

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Methicillin-resistant Staphylococcus aureus (MRSA) is a major cause of skin, wound, soft tissue, respiratory, and endovascular infections as well as a leading cause of hospital-acquired infections. Many outbreaks of S. aureus have been reported, and some have been traced to environmental sources [1-3]. The transmission of MRSA is presumed to occur through contact with a common reservoir of environmental contamination, including computer keyboards, faucets, door handles, floors, bed linens, patient gowns, and blood pressure cuffs [1, 2, 4].
In many hospitals, portable radiological studies are routinely performed on patients in wards or intensive care units. Even before the emergence of the antimicrobial resistant organisms, there were reports of contaminated patients coming into contact with medical devices used in radiology departments [5, 6]. A study from the late 1960s showed that staphylococci, coliform bacteria, and molds contaminated the surfaces of X-ray equipment contacted by patients, such as chest racks, chin supports, and X-ray tables [5]. However, the contamination of X-ray cassette surfaces by antimicrobial-resistant microorganisms, such as MRSA, has not yet been examined. The present study was performed to determine whether the surfaces of X-ray cassettes contacted by patients were contaminated with MRSA. In addition, the clonal relationships of isolates were analyzed using pulsed-field gel electrophoresis (PFGE). While screening for MRSA, we also identified heavy contamination of X-ray cassette surfaces with methicillin-resistant Staphylococcus haemolyticus (MRSH). MRSH is a mannitol-fermenting, coagulase-negative staphylococcus whose colonies resemble MRSA on mannitol salt agar containing oxacillin.
METHODS
1. Bacterial isolation
Thirty-seven X-ray cassettes from the radiology department of a tertiary-care hospital were evaluated for MRSA contamination. Vertically stacked cassettes in the radiology department were sequentially sampled for cultures. For each X-ray cassette, the entire patient-contacting surface, which was made of polyvinyl chloride, was wiped with a cotton swab moistened with sterile normal saline. The screening swabs were inoculated on mannitol salt agar containing 6 µg/mL of oxacillin (MSO), and the plates were incubated at 35℃ for 48 hr. From each MSO plate, 1-3 yellow colonies suspicious for MRSA were subcultured on blood agar plates. Gram stains were performed from pure cultures of the isolates. All gram-positive cocci were tested for coagulase, DNase, and growth on mannitol salt agar. Isolates were identified using the MicroScan WalkAway system (Dade Behring, Sacramento, CA, USA). Antimicrobial susceptibility was determined by disk diffusion testing, and the results were interpreted using the Clinical and Laboratory Standards Institute breakpoint criteria [7]. In addition, PCR-based tests on the mecA gene were performed to confirm the identification of MRSA.
2. PFGE
For each cassette yielding positive cultures, 1 isolate was selected for analysis by PFGE. PFGE was performed as previously reported [8] with some modifications, including prolonged times for plug digestion and washing. Plugs were digested in a total of 100 µL of restriction enzyme buffer and 20 U of SmaI (New England Biolabs, Beverly, MA, USA) at 25℃ for 6 hr. Electrophoresis was performed using the CHEF Mapper system (Bio-Rad Laboratories, Hercules, CA, USA) in 0.5×Tris-borate-EDTA buffer. Migration conditions were as follows: temperature, 14℃; voltage, 6 V/cm; switch angle, 120°; and one linear switch ramp of 5-40 sec for 20 hr. PFGE patterns were analyzed using BioNumerics software (Applied Maths BVBA, Sint-Martens-Latem, Belgium).
RESULTS
MRSA was isolated from 6 of the 37 X-ray cassettes (16.2%). Of the 6 contaminated X-ray cassettes, 4 (samples 1, 2, 3, 4) were adjacent to each other, and another 2 (samples 22, 23) were adjacent to each other while stored in the radiology department. Of the 4 adjacent X-ray cassettes, 2 cultures (samples 3, 4) yielded more than 100 colonies, and the remaining 2 cultures (samples 1, 2) yielded 3 and 20 colonies, respectively. The cultures of the other 2 adjacent X-ray cassettes each yielded less than 5 colonies.
During strain identification, some colonies suspicious for MRSA on MSO were determined to be coagulase-negative staphylococci. Nearly all of these coagulase-negative staphylococci were identified as MRSH. MRSH was isolated from 19 of the 37 X-ray cassettes (51.4%). Fourteen of the cultures yielded less than 10 colonies; 2 cultures yielded 10-50 colonies, and the remaining 3 cultures yielded 50 or more colonies of MRSH. One cassette was contaminated with 2 colonies of S. capitis, a mannitol-fermenting coagulase-negative staphylococci.
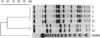
Among the MRSA contaminants (N=6), PFGE analysis revealed 2 major pulsotypes (Fig. 1). An identical PFGE pattern was observed in 4 isolates (samples 1, 3, 4, and 22), and a second identical pattern was observed in 2 isolates (samples 2 and 23). Among the MRSH contaminants (N=19), PFGE analysis revealed 2 major pulsotypes (Fig. 2); a single identical PFGE pattern was observed in 11 isolates (samples 5-9, 13, 14, 17, 19, 24, and 25) and another was observed in 5 isolates (samples 15, 16, 20, 21,and 26).
DISCUSSION
The principal mode of MRSA transmission within a hospital is from patient to patient via transient colonization of hospital personnel's hands, which acquire the organism from direct patient contact or handling contaminated materials [9]. Furthermore, during radiology procedures, contact can occur between contaminated X-ray cassettes and a patient's clothing and skin or the radiology technician's hands. The role of inanimate objects in clinical infections is controversial, and there is little evidence demonstrating that decreasing environmental MRSA contamination lowers the rates of patient infection [10, 11]. However, the patient environment is considered to be a potential fomites for infection, and contamination of the hospital environment with multi-resistant bacteria can be controlled [10, 12].
The importance of reducing contamination in the hospital environment remains unclear. However, 2 of the 37 X-ray cassettes were heavily contaminated with MRSA, which could increase the risk of transmission within the hospital, such as to elastic bandages for wound care, patient's skin, and the hands of radiology personnel.
The 6 MRSA isolates and 19 MRSH isolates each showed 2 major pulsotypes. For each organism, the pulsotypes were closely related. These findings suggest that cross-contamination of X-ray cassettes by MRSA and MRSH can result from a few common sources of contamination. Notably, we did not screen the technicians in the department of radiology for MRSA during the study period. Therefore, it is not clear whether the X-ray cassettes became contaminated by the medical personnel's hands or by surface-to-surface contact between the stacked X-ray cassettes.
Although this study identified X-ray cassettes contaminated by methicillin-resistant staphylococci, we could not detect non-mannitol fermenting staphylococci, such as Staphylococcus epidermidis, or other pathogenic bacteria, because we only performed screening using MSO. As such, we cannot exclude contamination with another genus or coagulase-negative staphylococcus. The use of chromogenic medium can provide fast and accurate detection of MRSA contamination in the presence of coagulase-negative staphylococci producing yellow colonies on MSO.
The best method for disinfecting contaminated X-ray cassettes is unclear. In our hospital, the surfaces of X-ray cassettes were disinfected once weekly with a gauze soaked in 70% ethanol. In order to prevent the transmission of microorganisms from contaminated X-ray cassettes to patients, an X-ray cassette cover could be used for patients who are infected or colonized with MRSA and for patients with oozing skin lesions. However, this study did not establish a role for the contaminated X-ray cassettes in the spread of MRSA, and the role of preventive measures requires further investigation. In addition, contamination rates might differ according to the prevalence of MRSA; for instance, the rate of MRSA in bloodstream infections is as high as 70% in Korea, a highly endemic country [13].
With the exception of MRSA isolates from 6 X-ray cassettes, many of the yellow colonies on MSO were identified as MRSH, another mannitol fermenting staphylococcus. Although less virulent than S. aureus, S. haemolyticus has been associated with septicemia and skin and soft-tissue infections [14, 15]. PFGE analysis demonstrated that most MRSH isolates in this study were identical or clonally related. This finding suggests that S. haemolyticus can spread in the hospital environment via medical devices, as reported in other studies using PFGE [16, 17].
In conclusion, we demonstrated that patient-contact surfaces of X-ray cassettes were contaminated with MRSA and MRSH. PFGE patterns indicated that these methicillin-resistant staphylococci were clonally related. Because X-ray cassettes are possible fomites for the transmission of MRSA and other pathogens, the application of contamination barriers or decontamination procedures should be considered.

 XML Download
XML Download