft function was evaluated by considering the estimated glomerular filtration rate (eGFR) and level of proteinuria. Serum creatinine levels were measured by the Jaffe method on a Hitachi 7600-210 autoanalyzer (Hitachi Co. Ltd., Tokyo, Japan) using Daiichi creatinine (Daiichi Pure Chemicals Co. Ltd., Tokyo, Japan). eGFR was estimated from the serum creatinine levels using the abbreviated Modification of Diet in Renal Disease formula [7]. Renal function after the operation was categorized into the immediate recovery of graft function (IGF) or slow recovery of graft function (SGF) group on the basis of the eGFR on post-transplant day (POD) 14. Delayed recovery of graft function (DGF) was defined as the need for dialysis within 7 days after transplantation. The level of proteinuria was measured by the semiquantitative method using an automated urine analyzer. The reflectance of the surface of URiSCAN Super test strips (YD Diagnostics, Yongin, Korea) was evaluated using a reflectance photometer after the strip was reacted with the patients' urine samples.
RESULTS
1. Characteristics of recipients and donors
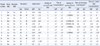
Information on the recipients is provided in Table 1. Of the 12 recipients, 7 were women and 5 were men. The median age of the recipients was 51 yr (average age, 48.75 yr; range, 23-60 yr). All patients received major ABO-mismatched grafts, with no weak ABO subgroups among the donors. No patient showed hyperacute rejection after transplantation, and loss of grafts did not occur during the hospitalization period.
2. Anti-A/B antibody titers
Anti-A/B antibody titers were recorded on the day before initiation of PE and IVIG administration, the day of transplantation, the time of discharge from hospital, and at 1 month after transplantation (Table 1). The initial anti-A/B antibody titers of the patients were 1:8-1:128, and the titers decreased in response to PE and IVIG administration to 1:8 in all patients. The average number of pre-transplantation PE and IVIG treatments was 4.0±0.89 (range 3-5). In general, the higher the initial antibody titer, the greater the number of pre-transplantation treatments required. However, patient 2 needed 5 treatments of PE and IVIG before transplantation due to a low response to treatment.
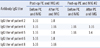
Most of the patients' antibody titers at the time of discharge from hospital were higher than the titers at transplantation but lower than their initial titers. Post-transplantation PE and IVIG treatment was performed with 5% albumin solution in order to reduce anti-A/B antibody titers to below 1:16 to avoid rejection in 5 patients (patients 2, 4, 5, 6, and 8). In patients 2 and 5, post-transplantation PE and IVIG administration was effective at lowering antibody titers; however, in patients 4 and 8, anti-A/B antibody titers did not respond to PE and IVIG administration. In patient 6, ABO IgG antibody titers were 1:8 after post-transplantation PE and IVIG administration, but were 1:16 at discharge (Table 2).
3. eGFR and proteinuria
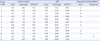
After transplantation, serum creatinine levels, eGFR, and proteinuria showed improvement in all patients. The average creatinine levels at 1 week, 2 weeks, and 1 month after transplantation were 1.30, 1.06, and 1.18 mg/dL, respectively. No patient underwent dialysis after transplantation i.e. no patient showed DGF. The eGFR at POD 14 was computed as over 60 in 10 of the 12 patients, suggesting IGF, while 2 patients (patients 6 and 10) showed eGFR of less than 60, which indicated SGF. Proteinuria due to glomerular damage was negligible in all recipients (Table 3).
DISCUSSION
All patients showed graft success and good decrease in serum creatinine level. The average creatinine level at discharge was 1.13 mg/dL, and the average period from transplant to discharge was 18.25 days. The average creatinine level of patients who underwent ABO-compatible kidney transplantation at YUHS between 1997 and 2002 was 1.86 mg/dL and 1.58 mg/dL at 1 week and 1 month after transplant, respectively [8]. The short-term outcomes of ABO-incompatible kidney transplantation were similar to those of ABO-compatible kidney transplantation.
Since the concept of depleting anti-A/B antibody using PE was introduced to overcome the donor-recipient ABO-incompatibility in kidney transplantation, many trials were conducted for several decades. The outcome of ABO-incompatible kidney transplants has been improved and introduction of tacrolimus/mycophenolate mofetil has been regarded as major factor that made a difference [9]. In Korea, successful outcomes without graft loss were reportd in ABO-incompatible kidney transplants pretreated with PE, tacrolimus, mycophenolate mofetil and rituximab [10, 11]. Compared to IGF, DGF and SGF i.e. poor early graft function is associated with higher rates of acute rejection and impaired renal allograft survival [12]. We predict good prognosis for patients who showed IGF in this study and poor prognosis for patients with SGF, who may require a renal biopsy for diagnosis of rejection.
Antibody-mediated rejection is a significant risk to the survival of patient and graft. Donor-specific anti-HLA antibodies are more closely associated with rejection than anti-A/B antibodies; nevertheless, prevention of immune reactions due to anti-A/B antibodies is crucial for transplant success. ABO antigens are expressed not only on red blood cells but also in various cells such as the endothelial cells of graft organs. ABO-incompatible graft implantation often results in immediate hyperacute rejection, involving failure of graft reperfusion due to thrombosis of the microvasculature [13]. Titers of the anti-A/B IgG antibodies are considered to be more important than titers of IgM. Gloor et al. reported that initial anti-A/B IgG titer of more than 1:256 is significantly associated with the incidence of antibody-mediated rejection [14]. Further, Toki et al. reported that an anti-A/B IgG titer above 1:32 at the time of transplantation is an independent risk factor for antibody-mediated rejection [15]. In this study, patient 6 and patient 11 had the highest initial anti-A/B IgG titers (1:128) and had the lowest eGFR at 50.44 and 44.00, respectively.
PE is used to reduce titers of anti-A/B antibodies, but PE does not eliminate only the anti-A/B antibodies in the plasma. Along with antibodies, plasma constituents are also removed by PE. Theoretically, one-volume PE should lead to removal of 70% of the substances in plasma [16], but actually, efficiency of PE is lowered due to the movement of extravascular substances to the intravascular compartments and resynthesis of plasma substances [17].
Accordingly, 5% albumin solution and AB blood group FFP were used as replacement fluids during PE. Use of albumin involves a minimal risk of infectious disease and rarely causes any allergic reaction. For removing plasma substances without causing any deficits in the plasma, albumin is the most appropriate replacement fluid. Usually, albumin is preferred to FFP because compared to albumin, FFP is associated with higher risk of hypersensitivity reactions and transmission of viral infections [18]. However, in this study, the last 2 PEs immediately before the transplantation were performed with FFP to supply coagulation factors to the patients in order to assuage the worry of surgeons concerning bleeding during operation. Furthermore, soluble ABO antigens present in the FFP can neutralize recipients' isoagglutinins. Therefore, FFP, as a replacement fluid, can possibly help to reduce the recipient's anti-A/B antibody titers [17].
IVIG administration can play a role in the reduction of antibody titers, but the exact mechanism is not well defined. It is thought that IVIG suppresses the rebound of antibody titers right after PE. In addition, IVIG is administered after PE to prevent excessive hypogammaglobulinemia.
Post-transplantation PE and IVIG treatments were related to successful renal transplantation during the study period; this may be attributed to a decrease in anti-A/B antibody titers. Lowering the anti-A/B antibody titers by PE and IVIG administration prevented aggravation of antibody-mediated rejection, allowing for successful renal graft functioning. In this study, 5 out of the 12 patients underwent post-transplantation PE and IVIG treatment. Table 2 shows the changes in anti-A/B antibody titers before and after post-transplantation PE and IVIG treatments. Among these 5 patients, 3 patients (patients 2, 5, and 6) showed a decrease in antibody titers after post-transplantation PE and IVIG treatment, but the antibody titers of patient 6 increased right before discharge from hospital. As a result, only 2 patients showed IgG titers within the target range at the time of discharge. Patients 4, 6, and 8 had high ABO IgG titers and required a more number of pre-transplantation PE and IVIG treatments than the other 2 patients. The degree of response to pretransplantation PE and IVIG treatment appeared to be associated with the degree of response to post-transplantation PE and IVIG treatment.
PE is currently considered as a supportive therapy for ABO-incompatible kidney transplantation. Procedures that remove a recipient's anti-A/B antibodies are essential for ABO-incompatible kidney transplantation. Protocols for pre-transplantation desensitization should include antibody removal process. PE may help overcome the barrier of ABO incompatibility by removing the recipient's natural antibodies against the donor's A and/or B blood group antigens. We suggest that PE be considered as a primary therapy for ABO-incompatible kidney transplantation.

 XML Download
XML Download